
Abstract
BACKGROUND AND PURPOSE: Transcranial color-coded real-time sonography (TCCS) is a useful tool to evaluate disease of the middle cerebral artery (MCA). This study was undertaken to identify TCCS criteria for the diagnosis of MCA stem and MCA branch occlusions.
METHODS: TCCS and digital subtraction angiography were performed in 55 consecutive patients with acute stroke: 10 with MCA stem occlusion, the MO group; eight with MCA branch occlusion, the MB group; and 37 with nonocclusive lesions, the control group. We measured the end-diastolic velocity (EDV) of the bilateral MCA stems and calculated the end-diastolic ratio by dividing the EDV of the unaffected side by that of the affected side.
RESULTS: EDV was highest in the control group, and end-diastolic ratio was highest in the MO group. An EDV of >25 cm/s indicated a nonocclusive lesion in the MCA, with a positive predictive value of 98.4%, a negative predictive value of 81.0%, and an accuracy of 93.9%. An EDV of ≤25 cm/s with an end-diastolic ratio of <2.7 indicated an MCA branch occlusion with a positive predictive value of 85.7%, a negative predictive value of 97.2%, and an accuracy of 95.3%. An EDV of ≤25 cm/s with an end-diastolic ratio of ≥2.7 indicated MCA stem occlusion with a positive predictive value of 100%, a negative predictive value of 100%, and an accuracy of 100%.
CONCLUSION: We developed TCCS criteria for the diagnosis of MCA diseases. MCA flow velocity detected by means of TCCS can help identify MCA stem occlusion as well as MCA branch occlusion.
In the early 1990s, transcranial color-coded real-time sonography (TCCS) was introduced as a new method for imaging the basal cerebral arteries (1–3). TCCS is a noninvasive, easy-to-repeat, diagnostic technique that is widely used for the evaluation of cerebral hemodynamics. As a result of combining the B-mode facility and the color-coded Doppler facility, the brain vessels can be clearly displayed. Furthermore, since the angle of insonation can be measured and corrected for, one can obtain velocity measurements that are closer to true values (4, 5). Thus, TCCS is a useful tool in evaluating vascular diseases of the middle cerebral arteries (MCAs), particularly in patients with ischemic stroke.
However, only a few reports have described the diagnosis of MCA stem occlusion with TCCS (6, 7). In fact, TCCS criteria for MCA occlusion, particularly MCA branch occlusion, have not yet been established. MCA branch occlusion frequently occurs in patients with acute ischemic stroke. Therefore, it is important to be able to evaluate the MCA branch occlusion as well as the MCA stem occlusion when one is deciding on a patient’s therapy.
Peripheral resistance, which is found after the point of measurement, is thought to reflect blood flow velocity; the higher peripheral resistance, the lower the blood flow velocity. Therefore, we hypothesized that the blood velocity in the MCA stem of patients with MCA branch occlusion is lower than that in patients without MCA occlusion and that it is higher than that of patients with MCA stem occlusion. The aim of the current study was to establish TCCS criteria for determining the specific sites of MCA occlusion.
Methods
We prospectively performed TCCS in 66 consecutive patients with acute stroke who underwent intra-arterial digital subtraction angiography (DSA). TCCS examinations were performed 24 hours before and after the intra-arterial DSA study. Eleven patients (three with occlusion or a severe stenosis in internal carotid artery, six with MCA stem stenosis, and two with proximal MCA occlusion) were excluded from this study. Patients with proximal MCA occlusion were excluded because TCCS could not display the flow signal of the MCA, and thus the flow velocity could not be measured. Therefore, 55 patients were enrolled. Their stroke subtypes were as follows: two patients had a lacunar stroke, 10 had atherothrombotic stroke, 20 had cardioembolic stroke, one had a transient ischemic attack, 18 had other types of ischemic stroke, three had hemorrhagic stroke, and one had amourosis fugax.
