
Abstract
Summary: A self-expanding stent has recently been introduced for the treatment of wide-neck aneurysms. We describe two cases of stent malposition within large aneurysms. In the first case, the stent was dislodged during microcatheterization. This was managed by placement of a second stent through the interstices of the first followed by aneurysm coiling. In the second case, after deployment, the proximal portion of the stent moved into the aneurysm as the exchange guidewire was removed. This patient was treated by vessel sacrifice.
Detachable coils are established as a safe and effective treatment option for some patients with intracranial aneurysms (1). Not all patients are good candidates for endovascular therapy. Wide-neck aneurysms are particularly challenging. Both subtotal aneurysm occlusion with coils and aneurysm recurrence have been associated with large dome-to-neck ratios (2, 3). The balloon remodeling technique pioneered by Moret has given endovascular therapists greater latitude in treating aneurysms with unfavorable neck-to-dome ratios (4). Another approach has been to use a balloon expandable coronary stents to bridge the neck of wide-neck aneurysms (5). These stents are relatively stiff and are not approved for this use by the Food and Drug Administration (FDA).
Recently, the self-expanding Neuroform stent (Boston Scientific/Target Therapeutics, Inc., Natick, MA) has been approved by the FDA specifically for the treatment of wide-neck aneurysms. The stent is constructed of nitinol and has diameters ranging from 2.5 mm to 4.5 mm and lengths ranging from 10 mm to 20 mm. The interstices of the deployed stent vary from 2.0F to 2.5F, allowing the placement of a microcatheter through the stent and into the aneurysm. The radial force exerted by the stent is minimal at 10 mm Hg as compared with the Radius Stent (Boston Scientific, Natick MA) at 36 mm Hg and the Precise Stent (Cordis Endovascular, Miami Lakes, FL) at 140 mm Hg (personal communication David Barry, chief engineer, Smart Therapeutics/Target). Although this property may reduce injury to the vessel wall, it may also allow displacement of the stent after deployment.
In this report, we describe two patients with dislodgement of a Neuroform stent into the target aneurysm with their subsequent management. Both patients had large symptomatic internal carotid artery aneurysms. The initial goal in each was coiling of the aneurysm with preservation of the flow in the carotid artery. In the first case, a second Neuroform stent was placed through the interstices of the original stent. In the second patient, the parent vessel was sacrificed.
Interventions
Patient 1
A 49-year-old female patient presented with severe right retro-orbital headaches. CT of the brain and conventional angiography demonstrated a 12-mm right internal carotid precavernous segment aneurysm that projected into the subarachnoid space at the sella turcica. Endovascular therapy was pursued given the aneurysm location. The appearance of a wide neck on the angiogram caused us to anticipate that a Neuroform stent might be necessary to reconstruct the artery before coil placement.
The procedure, including the possible use of the Neuroform stent, was explained to the patient. Signed informed consent was obtained for the procedure and for the Neuroform device (under a humanitarian device exemption). Plavix (clopidogrel bisulfate, Bristol-Meyers Squibb, Sanofi Pharmeceuticals Partnership, New York, NY) 75 mg/day was started 5 days before the procedure. Aspirin at a dose of 325 mg/day was also initiated 5 days prior to the intervention.
Following induction of general anesthesia, a 6F sheath was placed in the right common femoral artery. A 5F Envoy guiding catheter was advanced into the right internal carotid artery. Digital subtraction angiographic images were obtained, demonstrating a 12-mm precavernous segment right internal carotid aneurysm that projected medially. Multiple obliquities were obtained, although the aneurysm neck could not be projected separately from the parent vessel and the aneurysm.
The patient was anticoagulated with a 6000-U bolus and 600-U/h drip of intravenous heparin (USP, Wyeth-Ayers & Co., Philadelphia, PA). The activated clotting time (ACT) was maintained between 250 and 300 seconds.
Biplane road mapping was used to navigate a 4.5-mm × 15-mm Neuroform stent over a Transcend 10 guidewire (Boston Scientific/Target Therapeutics) into a position straddling the right internal carotid artery precavernous segment aneurysm. The stent was deployed over the neck of the aneurysm in satisfactory position.
