
Abstract
BACKGROUND AND PURPOSE: Recent advances in the display of medical images permit the routine study of temporal bone CT images at high magnification. We noted an unfamiliar structure, which we now call the “cochlear cleft,” in the otic capsule. To our knowledge, this report represents the first description of this structure in the medical imaging literature.
METHODS: Temporal bone CT performed in 100 pediatric patients without sensorineural hearing loss were examined for the presence of cochlear clefts. Incidence of cochlear clefts as well as the relationship between age and incidence was examined.
RESULTS: Cochlear clefts were present in 41% of the subjects. Incidence decreased with age.
CONCLUSION: We describe a cleft in the otic capsule that is frequently seen on magnified images of temporal bone CT studies in children. The cleft may be the fissula ante fenestram.
Temporal bone structures as small as 0.2 mm can now be depicted by use of CT with current software (Centricity; GE Medical Systems, Milwaukee, WI). On several CT studies of temporal bones, we noticed a previously undescribed area of decreased attenuation in the cochlear otic capsule, and we report the results of our efforts to learn more about it.
Methods
We retrospectively, with the approval of our institutional review board, examined the temporal bone CT studies of 200 temporal bones in 100 children without known sensorineural hearing loss. The ages ranged from 0.5 to 19.3 years; the average age was 8.8 years. The indications for CT examination were otomastoiditis (37 patients), trauma (31 patients), cholesteatoma (13 patients), conductive hearing loss (11 patients), mastoidectomy follow-up (three patients), facial nerve paralysis (two patients), and one case each of headache, otalgia, and external otitis.
The cochleas, examined in the axial plane only, were scored as follows: 0, no cleft seen; 1, small cleft possibly or probably exists; 2, small cleft definitely seen; 3, moderate-sized cleft seen; 4, large cleft seen.
Two physicians (J.B.C., C.B.), one a neuroradiologist, evaluated each temporal bone. Disagreements about the score were resolved, after discussion, by the neuroradiologist.
The cochleas were then grouped into those with and those without clefts. Those with scores of 0 or 1 were put into the group without clefts. Those with scores of 2, 3, or 4 were placed into the group with clefts.
Results
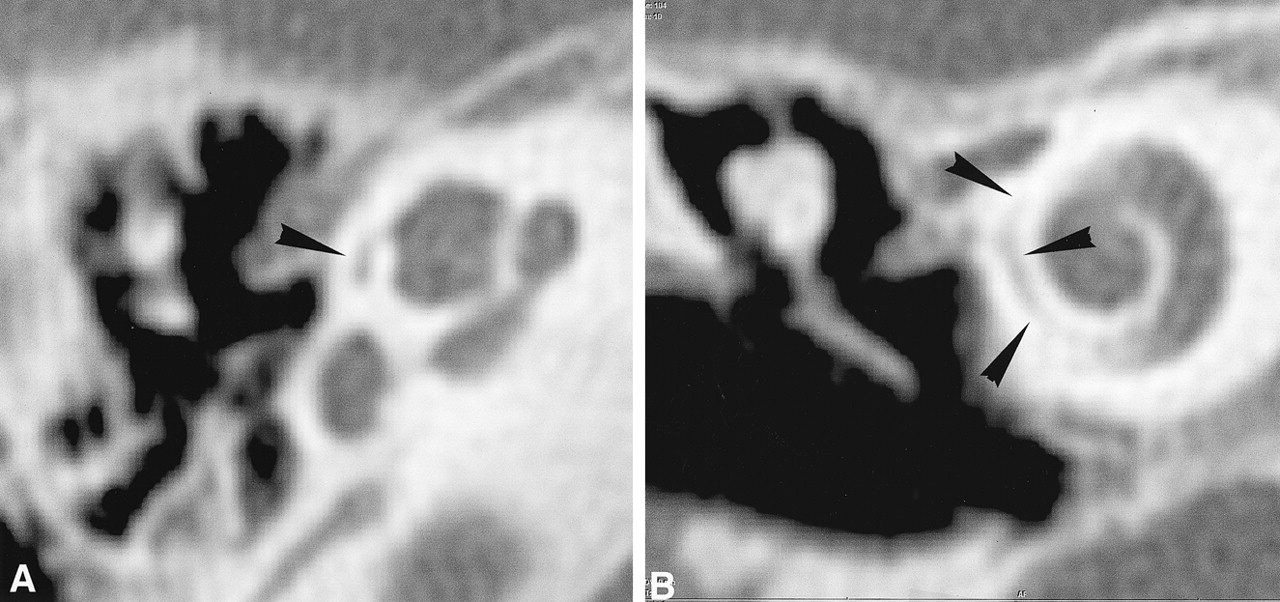
The cochlear cleft (Figs 1–3) occupies a short segment of a spiral plane in the middle of the otic capsule parallel to the base turn of the cochlea. It is a C-shaped ribbon whose upper part is underneath the cochleariform process. Its size varies, but its form is constant.