The study protocol followed all principles outlined in the Declaration of Helsinki. Selective angiography was performed by using biplane DSA (Angio Rex Super-G and DFP-2000A; Toshiba, Tokyo, Japan). All examinations were performed by means of transbrachial or transfemoral catheterization in accordance with the Seldinger method. Standard anteroposterior and lateral images were routinely obtained.
According to the DSA results, we assigned the patients as follows: Patients with an MCA stem occlusion were the MO group, patients with an MCA branch occlusion were the MB group, and patients with no occlusive or stenotic MCA lesions were the control group.
TCCS was performed by using a unit (Sonos 5500; Philips Medical Systems, Japan, Tokyo) with a 1.0–3.0-MHz sector scan. The transtemporal acoustic window was used to visualize the MCA stem in real time by using color signals. We obtained color Doppler flow images and measured flow velocity at the MCAs. Patients were examined first in the left lateral decubitus position and then in the right lateral decubitus position. Particular care was taken to identify an appropriate straight-vessel segment of the MCA by means of tilting, rotating, or shifting the transducer. A 1.9-mm, range-gated, pulsed Doppler sample volume was used to measure the blood flow velocity in the MCA stem. The sample volume was moved slowly from the proximal to the distal position along the horizontal segment of the MCA and displayed as a color flow image on B-mode images. We chose the measured point where the blood flow velocity was the highest. Then we measured the mean end-diastolic velocity (EDV) over five consecutive cardiac cycles. Angle correction was applied when the correction angle did not exceed 60°. Furthermore, the side-to-side ratio of the end-diastolic flow velocity (end-diastolic ratio) was calculated by dividing the velocity of the unaffected side by that of the affected side in the MO and MB groups. We also detected the end-diastolic ratio of patients in the control group by dividing the higher MCA velocity by the lower one.
The age and blood flow velocity data for each group were expressed as the mean ± SD. Statistical comparisons of velocity differences within each group were performed by using one-way factorial analysis of variance and then Scheffé multiple comparison tests. Sensitivity-specificity curve analysis was applied to obtain cutoff values for EDV to distinguish the MO or MB group from the control group and for the end-diastolic ratio to differentiate the MO group from the MB group. A P value of < .05 was accepted as indicating a significant difference.
Results
We performed intra-arterial DSA in 55 patients (46 men and nine women; mean age, 63.8 ± 13.1 years). TCCS depicted bilateral MCA flow signals in 43 patients. However, TCCS depicted only unilateral MCA flow signal intensity in the other 12 patients. Consequently, the EDV of 98 vessels was measured. Occlusive lesions were present in 10 patients with a unilateral mid-to-distal occlusion of MCA stem, seven patients with a unilateral MCA branch occlusion, one patient with bilateral MCA branch occlusions, and 37 patients without a significant occlusion or stenosis. Thus, the groups consisted of patients with an occlusion of the MCA stem (MO group, n = 10), those with an occlusion of the MCA branch (MB group, n = 8), and patients with no occlusive lesions (control group, n = 37).