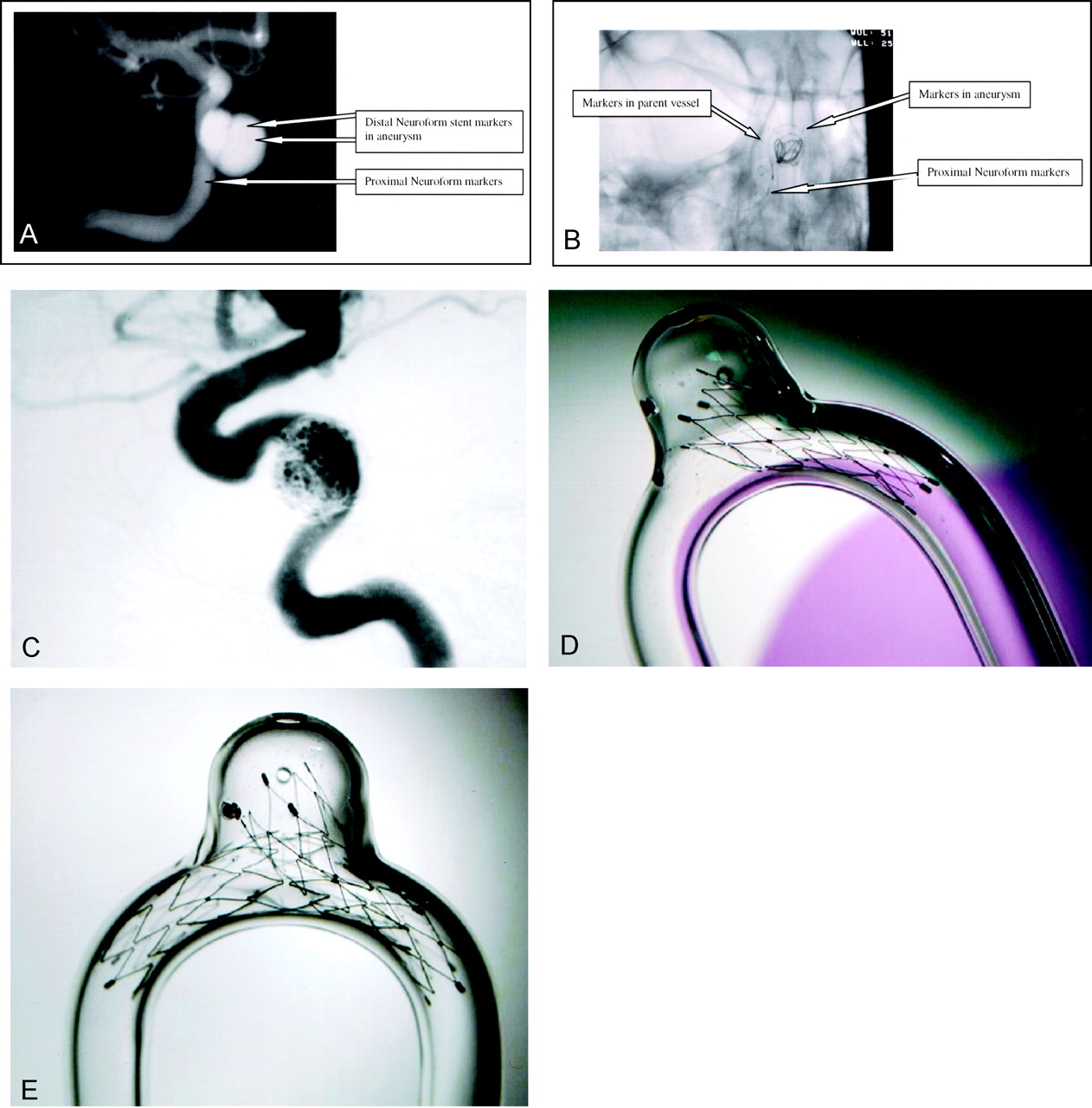
A Prowler Plus microcatheter (Cordis Endovascular) and a Transcend 14 microwire (Boston Scientific/Target Therapeutics) were used without success to access the aneurysm through the interstices of the stent. A Prowler 14 microcatheter and Transcend 14 microwire was then used to access the aneurysm through the interstices of the stent. Digital subtraction angiograms demonstrated that the distal stent markers had been displaced into the aneurysm (Fig 1A). A Guglielmi detachable 10 standard 10-mm × 30-cm coil (Boston Scientific/Target Therapeutics) was advanced through the Prowler 14 catheter into the aneurysm. The coil loops herniated past the stent and into the parent vessel. Therefore, the coil was removed.

Patient 1.
A, Anteroposterior right internal carotid arteriogram showing the aneurysm with the displaced stent.
B, Anteroposterior radiograph showing markers of the two stents: the porximal markers are in the carotid artery, the distal markers of the second stent are in the parent artery distal to the aneurysm. The first coil has been deployed and is about to be detached.