Large cochlear cleft in a 2-year-old child.
A. Axial CT. The cleft (arrowhead) measures 1.3 high and 0.3 mm wide.
B. Coronal CT. The cleft (arrowheads) is 3.4 mm high and 0.2–0.4 mm wide.

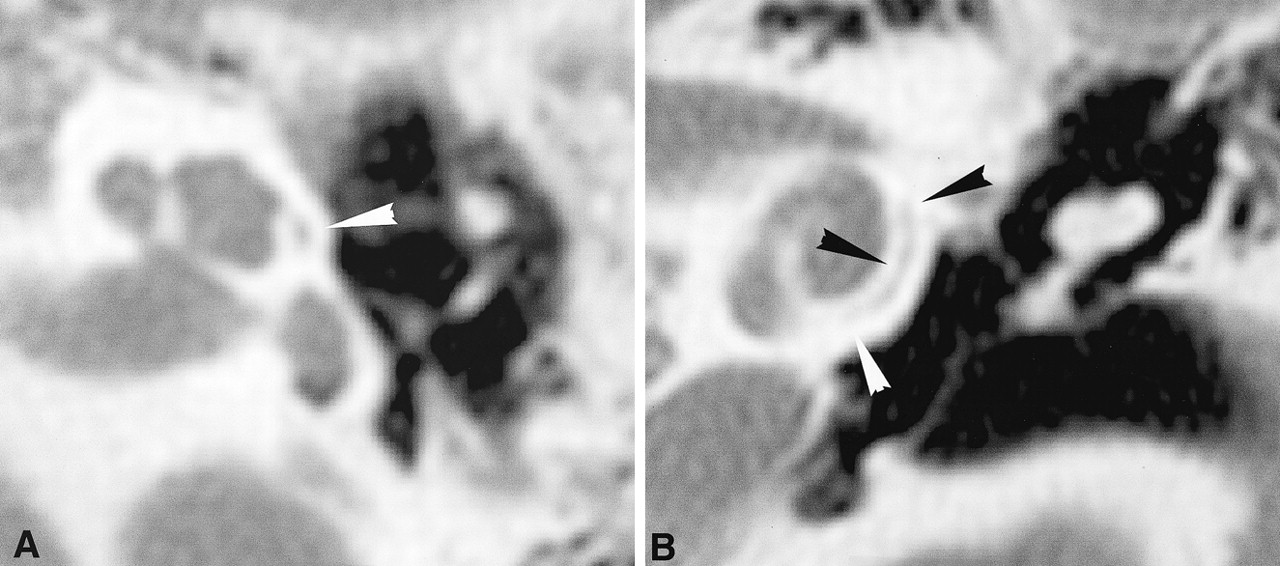
Large cochlear cleft in a 7-year-old child.
A. Axial CT. The cleft (arrowhead) is in the otic capsule lateral to the middle turn of the cochlea. It measures 0.8 high and 0.4 mm wide.
