
Abstract
Summary: The HydroCoil Embolic System (HES; MicroVention, Aliso Viejo, CA) was developed to improve the efficacy of endovascular treatment of cerebral aneurysms. The HES may reduce recurrences of aneurysms by allowing for increased packing density as compared with platinum coils. We report our initial experience with the HES in the treatment of 11 patients with cerebral aneurysms and compare findings to those in size-matched control cases treated with platinum coils. The HES provided substantially improved volumetric packing of the aneurysm lumen relative to standard platinum coils (73% vs. 32%; P=.0001).
A principal disadvantage of endovascular therapy of cerebral aneurysms with endovascular coils as compared with surgical clipping is aneurysm recurrence (1–3). Aneurysm recurrence following endovascular therapy is likely related, at least in part, to the density of packing of coils into the aneurysm, defined as volumetric percentage occlusion of the aneurysm cavity with the endovascular device (4–7). The HydroCoil Embolic System (HES; MicroVention, Aliso Viejo, CA) is designed with an expansile hydrogel that should theoretically fill more of the aneurysm lumen than standard platinum coils (8). We report our experience with the HES in 11 cases of cerebral aneurysms, with particular attention to the degree of aneurysm filling with embolic coils, and compare them to size-matched cases treated with platinum coils.
Technique
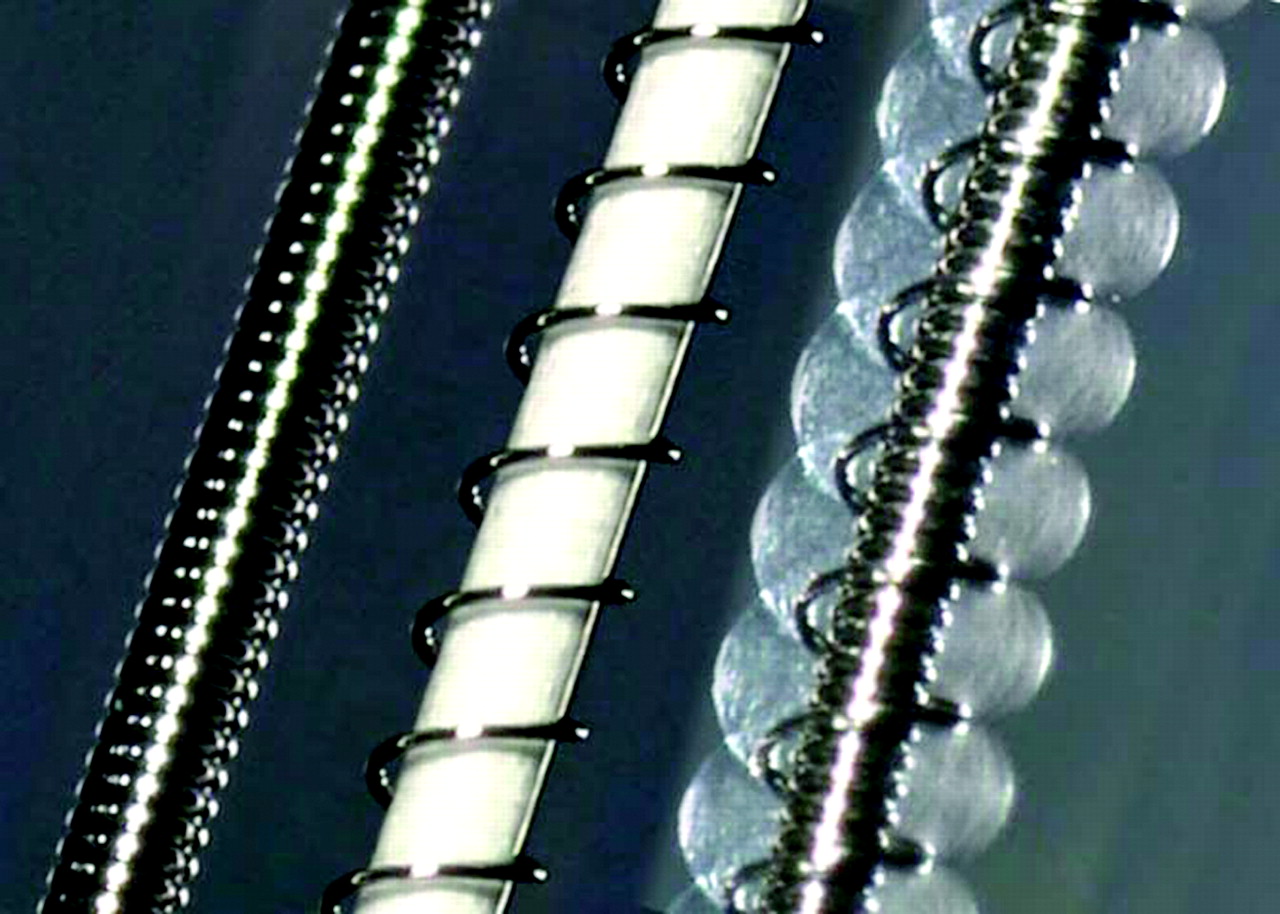
The HES is constructed as a hybrid hydrogel-platinum coil device (Fig 1). The initial diameter of these devices is 0.009 inch, and the expanded diameter is 0.027 inch. In blood, the hydrogel swells to its maximum diameter (three times the original coil diameter) in approximately 20 minutes.

