
Abstract
Summary: When standard transarterial or transvenous interventional techniques failed to provide access to treat an indirect carotid cavernous fistula, we used sonographically guided direct percutaneous access through the facial vein to successfully embolize a lesion.
Treatment options for carotid cavernous fistulas (CCFs) include manual carotid artery compression, transarterial endovascular embolization, radiation therapy, and transvenous embolization (1–9). Multiple authors have identified transvenous embolization as the treatment of choice (1, 6).
We performed a sonographically guided puncture of the facial vein to provide access to the superior ophthalmic vein (SOV) and to the cavernous sinus and successfully embolized an indirect CCF with a combination of Guglielmi detachable coils (GDCs) and an n-butyl-2-cyanoacrylate (NBCA) injection.
Case Report
A 78-year-old white female patient was referred to the interventional neuroradiology (INR) service for increasing proptosis in the left eye. The patient also reported headache and partial loss of vision in the left eye. Physical examination revealed marked proptosis and congestion of the left eye with partial ophthalmoplegia. Pupils were symmetric, and pupillary reflexes were preserved. Neurologic examination was otherwise unremarkable.
The patient previously had six sessions of embolization, during which multiple arterial feeders and the right cavernous sinus were embolized. The last embolization session was 8 months before this admission.
After the patient gave informed consent, she was transferred to an INR suite. Under general anesthesia, the right common femoral artery and left common femoral vein were accessed, both with 6F vascular sheaths; 5000 U of intravenous heparin was administered.
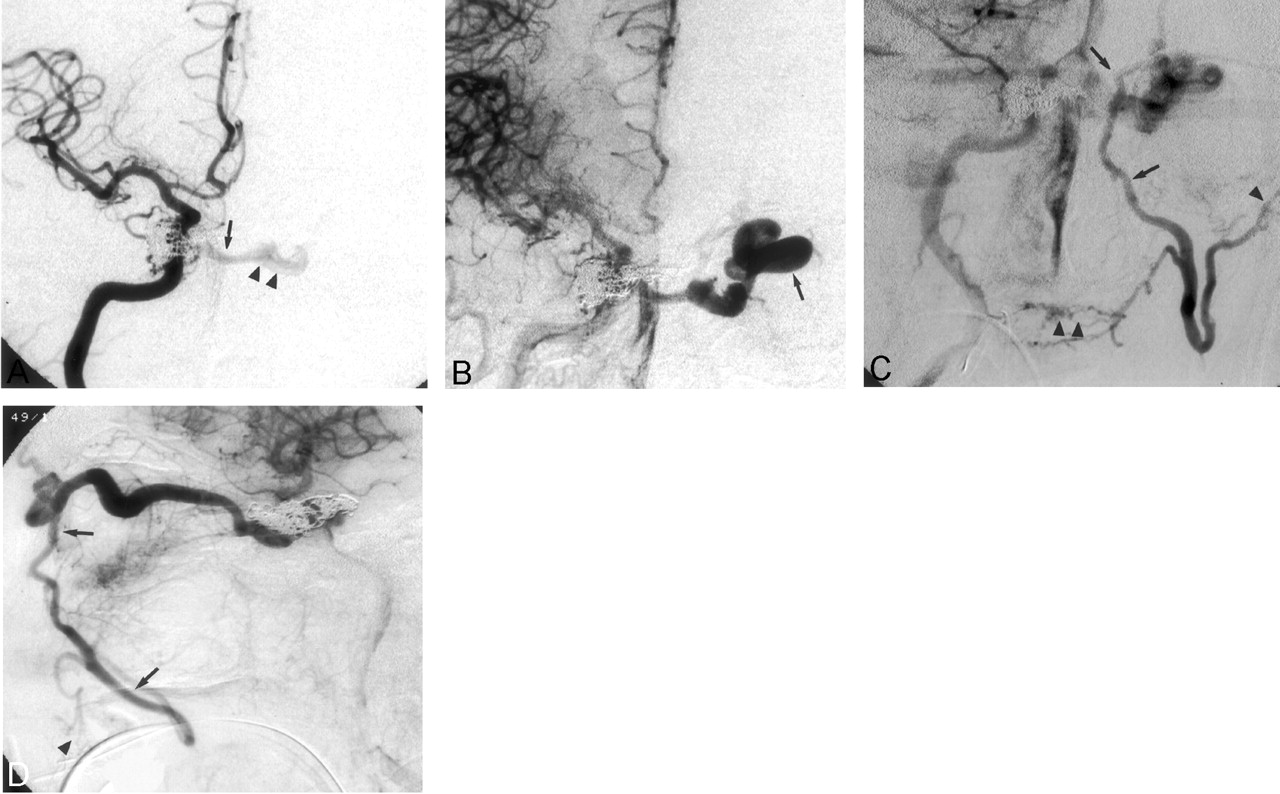
A cerebral arteriogram showed a persistent indirect CCF on the right, flowing despite multiple GDCs within the cavernous sinus from prior embolization (Fig 1). The fistula was supplied by dural and cavernous branches of the right internal carotid artery (ICA) and drained via the circular sinus to the contralateral cavernous sinus and from there to the left SOV and left facial vein, which were prominent (Fig 1). There was no cortical venous drainage. The left facial vein appeared to terminate in a web of small collateral veins with no direct connection to any major venous channel (Fig 1C and D). Also of note was a failure to opacify the inferior petrosal sinuses or the right SOV, which may have thrombosed because of prolonged venous hypertension or prior embolization. Injections into the left ICA also faintly opacified the fistula and confirmed these findings. No other arterial feeders were depicted on bilateral external carotid artery (ECA) or vertebral artery injections.

A, Selective right internal carotid arteriogram (frontal view) shows an indirect right CCF with flow through the circular sinus (arrow) cross-filling the left cavernous sinus (arrowheads). There are coils within the right cavernous sinus from an embolization previously attempted at another institution. B, Later phase of the same injection. A large left SOV is opacified (arrow). C and D, On later phase images (C, frontal view; D, lateral view), the left SOV drains toward the left angular and facial veins (arrows). The left facial vein terminates in small collateral channels (arrowheads) and does not directly communicate to the jugular venous system.