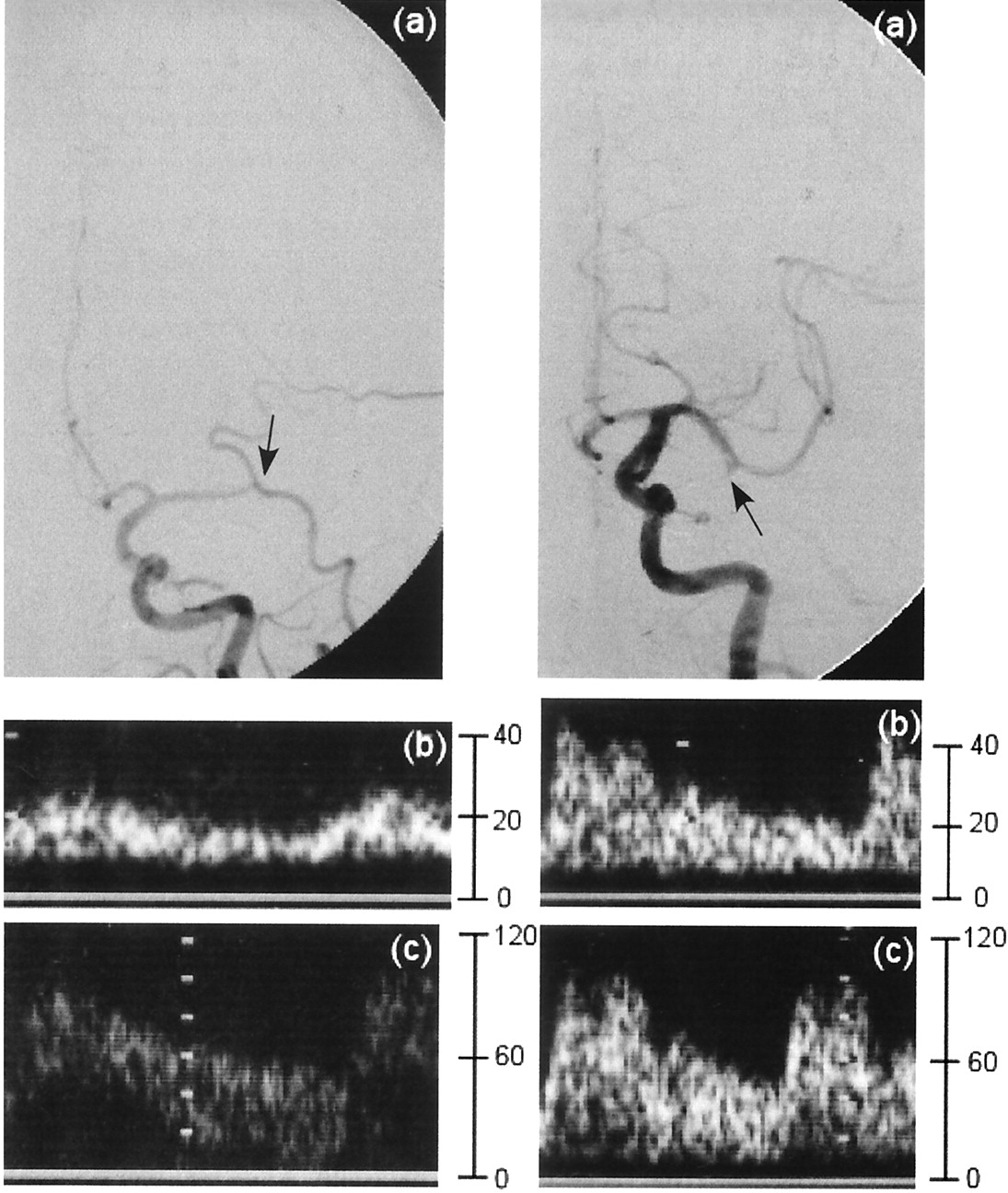
We did not detect MCA flow on the right side in the patient with bilateral MCA branch occlusions. Typical waveforms obtained in the MO and MB groups are shown in Figure 1.

Left anteroposterior carotid angiograms in representative cases evaluated with cerebral angiography and TCCS. Y axis is represented blood flow velocity (cm/s). Left image shows occlusion of the horizontal portion of the left MCA (a). Occlusion site overlies the external carotid artery branch. Doppler waveforms of the left (b) and right (c) MCAs show EDVs of 14.5 and 49.9 cm/s, respectively. Right image shows occlusion of the branch in the left MCA (a). Doppler waveforms of the left (b) and right (c) MCAs show EDVs of 18.2 and 44.6 cm/s, respectively.