Hybrid hydrogel-platinum coil device. Left, Bare platinum coil. Middle, Prehydration image, showing initial profile of the device. Highly compact hydrogel material is wrapped around a platinum coil. An outer “overcoil” is wrapped around the hydrogel-covered coil. The outer diameter of the coil is 0.008 inch. The thickness of the hydrogel is approximately 0.0005 inch, such that the outer diameter of the gel covering is 0.009 inch. With the overcoil, the outer diameter is 0.013 inch. Right, Posthydration image of the device, showing marked expansion of the hydrogel material, which has become translucent. The radial thickness of the expanded hydrogel is approximately 0.009 inch, such that the total outer diameter of the hydrated device is 0.027 inch.
We chose to apply the HES to patients with “medium”-size aneurysms, ranging from 3.5 to 8.5 mm in diameter. The aneurysms treated with HES were treated in a standardized manner. A single, standard, platinum framing coil (MicroVention, Aliso Viejo, CA; or Micrus Corporation, Mountain View, CA) was deposited in the aneurysm. HES coils (mean, 1.6 HES coils; range, 1–4 HES coils) were then deposited to fill most of the aneurysm volume. Finally, where indicated, the remainder of the aneurysm was then filled with small, soft platinum coils. Coils were added until no further coils would fit into the aneurysm without depositing in the parent vessel. Aneurysms included were located in wide variety of locations in both the anterior and posterior circulation.
A control group of 11 patients treated with standard platinum coils was assembled from our recent experience. These aneurysms were chosen to be similar in size to the aneurysms treated with HES and were located in a wide variety of locations in both the anterior and posterior circulation. These aneurysms were treated by adding coils until no further coils would fit into the aneurysm without depositing in the parent vessel.