B. Coronal CT. The cleft (arrowheads) is in the lateral part of the cochlear otic capsule. It measures 5.0 mm high and 0.2–0.3 mm wide

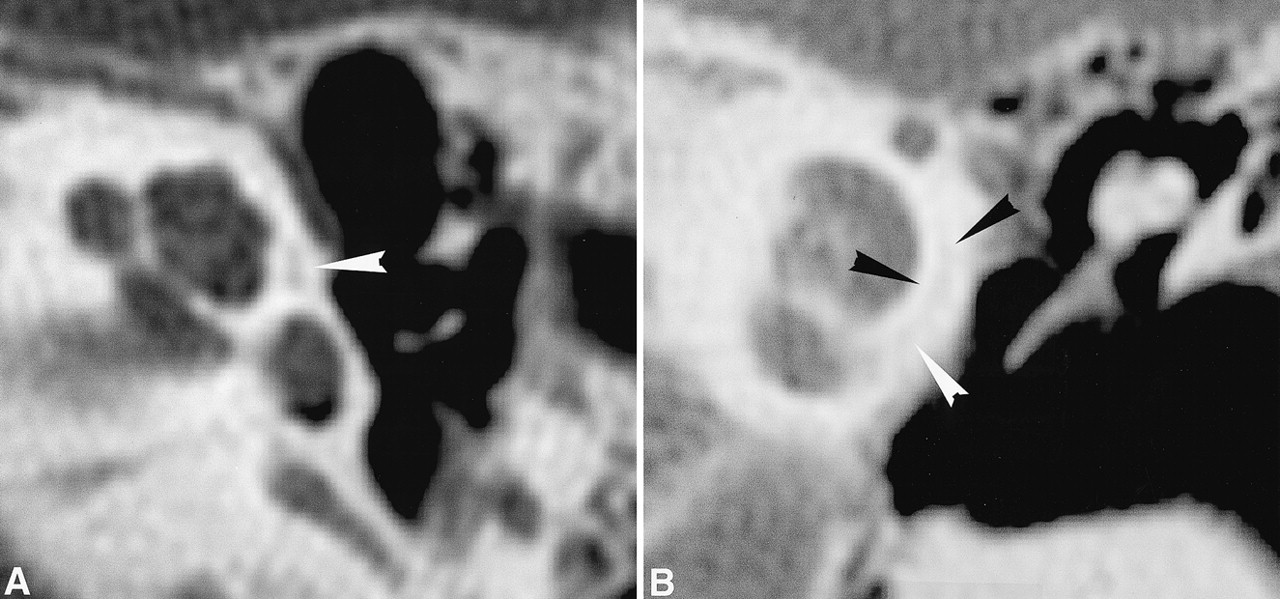
Small cochlear cleft in an 8-year-old child.
A. Axial CT. The cleft (arrowhead) measures 0.9 mm high and 0.2 mm wide.
B. Coronal CT. The cleft (arrowheads) is 3.7 mm high and 0.2–0.4 mm wide.
Cochlear clefts were present in 34% of the 200 temporal bones of the 100 patients. Forty-one percent of the patients had at least one cochlear cleft. The cochlear cleft was bilateral in 26% and unilateral in 15% of the normal population. Its frequency of occurrence was equal on both sides.
The cochlear cleft scores of the 200 temporal bones are shown in Table 1. Of them, 133 temporal bones fell into the groups without clefts, and 67 were placed in the groups with clefts (Table 1).