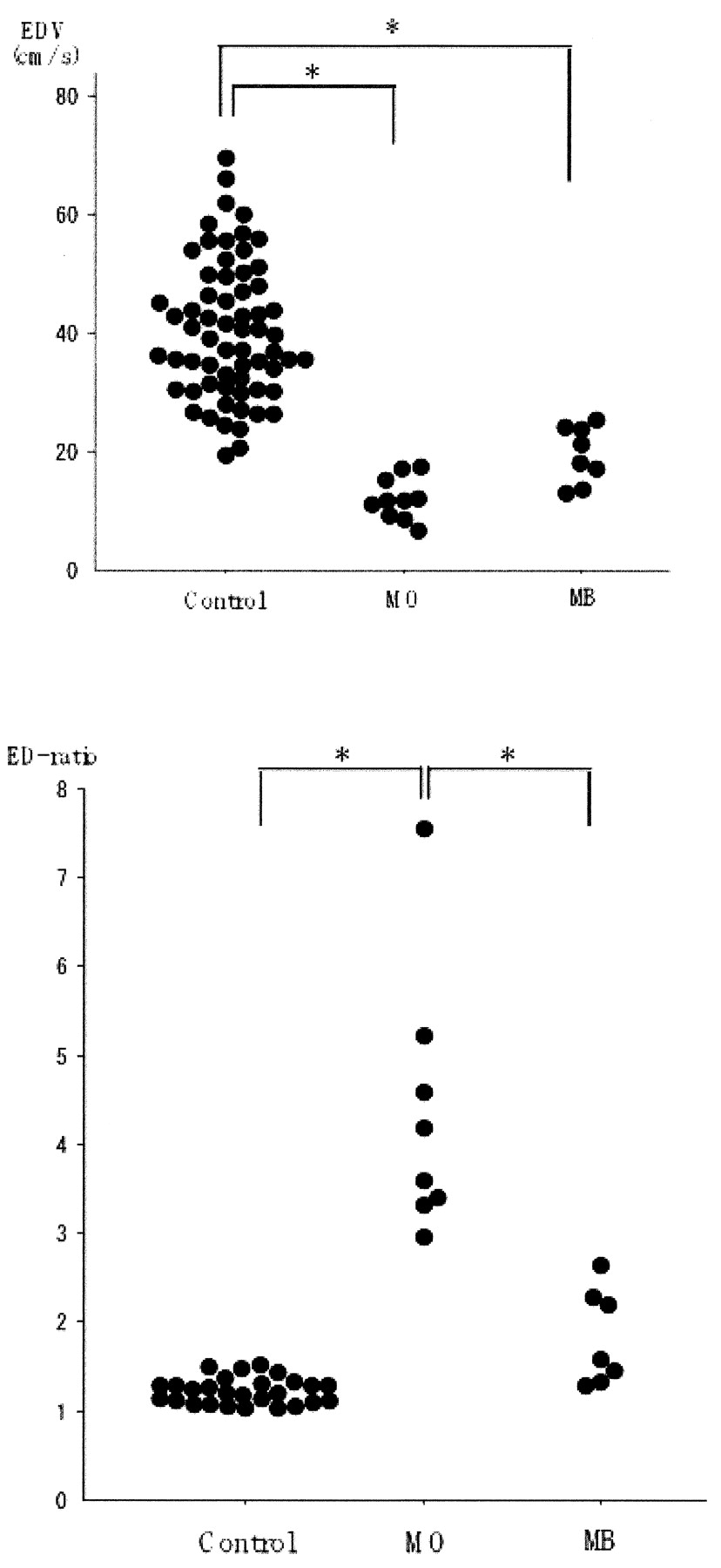
The end-diastolic ratio was calculated for all patients in whom bilateral MCAs were detected. Scattergrams of the EDV and the end-diastolic ratio for each group are shown in Figure 2. EDV was significantly higher in the control group (40.5 ± 11.5 cm/s) than in the MO group (12.2 ± 3.6 cm/s, P < .001) or MB group (19.6 ± 4.8 cm/s, P < .001). The end-diastolic ratio (4.2 ± 1.5) of the MO group was significantly greater than that of the MB group (1.8 ± 0.5, P < .001) or control group (1.2 ± 0.1, P < .001).

Scattergrams. Top, Mean EDVs (±2 SDs) for the control, MO, and MB groups are 40.5 ± 11.5, 12.2 ± 3.6, and 19.6 ± 4.8, respectively (P < .001, Scheffé test). Bottom, Mean end-diastolic ratios (±2 SDs) for the control, MO, and MB groups are 1.2 ± 0.1, 4.2 ± 1.5, and 1.8 ± 0.5, respectively (P < .001, Scheffé test).