None of cases required the use of balloon remodeling or adjunctive stent placement. Five patients in the HES group and four patients in the standard coil group had ruptured aneurysms. No clinical complications occurred in either the HES group or the standard coil group.
The aneurysm volume was calculated by assuming that the aneurysms were elliptical, by using the formula: 


The coil packing density was expressed by using the following formula: 
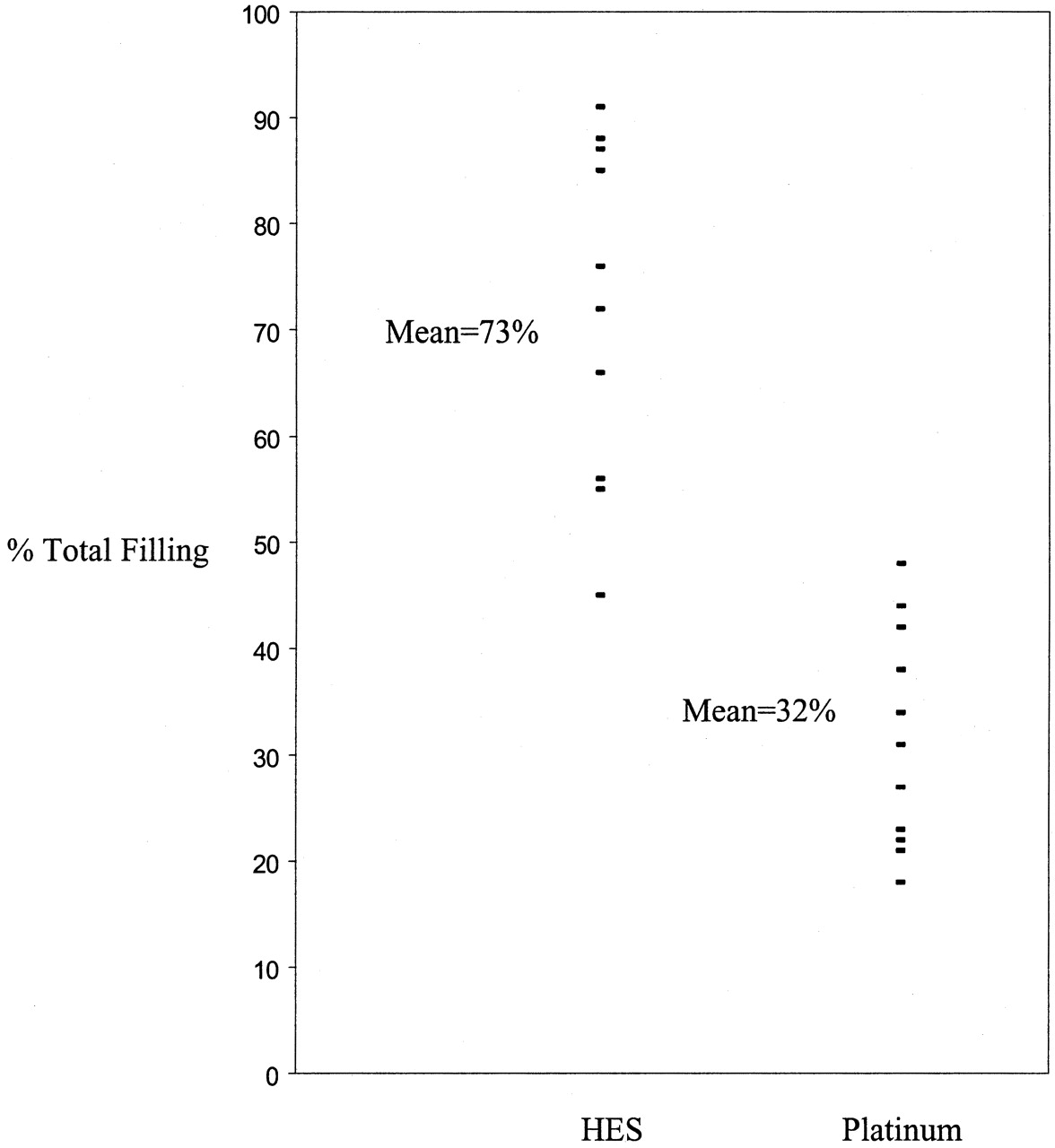
Aneurysm volumes, packing densities, numbers of coils per aneurysm, and number of coils per milliliter of aneurysm volume were compared between groups by using two-sample, two-tailed t tests (Table 1). The HES provided improved packing of the aneurysm lumen relative to standard platinum coils (72% vs. 32%; P=.0001) (Fig 2). With HES, there were trends toward decreased coils per aneurysm (3.9 coils/aneurysm vs 4.6 coils/aneurysm) and decreased coils per milliliter of aneurysm volume (55 coils/mL versus 80 coils/mL), but these trends were not statistically significant.

Scatter diagram of percent total occlusion of 11 aneurysms treated with platinum coils and 11 aneurysms treated with HES coils.
Comparison of aneurysms treated with adjunctive HydroCoil Embolization System (HES) vs. platinum coils alone
Discussion
Cerebral aneurysms treated with endovascular coil packing are only partially filled with coils, with most the intraluminal volume being filled initially with thrombus (9). Natural thrombolytic processes acting on this unstable thrombus may, in part, cause recurrence of aneurysms following endovascular coil therapy. An aneurysm filled with fewer coils and more thrombus could reasonably be expected to have a greater likelihood of recurrence. Indeed, low aneurysm coil packing density is associated with an increased risk of aneurysm recurrence, especially if less than 25% (4–7). The expanding hydrogel on the HES displaces clotting blood from the aneurysm lumen, resulting in a better packing density.