At this point, a 6F Envoy guiding catheter (Cordis, Miami Lakes, FL) was placed in the left internal jugular vein just below the craniocervical junction; multiple attempts were made to pass Prowler 14 and Prowler 10 microcatheters (Cordis) over Agility 14 and Agility 10 (Cordis) wires into the inferior petrosal sinus. Although the microcatheters could be passed into a small caliber residual channel of the left inferior petrosal sinus, it was not possible to access the cavernous sinus via this channel. These attempts were repeated from the right side, with similar unfavorable results.
A 5F vertebral catheter (Cordis) was then placed in the right ICA. Injections were made to further evaluate the left facial vein and explore the possibility of catheterizing it via a transfemoral venous approach. These injections, however, confirmed that the left facial vein terminated in a web of small collateral veins in the patient’s face that were not accessible from the transfemoral route. It was also noted that the facial vein was 2 mm in diameter and had a relatively straight course in its infraorbital portion (Fig 1C and D). It was decided to attempt a sonographically guided puncture of the facial vein.
A Site Rite II vascular access sonography unit (Dymax, Pittsburgh, PA) was brought to the INR suite. A brief sonographic examination of the face confirmed visibility of a 2-mm facial vein in the expected location. The vein was identified as an echolucent circular structure with relatively thick walls, presumably from longstanding venous hypertension. It was compressible and also showed some pulsatility. Under sterile conditions, the facial vein was accessed by using real-time sonographic guidance with a 21-gauge micropuncture needle (Cook, Bloomington, IN). Once blood return was seen, a 0.018-inch guidewire was passed into the facial vein until its tip was in the angular vein; a 4F sheath from the micropuncture system (Cook) was placed over the wire (Fig 2A). After the sheath was secured, a heparinized saline flush was started, and contrast medium injection was performed, which confirmed the position of the sheath with its tip near the angular vein and good opacification of the left SOV. A road map was obtained by using the 4F sheath, and a Prowler 14 (Cordis) microcatheter was successfully passed into the SOV over an Agility 14 wire (Cordis) (Fig 2B). A-5 mm GDC coil was deployed in the proximal SOV near its junction to the left cavernous sinus; the catheter was passed through the coil into the left cavernous sinus-circular sinus and into the right cavernous sinus until its tip reached the site of the fistula. From this catheter position, a 60%:40% mixture of NBCA (Cordis) was injected in a controlled fashion, which filled the right cavernous sinus, the fistula, the circular sinus, the left cavernous sinus, and the proximal portion of the left SOV to the level of the GDC coil (Fig 3). Care was taken to preserve as much of the intraorbital left SOV as possible to maintain venous return from episcleral veins. After embolization, injections through the arterial catheter into the right ICA, left ICA, right ECA, and vertebral artery showed complete closure of the fistula, with preservation of flow in all other cerebral branches (Fig 3). The 4F sheath in the left facial vein was removed, and brief manual compression was applied over the puncture site. No complications occurred.