C, Lateral right ICA at the completion of coiling shows filling of the center of the aneurysm.
D, Aneurysm model with the end of the stent displaced into the aneurysm.
E, Aneurysm model with a deployed second stent through the first stent without narrowing of either stent.
After review of the options, it was decided that a stent could be placed through the stent already in place. The appropriate stent was not available, so this procedure was scheduled for a future date. The patient continued to receive aspirin 325 mg/day and Plavix 75 mg/day.
The patient returned for elective treatment approximately 2 months later without new interval symptoms. After placement of a 6F sheath in the right common femoral artery, a temporary balloon occlusion test was performed to evaluate for adequate collateral flow in the event that vessel sacrifice was required. Following inflation of the balloon in the right internal carotid artery, the patient developed left-sided hemiparesis and neglect. This was considered a clinical failure, and the balloon was deflated. The patient returned to her baseline status.
General anesthesia was then induced, and a 5F Envoy guide catheter was placed in the distal cervical right internal carotid artery. The patient received a bolus of intravenous heparin, and a heparin drip was titrated to maintain the ACT between 250 and 300 seconds for the procedure.
Digital subtraction angiography was performed to obtain a working projection. Using road-mapping guidance, a Prowler 14 microcatheter and Transcend 14 microwire were then advanced through the previously placed Neuroform stent and into the proximal middle cerebral artery (MCA). A 300-cm exchange length Transcend 14 microwire was advanced through the microcatheter into the proximal MCA, and the Prowler 14 was removed.
The 4.5 × 20-mm Neuroform stent was loaded into a Renegade HI-FLO catheter (Boston Scientific/Target Therapeutics) by using the following technique: after the tip of the Neuroform nonbraided delivery catheter was placed into the hub of the Renegade microcatheter, the Neuroform stent was pushed to the tip of the Renegade by using the Neuroform stabilization tube and a reverse-mounted Transcend 10 microwire (Boston Scientific/Target Therapeutics) for increased stiffness.
The Renegade microcatheter containing the Neuroform stent was advanced over the 300-cm Transcend guidewire through the previously placed stent. The guidewire was removed, and the stabilizer tube and Transcend guidewire combination was used to deploy the stent from distal to proximal.
A Prowler 14 microcatheter and Transcend 14 guidewire were used to access the aneurysm through the interstices of the stents (Fig 1B). Ten Matrix coils (Boston Scientific/Target Therapeutics) totaling 124 cm in length were deployed within the aneurysm. Coiling was terminated when the microcatheter backed out of the aneurysm. Several unsuccessful attempts were made to reenter the aneurysm with a Prowler 10 microcatheter (Cordis Endovascular) to continue coiling. Digital subtraction angiographic images after coiling showed filling of the medial portion of the aneurysm (Fig 1C). Optimal packing of the aneurysm may have been limited by displacement of the initial stent into the aneurysm. The patient was discharged from the hospital in good condition.
Patient 2
A 32-year-old female patient with severe headaches and left facial pain was found to have a 12-mm left internal carotid artery cavernous segment aneurysm at MR and CT imaging. A balloon test occlusion was performed. The patient passed a 30-minute temporary balloon occlusion test clinically and by relative cerebral blood flow perfusion scanning by using Tc99 m bicisate tomographic imaging. We planned to attempt to preserve the vessel by means of stent-assisted coiling of the aneurysm, with sacrifice only if that approach failed.
The procedure including Neuroform stent placement and possible vessel sacrifice was explained to the patient and signed consent was obtained. Plavix 75 mg/day and aspirin 325 mg/day were initiated 5 days before the procedure.
Following induction of general anesthesia, a 6F sheath was placed in the right common femoral artery and a 5F sheath was placed in the left common femoral artery. A baseline ACT was obtained, and intravenous heparin was administered to maintain the ACT at approximately 300 seconds.
A 5F guide catheter was placed in the left internal carotid artery, and a working projection was obtained. A Prowler 14 microcatheter and Transcend 14 microwire were navigated into the proximal left MCA. This was accomplished with significant difficulty because of the large neck of the aneurysm and the angle between the aneurysm and the distal carotid artery. The Transcend microwire was then exchanged for a 300-cm 0.010-inch Transcend microwire, and the Prowler 14 was removed. A Neuroform 4.5-mm × 20-mm stent had been preloaded into a Renegade HI-FLOW braided microcatheter (Boston Scientific/Target Therapeutics). The device was advanced over the 300-cm Transcend 10 microwire into an optimal position bridging the neck of the aneurysm. The stent was deployed from distal to proximal, but the proximal portion of the stent herniated into the aneurysm when the guidewire was removed (Fig 2A and B). Although some foreshortening likely occurred, the length of the neck may have required more rigid scaffolding than the Neuroform could provide in this situation, because movement of the stent did not occur until the exchange length wire was withdrawn. Because of the difficulty catheterizing the vessel distal to the aneurysm without herniating the system into the aneurysm, vessel sacrifice was deemed to be the safest and most effective option.