“Cochlear Cleft” Scores
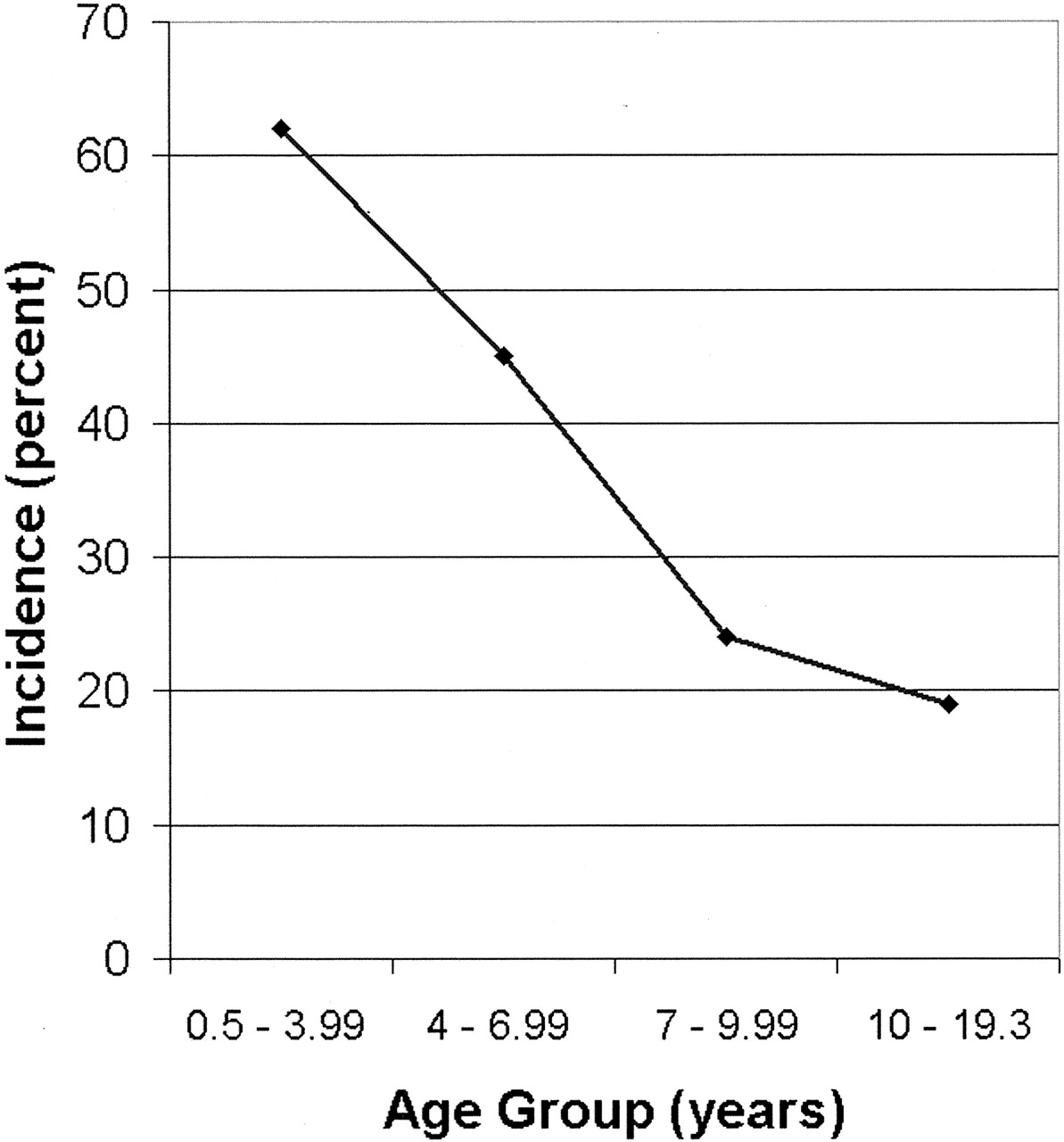
We noticed that the average cochlear cleft score decreased in older children (Table 2). We found the reason for this decrease was that the cochlear cleft was seen less often in older children (Table 3). We divided the patients into four age groups. The cochlear cleft incidence dropped from 62% in the youngest group to 19% in the oldest group (Fig 4).

Plot of cochlear cleft occurrence versus age. The occurrence rate decreases from 62% in the youngest age group to 19% in the oldest.
Average “Cochlear Cleft” Scores at Various Ages
“Cochlear Cleft” Incidence at Various Ages
Discussion
The cochlear cleft is contained within the otic capsule, a structure differing from other bones in the large number and early fusion of its ossification centers, in its growth within the fetus to adult size, and in its layered structure (1). Its 14 ossification centers form and fuse in just 6 weeks from the 15th to 21st weeks of fetal life, and the capsule attains adult size at 21 weeks. The capsule retains its fetal architecture and is not converted into haversian bone. The capsule consists of three bone layers (2). The inner layer is adjacent to the labyrinthine periosteum and is called the inner periosteal layer. The outer layer lies under the periosteum of the middle ear cleft or in contact with the petrous temporal bone (3) or dura and is called the outer periosteal layer. In between is the middle or enchondral layer (4). In the fetus, this middle layer is first composed of cartilage islands, which may persist or differentiate into either endochondral bone or fibrous tissue. In most of the capsule, endochondral bone results, but differentiation into fibrous tissue or cartilage occurs adjacent to the oval window to form the fissula ante fenestram (Fig 5).