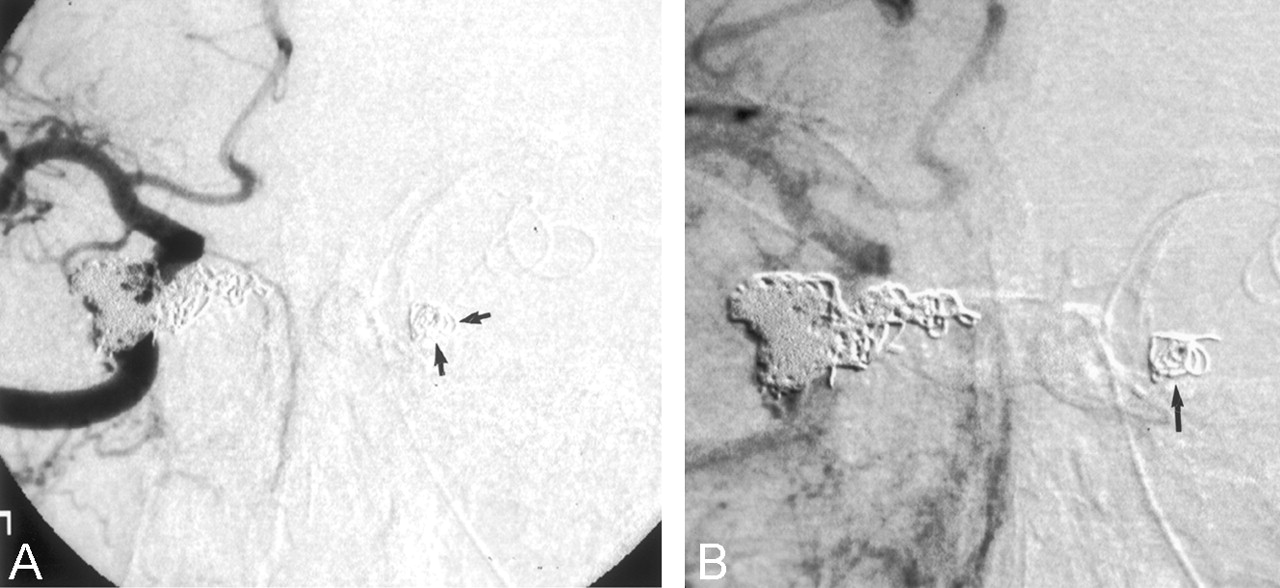
A, The 4F sheath is placed percutaneously inside the left facial vein. Note that the puncture site is well inferior to the left orbit. B, Catheterization of the left SOV (lateral view)

Early- (A) and late-phase (B) images from a right internal carotid injection following embolization with NBCA and GDC. The coil within the left SOV is depicted (arrows), and a completely obliterated CCF can be seen.
The patient recovered fully within the next 24 hours and was discharged home the next day and prescribed 325 mg of acetyl salicylic acid PO q.d. Eight weeks after the procedure, her proptosis and chemosis had completely resolved. She remains asymptomatic.