Patient 2.
A and B, oblique left internal carotid arteriogram showing the distal markers of the stent in the ICA and the proximal markers of the displaced stent within the large artery.
A 7F standard occlusion balloon catheter (Boston Scientific/MEDI-TECH; Natick, MA) was used for carotid flow arrest, and a Prowler Plus microcather was advanced into the petrous segment of the left internal carotid artery. A total of 25 Tornado coils were deployed to achieve vessel occlusion. The patient suffered a transient ischemic event after the procedure but made a full recovery.
Discussion
The Neuroform stent is a new tool for treatment of wide-neck aneurysms. One limitation of this device is the potential for movement of the stent after deployment. This may be attributed to the minimal radial force exerted by the stent against the vessel wall. In this report, we describe two patients in whom either the distal or proximal end of the stent was dislodged or misplaced into the target aneurysm.
The manufacturers recommend that the Neuroform stent extends 4 mm proximal and 4 mm distal to the aneurysm neck to achieve stability. The amount of stent foreshortening is reported to be 1.8–5.4%. In both patients, the stent markers seemed to indicate an appropriate amount of parent vessel overlap. In the first patient, we used a 15-mm stent—the longest available to us at that time. A longer stent may have provided more stability. In the second patient, the proximal end of a 20-mm stent moved into the target aneurysm when the exchange length wire was withdrawn after deployment. Currently, the maximal length available is 20 mm. In the future, 30-mm Neuroform stents will be available. Longer stents, however, may present greater difficulty in placement, especially around tortuous anatomy.
There are several options that may be pursued once a stent has dislodged. Parent vessel sacrifice may be considered if the collateral circulation is adequate, as in the case of the second patient. In the first patient, however, sacrifice of the parent vessel was not an option, because she failed the temporary balloon occlusion test. In this patient, we proceeded with placement of a second stent that passed through the interstice of the first stent and continued into the distal parent artery. Before we used this technique, this approach was investigated (personal communication, Aaron Berez, MD, SMART Therapeutics/Target) in an in vitro model (Fig 1D and E) by using this technique to treat our patient. The attachment of the rings of the stent facilitates this, because there are only two points of attachment between cells allowing the stent to swing open at each segment. Ideally, this should avoid development of a waist in the second stent as it deploys through the first stent.
It would seem that overlapping stents could be placed if the proximal portion of the first stent is stable in the parent artery and the exchange length wire is maintained across the aneurysm with its tip securely in the vessel distal to the aneurysm. Proximal misplacement of the stent in our second patient made the option of placing a second stent more difficult; therefore, vessel sacrifice was performed.
Conclusion
The Neuroform stent allows endovascular therapists to treat some difficult wide-neck aneurysms. Misplacement of the stent into the target aneurysm during deployment or by dislodgement during catheterization is a potential complication. This impediment may be avoided by deploying longer stents for increased stability. If the complication occurs, it may be successfully managed by parent vessel sacrifice or by placing a second stent through the interstices of the first stent.
- Received April 30, 2003.
- Accepted after revision May 31, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Bailout stentectomy of 47 self-expandable intracranial stents
- Double stent assisted coiling of intracranial bifurcation aneurysms in Y and X configurations with the Neuroform ATLAS stent: immediate and mid term angiographic and clinical follow-up
- Stent-Assisted Coiling in Endovascular Treatment of 500 Consecutive Cerebral Aneurysms with Long-Term Follow-Up
- Technical, angiographic and clinical outcomes of Neuroform 1, 2, 2 Treo and 3 devices in stent-assisted coiling of intracranial aneurysms
- X-configuration intersecting Enterprise stents for vascular remodeling and assisted coil embolization of a wide neck anterior communicating artery aneurysm
- Reconstructive Endovascular Treatment of Intracranial Fusiform Aneurysms: A 1-Stage Procedure with Stent and Balloon
- Bailout Stent Deployment during Coil Embolization of Intracranial Aneurysms
- Interventional Neuroradiology