
We read with interest the article by Takanashi et al (1) in the May 2004 issue of the AJNR. The authors reported two cases involving lesions of splenium of the corpus callosum in patients with influenza-associated encephalitis/encephalopathy. Although they described a reversible lesion in the splenium of the corpus callosum, they did not investigate causes other than encephalitis/encephalopathies. We would like to emphasize previously published reports regarding such lesions.
For instance, Kim et al (2) initially described transient splenial lesions, as revealed on MR imaging, in 1999. Focal nonhemorrhagic lesions of the corpus callosum are rare, but they have been described in various clinical conditions, and little is known about the underlying mechanisms. Although the pathogenesis is not understood, awareness of the fact that this is a reversible focal lesion may help prevent unnecessary invasive diagnostic and therapeutic intervention. Various pathologic conditions, such as multiple sclerosis, trauma, neoplasm, infarct, leukodystrophies (especially adrenoleukodystrophy), AIDS dementia complex, and Marchiafava-Bignami disease, may also involve the corpus callosum (3).
Kim et al (2) reported such lesions in six patients with focal epilepsy. They classified the lesion as demyelination and hypothesized that anticonvulsive drug toxicity was the cause. Similar lesions have been described in epileptic patients in the postictal period as well. These lesions have been interpreted as transient focal edema due to transient physiologic alteration in the callosal fibers caused by seizure activity. Association of such splenial lesion with acute cerebellitis due to herpes simplex, and its regression within 72 hours, has also been reported (4).
In support of these observations, we herein briefly report our experience with a 24-year-old man who presented with headache and apathy lasting for 5 days. He had no remarkable medical history, he was not receiving any medication, and he denied alcohol abuse. Scalp electroencephalograms were normal, and CSF testing showed slight elevation of protein levels. Results of blood tests were unremarkable for demyelinating or other systemic conditions, metachromatic leukodystrophy, antiphospholipid antibody syndrome, or HIV infection. Titers of serum immunoglobulins against human herpes viruses, herpes simplex virus, Epstein-Barr virus, varicella zoster virus, rubella virus, measles virus, papovavirus, enterovirus, influenza virus, and rotavirus, and Mycoplasma pneumonia were normal. Cranial MR images showed a focal nonenhancing lesion in the splenium of the corpus callosum, which totally regressed within 4 weeks without medication (Figs 1–2). We believe that this case represented an instance encephalitis/encephalopathy, but this could not be proved.
The case that Takanashi et al (1) reported was believed to have same underlying cause as ours, but to our knowledge the association of such a lesion with apathy or headache has not been reported. Polster et al (5) have suggested that such a transient splenial lesion appears to be a nonspecific endpoint of a different disease processes leading to vasogenic edema. This seems the most probable pathophysiologic explanation of such splenial lesions, as in our case.

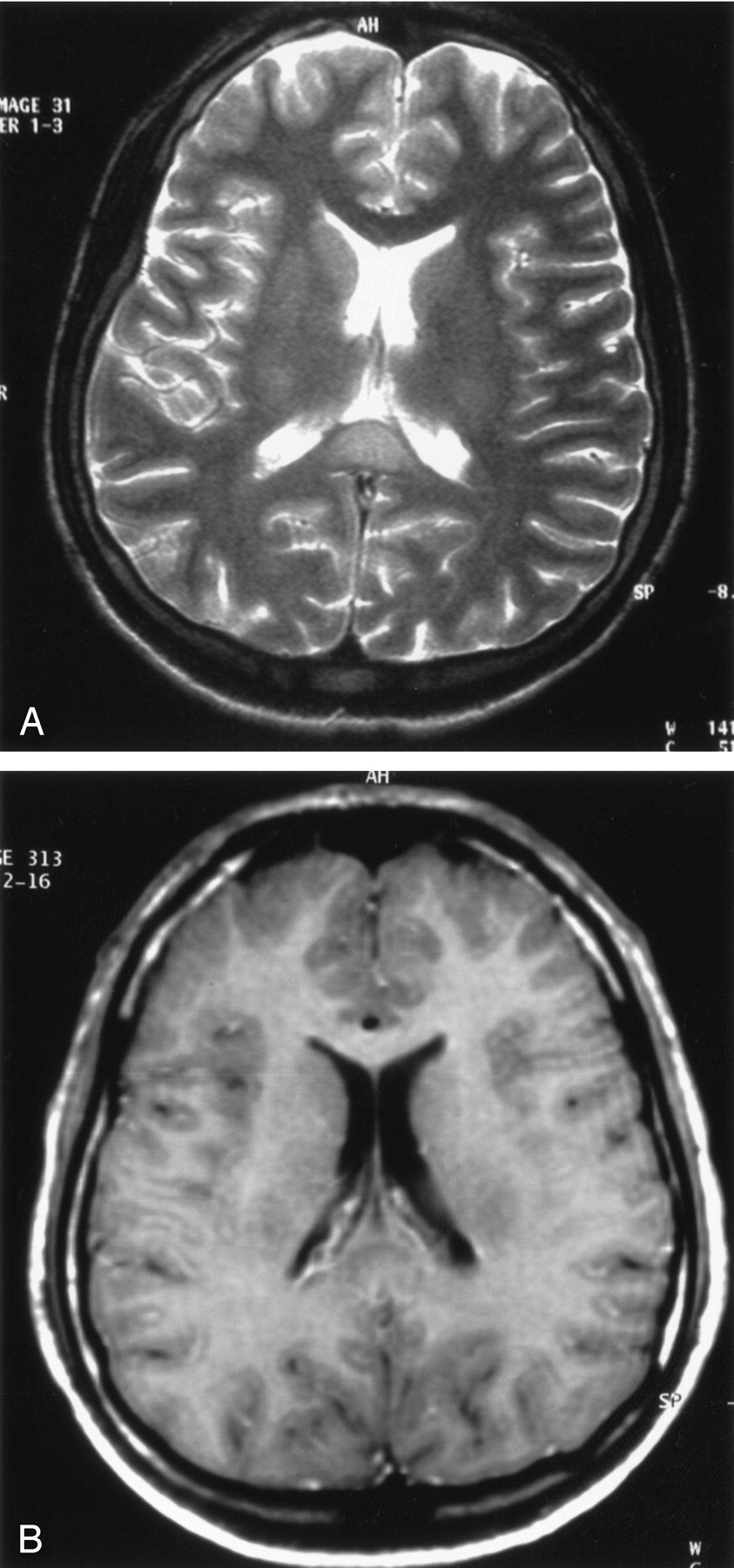
Cranial MR images obtained in a 24-year-old man show a focal nonenhancing lesion.