Discussion
Indirect CCFs are relatively uncommon lesions of unclear cause (1–6). Most patients come to medical attention because of ocular symptoms such as proptosis, chemosis, ophthalmoplegia, glaucoma, and subsequent vision loss (1, 3). Other presenting symptoms include headache, a constant and bothersome pulse, synchronous bruit, and, less commonly, cerebral manifestations such as intracranial hemorrhage from venous hypertension or rupture of coexisting pseudoaneurysms or cerebral ischemia and progressive neurologic deficit from chronic cerebral arterial steal (1). Although spontaneous resolution of CCF has been described, most patients who seek medical attention need treatment (1, 4).
Accessibility of the cavernous sinus to percutaneous transvenous embolization procedures changes as the disease progresses. Difficulties may result from occlusion of the inferior petrosal sinuses from longstanding venous hypertension, from prior embolization, or both. Once the inferior petrosal sinuses are thrombosed, percutaneous access may be carried out via the superior petrous veins or the route of the facial vein, angular vein, SOV, and cavernous sinus route, but these approaches are technically more difficult than the transfemoral venous approach. Many authors have reported their results with surgical access to the angular vein, SOV, Sylvian veins, and even cortical veins (2–9) in an attempt to pass microcatheters into the cavernous sinus for embolization of an indirect CCF. These combined surgical-endovascular approaches are more complex and pose a higher risk to the patient, especially if it involves the catheterization of cortical veins. Direct surgical access also carries the risk of additional morbidity, mortality, and possible undesirable cosmetic results (3).
Percutaneous access to the SOV and cavernous sinus has been performed under fluoroscopic guidance (2), although this approach has its own limitations. The possibility of inadvertently puncturing the eyeball or other vital structures in the tight orbital space is much higher, because only the opacified SOV and the osseous structures are visible. There is also risk of an intraorbital hematoma because of uncontrolled bleeding during the puncture or, if the embolization fails, after removal of the needle (2).
The sonographically guided approach allows access to the facial vein outside the orbit and eliminates the risk of complications, such as intra- or retro-orbital hemorrhage, cranial nerve damage, subarachnoid or intracranial hemorrhage, and arterial damage, which may result from direct puncture of the SOV or the cavernous sinus (2). Further advantages include a reduction in radiation exposure to the patient and to the interventionalist, elimination of the need for operating room time and surgical help, and the ease of manual compression of the puncture site after the procedure.
The limitations of this approach are mostly related to the diameter of the facial vein. One must take into account the fact that successful sonography depends on the skill of the operator; puncturing a 2–3-mm structure requires experience and the right equipment. We were able to access a 2-mm facial vein with a vascular-access sonographic unit and a micropuncture system (Cook). More sophisticated sonographic equipment and expertise may allow successful results with even smaller veins.
Conclusion
Detachable balloons, polyvinyl alcohol particles, absolute alcohol, coils, and NBCA have been used to embolize CCF (10). Indirect CCFs are usually amenable to treatment by coils or NBCA. In the case of our patient, we preferred to use NBCA, because a long segment of venous outflow from the site of the fistula on the right cavernous sinus to the circular sinus, left cavernous sinus, and left SOV was to be embolized. NBCA offered a quick and reliably permanent embolization of these veins with an acceptable margin of safety. One of the potential risks of NBCA embolization in such cases may be dispersion of the agent into the arterial system. This is unlikely, however, because blood flow is in the opposite direction. Other potential problems—such as dispersion of NBCA into the superficial middle cerebral veins, sphenoparietal sinus, or petrosal sinuses—also need to be avoided with meticulous technique and careful monitoring during injection, which should be done in a gentle and controlled fashion. We chose to deploy a single GDC coil in the proximal left SOV to limit the NBCA reflux into the SOV and to serve as a marker to stop the NBCA injection. The microcatheter can easily be advanced through the single coil into the left cavernous sinus, the circular sinus, and subsequently, into the area of the fistula on the right cavernous sinus. A patent SOV might be important as a venous outflow for episcleral venous system. Overall, sonographically guided percutaneous access of the facial vein is easily accomplished and is a safe and effective way to treat an indirect CCF if other routes are not available.
- Received July 29, 2002.
- Accepted after revision March 5, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}