In our practice, we pack aneurysms tightly with coils, stopping coil deposition only when no more coils can be safely deposited. Because of the volume of hydrogel deposited with the HES, we suspected that we might use fewer coils overall. There were trends toward decreases in coils per aneurysm and coils per milliliter of aneurysm volume, but these trends did not reach statistical significance. This trend toward use of fewer coils would probably be amplified in larger aneurysms. In addition, HES coils are now available in longer lengths and larger diameters than were previously available, which might also contribute to a trend toward use of fewer coils. Because the hydrogel is soft and deformable, it may not block the deposition of further platinum coils in the same way that a purely platinum coil does. HES coils are more expensive than standard platinum coils, but, because we tended to use only one or two in each case, we do not feel that they added substantial cost to the procedure.
We do not advocate using the HES coil as the only coil to treat an aneurysm. We used standard coils to form a “basket” or “framework” for subsequent deposition of HES coils. We then deposited HES coils to fill most the aneurysm volume. In six of 11 cases, we used only a single HES coil. Because of the expansion of the gel, HES coils have a maximum of 5 minutes of repositioning time before detachment or removal is necessary. We did not experience any deployment difficulty related to this time limitation. The HES coil is stiffer than standard coils, and therefore it is often not generally used as the final or “finishing” coil. Rather, the final coil was often a small, soft standard platinum coil. Smaller and softer HES coils suitable for use as “finishing” coils are currently under development.
This is a limited study of initial experience at a single center. Although we are encouraged by the improvement in aneurysm packing with HES, the effectiveness of hydrogel in preventing aneurysm recurrence remains to be proved. The HydroCoil for Embolic Aneurysm Occlusion (HEAL) trial is a multicenter trial that is currently underway that is expected to yield information regarding aneurysm recurrence following treatment with HES. We look forward to the HEAL trial results for proof that improved aneurysm packing with HES will yield a decrease in aneurysm recurrence.
Conclusion
Our initial experience demonstrates that the HES allows substantially improved packing of the aneurysm lumen relative to standard platinum coils (72% vs. 32%; P=.0001). We were able to significantly improve aneurysm packing even in cases in which only a single HES was used. Future, larger series with follow-up will be necessary to demonstrate that this improvement in aneurysm filling correlates with a decreased rate of aneurysm recurrence.
Footnotes
Drs. Cloft and Kallmes receive research support from MicroVention. Dr. Kallmes is also a stockholders in MicroVention.
References
- Received June 4, 2003.
- Accepted after revision July 13, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- GEL THE NEC: a prospective registry evaluating the safety, ease of use, and efficacy of the HydroSoft coil as a finishing device
- An injectable shear-thinning biomaterial for endovascular embolization
- HydroCoils Are Associated with Lower Angiographic Recurrence Rates Than Are Bare Platinum Coils in Treatment of "Difficult-to-Treat" Aneurysms: A Post Hoc Subgroup Analysis of the HELPS Trial
- HydroCoils Reduce Recurrence Rates in Recently Ruptured Medium-Sized Intracranial Aneurysms: A Subgroup Analysis of the HELPS Trial
- Coil Type Does Not Affect Angiographic Follow-Up Outcomes of Cerebral Aneurysm Coiling: A Systematic Review and Meta-Analysis
- The next generation HydroCoil: initial clinical experience with the HydroFill embolic coil
- Review of 2 Decades of Aneurysm-Recurrence Literature, Part 1: Reducing Recurrence after Endovascular Coiling
- Mathematic Analysis of Incremental Packing Density with Detachable Coils: Does That Last Coil Matter Much?
- HydroCoils, Occlusion Rates, and Outcomes: A Large Single-Center Study
- Angiographic and Clinical Outcomes in 200 Consecutive Patients with Cerebral Aneurysm Treated with Hydrogel-Coated Coils
- Angiographic and Histologic Comparison of Experimental Aneurysms Embolized with Hydrogel Filaments
- Computerized Assessment of Angiographic Occlusion Rate and Coil Density in Embolized Human Cerebral Aneurysms
- Endovascular Coiling of Cerebral Aneurysms Using "Bioactive" or Coated-Coil Technologies: A Systematic Review of the Literature
- Embolization of Intracranial Aneurysms With Hydrogel-Coated Coils Versus Inert Platinum Coils: Effects on Packing Density, Coil Length and Quantity, Procedure Performance, Cost, Length of Hospital Stay, and Durability of Therapy
- Rates of Delayed Rebleeding From Intracranial Aneurysms Are Low After Surgical and Endovascular Treatment
- Matrix Detachable Coils for the Endovascular Treatment of Intracranial Aneurysms: Analysis of Early Angiographic and Clinical Outcomes
- Stroke Review: Advances in Interventional Neuroradiology 2004