A, Axial T2-weighted turbo spin echo image (TR 5000 ms, TE 99 ms; NEX 2) shows hyperintense lesion in the splenium of the corpus callosum.
B, Axial T1-weighted, contrast administered spin echo image (TR 600 ms, Te 14 ms; NEX 2) reveals hypointense character of the lesion, without contrast enhancement.

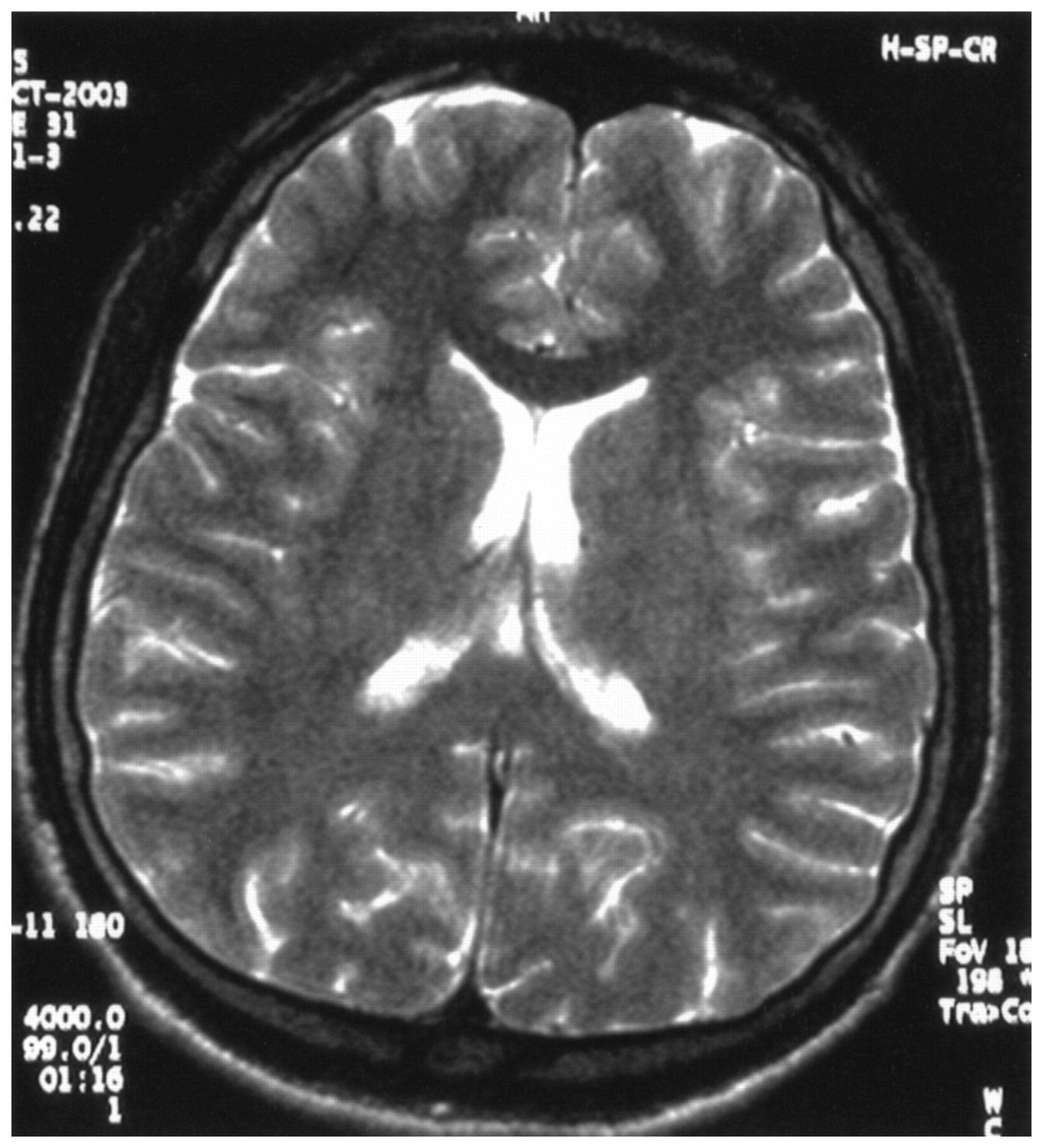
Axial T2-weighted turbo spin echo image (TR 5000 ms, TE 99 ms; NEX 2) shows resolution of the lesion in the splenium of the corpus callosum.
References
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}