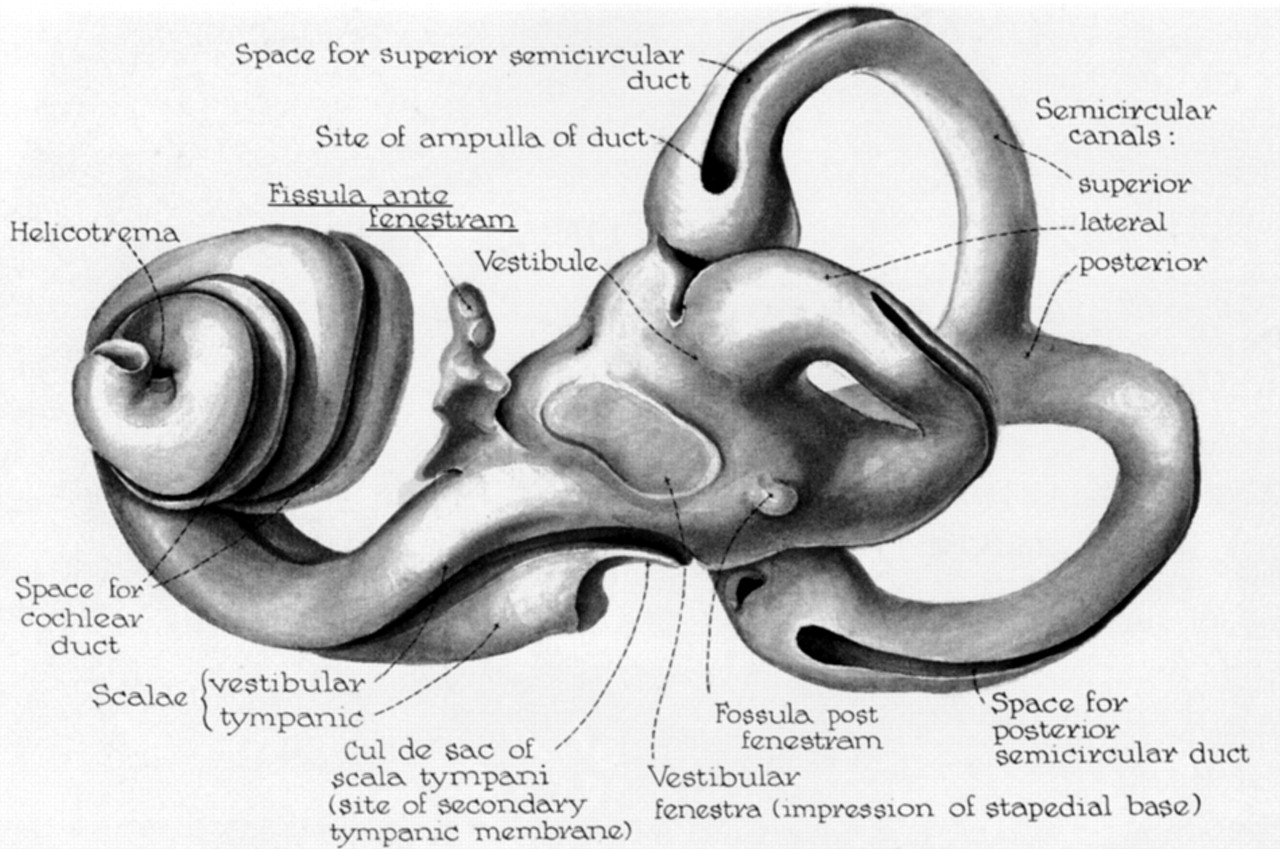
Illustration of the perilymphatic labyrinthine space, the fissula ante fenestram (label underlined) and fossula post fenestram (adapted from [8], permission pending). The endolymphatic spaces within the semicircular canals and cochlear duct are drawn as grooves in the perilymphatic surface. The outer surface of the perilymphatic space conforms to the bony labyrinth. The fissula ante fenestram arises from the lateral wall of the vestibule and nearby scala vestibulae, and it continues parallel to the adjacent cochlear turn.