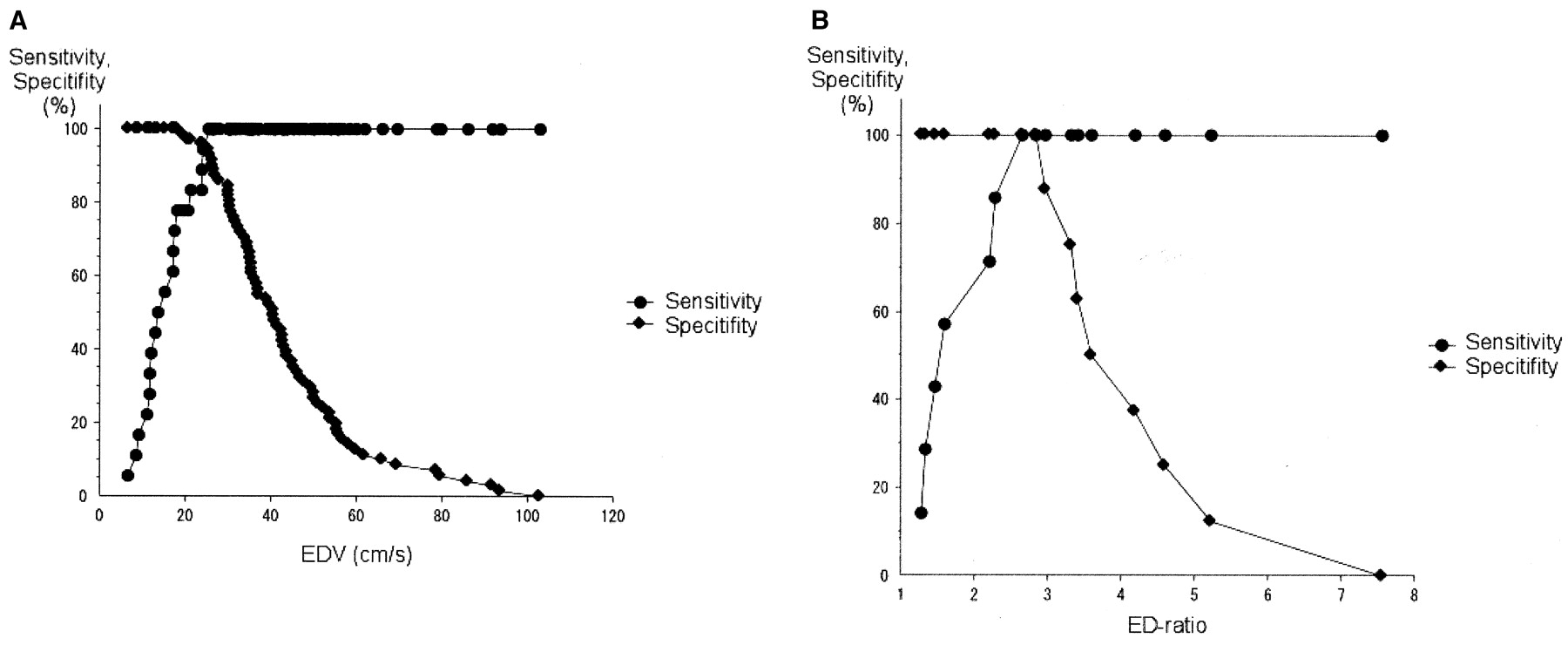
On sensitivity-specificity curve analysis, the optimal threshold value of EDV for differentiating the MO and MB groups from the control group was 25 cm/s (Fig 3A). A positive predictive value of 81.0%, a negative predictive value of 98.4%, and an accuracy of 93.9% were calculated for the optimal threshold value. The optimal threshold value of the end-diastolic ratio for discriminating the MO group from the MB group was 2.7 (Fig 3B), with a positive predictive value of 100%, a negative predictive value of 100%, and an accuracy of 100%.

Sensitivity-specificity curves.
A, Predicting MO or MB by EDV. Optimal threshold value for EDV is 25 cm/s.
B, Differentiating MO from MB by the end-diastolic ratio. Optimal threshold value for the ratio is 2.7.
Discussion
To our knowledge, this is the first study to develop TCCS criteria for diagnosing MCA stem occlusion and MCA branch occlusion. Kimura et al (7) reported that the end-diastolic ratio of patients with an MCA stem occlusion might increase to >1.9. In the present study, the end-diastolic ratio in the MO group was higher than 1.9, and this is compatible with the previous report by Kimura et al. Because they did not report TCCS criteria for determining MCA branch occlusion, the results of our MB group cannot be compared with their results.
Sensitivity-specificity curve analysis demonstrated an optimal threshold EDV value of 25 cm/s for differentiating MO and MB patients from control patients. In the MO and MB groups, 17 (94.4%) of 18 patients had an EDV <25 cm/s. However, of 37 patients in the control group, four (10.8%) had an EDV < 25 cm/s. Therefore, if the EDV is <25 cm/s, one cannot always identify the group (MO, MB, or control) to which the patient belongs. This is a limitation of our study. We have already reported that the end-diastolic ratio of control group patients was <1.9, even if EDV was under 25 cm/s (7). Therefore, the end-diastolic ratio should be useful in deciding if patients with EDV of ≤25 cm/s have an occlusive MCA lesion.
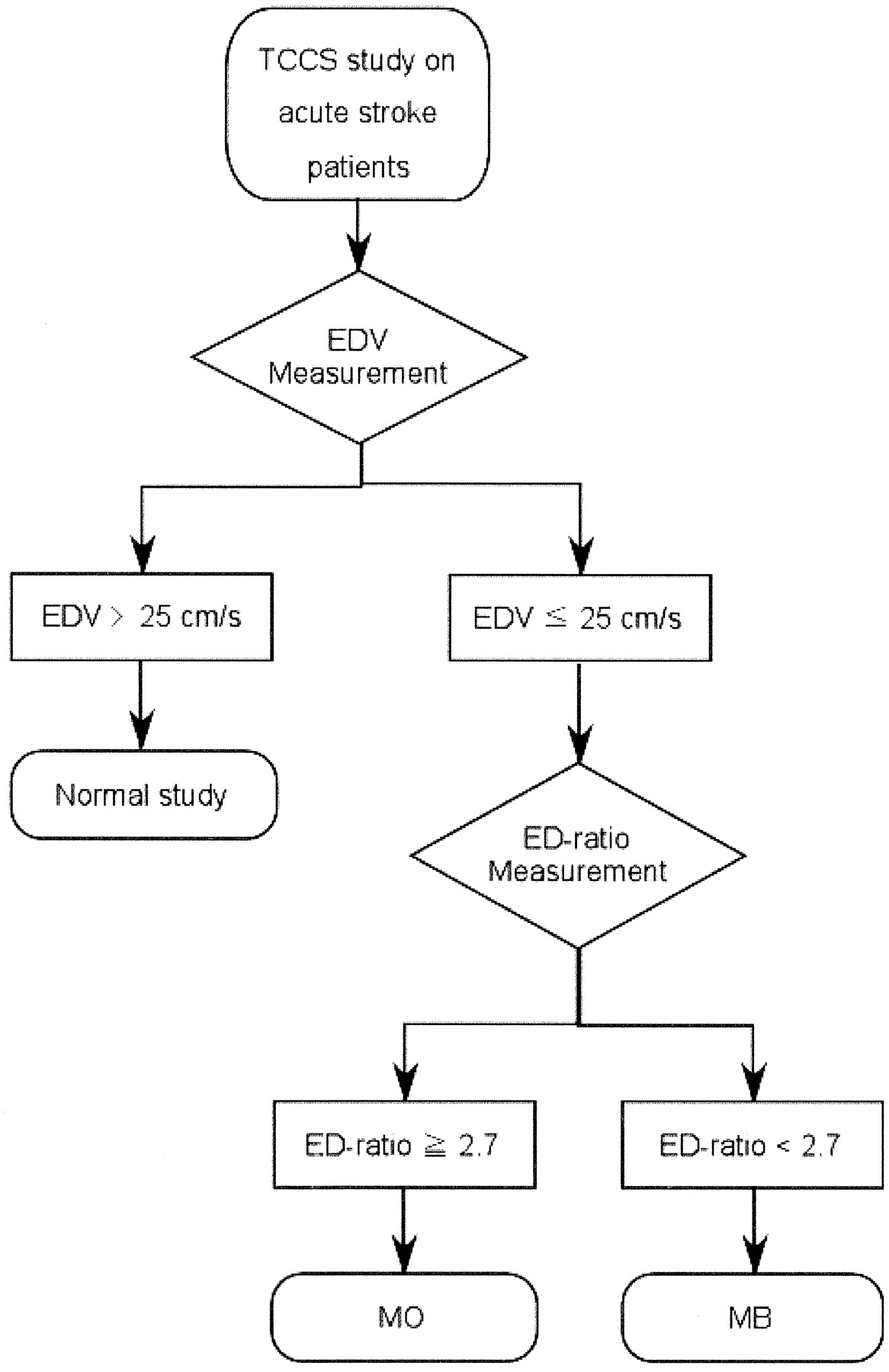
In the present study, we observed no differences in the end-diastolic ratio between the MB group and the control group. Therefore, the end-diastolic ratio alone is insufficient to diagnose an MCA branch occlusion. However, an end-diastolic ratio of 2.7 perfectly distinguished the MO group from the MB group. By using both the EDV and the end-diastolic ratio, we could distinguish the MB group from the control and MO groups. These results can be explained by the differences in the peripheral resistances among the MO, MB, and control groups. We conclude that the TCCS criteria of an EDV of ≤25 cm/s and an end-diastolic ratio of <2.7 indicates an MCA branch occlusion and that an EDV of ≤ 25 cm/s and an end-diastolic ratio of ≥2.7 indicates an MCA stem occlusion. The diagnostic algorithm for MCA stem and branch occlusion is shown in Figure 4.