Three-dimensional reconstructions from histologic sections of the fissula ante fenestram (5) in one fetus, one 2-year-old child, and one 18-year-old adult have shown the fissula ante fenestram as an irregular ribbon-like space, filled mostly with cartilage in the examples, that passes anteriorly within the otic capsule from the vestibule to the periosteum of the middle ear. In the fetus, the fissula ante fenestram then extends further in the capsule beyond the spot at which it contacts middle ear periosteum. This area of periosteal contact was near the “pulley” of the tensor tympani muscle, the cochleariform process (6).
By searching the Internet, we found a photomicrograph of a cochlear capsule space resembling a cochlear cleft at another institution (Fig 6). This cleft is in the middle layer of the otic capsule. There is no proof that the space shown in the photomicrograph and the cochlear cleft are the same.

Temporal bone photomicrographs showing temporal bone structures in an axial plane. (Courtesy of Dr. Barbara A. Bohne at the Washington University in St. Louis School of Medicine)
A, A nonosseous cleft is in the lateral part of the cochlear otic capsule (arrow). Ear structures visible are the carotid artery (CA), cochlea (CO), eustachian tube (ET), facial nerve (FN), foot plate of the stapes (FP), internal auditory canal (IAC), tympanic membrane (TM), tensor tympani muscle (TT), and vestibule (VE).
B, Enlarged view of the cochlea. The cochlear cleft (CC) is in the middle layer of the otic capsule. The base turn (BT) and middle turn (MT) of the cochlea are adjacent to the cleft.
It is probable either that the cochlear cleft is a space in the interface between the endosteal and outer periosteal layers of the otic capsule or that it is related to the fissula ante fenestram. However, we have no direct proof of this. The upper part of the cleft lies in the same region occupied by the fissula ante fenestram anterior to the oval window and medial to the cochleariform process. The lower part of the cleft in the inferolateral cochlear capsule on coronal CT images does not correspond closely to what is seen on histologic sections. This discrepancy may be due to the different axial planes of the histologic and CT images.
The decreasing incidence of the cochlear cleft with age suggests that it is being replaced or filled in with bone; however, we have no proof of this.
Other causes of areas of decreased attenuation in the otic capsule are osteogenesis imperfecta, otospongiosis, and Paget disease (7). These conditions were not present in our population.
Conclusion
A small nonosseous space we now call the cochlear cleft in the otic capsule is frequently seen on magnified CT images of the temporal bone. It is probable that this cleft is a space between the endosteal and outer periosteal layers of the otic capsule or that it is closely related to the fissula ante fenestram. The cochlear cleft is seen less often with advancing age.
Acknowledgments
Barbara A. Bohne, PhD, Professor of Otolaryngology at Washington University in St. Louis School of Medicine, took the temporal bone microphotograph. Her assistance is deeply appreciated. Judy Beane, PhD, and Stacy Poe, MS, performed the statistical analysis. Their assistance is deeply appreciated.
- Received May 23, 2003.
- Accepted after revision July 11, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comprehensive Review of Inner Ear Anatomy on Photon-Counting CT
- Internal Auditory Canal Diverticula among Pediatric Patients: Prevalence and Assessment for Hearing Loss and Anatomic Associations
- Retrospective Review of Otic Capsule Contour and Thickness in Patients with Otosclerosis and Individuals with Normal Hearing on CT
- Temporal Bone CT: Anatomy, Technique, and Associated Pathophysiology
- Incomplete Endochondral Ossification of the Otic Capsule, A Variation in Children: Evaluation of Its Prevalence and Extent in Children with and without Sensorineural Hearing Loss