Algorithm for diagnosing MO and MB by using the EDV and end-diastolic ratio on TCCS.
A few patients could not be examined because of inadequate insonation windows during TCCS. The failure rate increased with age and was higher in women because of the higher prevalence of temporal hyperosteosis (8). Furthermore, the detection rate of intracranial artery flow signal intensity by using transcranial Doppler imaging is lower in Japanese patients than in white patients (9). Contrast agents can increase the detection rate of the MCA with TCCS (8, 10–13). Therefore, use of a contrast agent may help in diagnosing MCA diseases if the MCA flow cannot be detected with conventional TCCS.
When intravenous thrombolysis with tissue plasminogen activator (t-PA) is given to ischemic stroke patients within 3 hours of stroke onset, long-term outcomes improve (14). The Prolyse in Acute Cerebral Thromboembolism (PROACT) II study (15) demonstrated a significant benefit from treatment with intra-arterial prourokinase in patients with MCA occlusion treated within 6 hours of stroke onset. Therefore, our TCCS criteria for MCA diseases may be useful in determining whether we perform the intra-arterial or venous thrombolysis in patents with hyperacute stroke. Furthermore, Eggers et al (16) reported that the use of sonography with t-PA therapy improved outcomes in patients with hyperacute ischemic stroke. Therefore, in the near future, TCCS may be useful not only as a diagnostic tool but also as a treatment in patients with MCA disease.
Conclusion
To our knowledge, we are the first group to develop TCCS criteria for diagnosing MCA stem occlusion and MCA branch occlusion. TCCS is a useful tool in the assessment of MCA diseases in patients with acute stroke.
Footnotes
Supported in part by Research Grants for Cardiovascular Diseases (14A-1) and Comprehensive Research on Aging and Health from the Ministry of Health and Welfare of Japan.
References
- Received November 11, 2003.
- Accepted after revision March 25, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}