
Abstract
Summary: Central pontine myelinolysis (CPM) occurs in the setting of rapidly corrected hyponatremia, especially in chronically debilitated patients. Conventional CT and MR imaging findings lag the clinical manifestations of CPM. We present a case in which restricted diffusion was identified within the central pons by using MR diffusion-weighted imaging within 24 hours of onset of patient tetraplegia and before findings were conspicuous with conventional MR imaging sequences (T1, T2, and fluid-attenuated inversion recovery).
Central pontine myelinolysis (CPM) is an osmolar disturbance resulting in demyelination that is initially difficult to detect with convention CT and MR imaging. The literature includes several cases in which the temporal evolution of CPM is followed with serial imaging (1–3). There have been a few reports describing findings of diffusion-weighted imaging (DWI) in CPM and extrapontine myelinolysis (EPM) (4, 5); however, we are unaware of published cases in which DWI demonstrated changes of CPM before development of conventional MR imaging signal intensity changes. This case also helps elucidate the temporal relationship of DWI with clinical symptoms and serum sodium levels, which are well documented for this patient.
Case Report
A 57-year-old female patient with a history of bipolar disorder, psychogenic water intoxication, and alcohol abuse was admitted to an outside hospital with weakness, confusion, and fever. On admission, the patient was found to be severely hyponatremic, with sodium levels of 95 mEq/L (normal, 135–145 mEq/L). The patient was undergoing therapy for pneumonia and urinary tract infection but remained febrile despite antibiotic therapy. The sodium level began to normalize at 111 mEq/L on day 2, 125 mEq/L on day 3, 129 mEq/L on day 5, 135 mEq/L on day 6, 140 mEq/L on day 7, 144 mEq/L on day 8, and 150 mEq/L on day 10.
Mental status transiently improved on the 2nd and 3rd hospital days, but then worsened. A noncontrast CT scan of the head was nondiagnostic on days 4 and 8. Electroencephalography and lumbar puncture findings were normal. The patient was then transferred to a tertiary care center on day 11, with a sodium level of 155 mEq/L; she was lethargic, delirious, and was developing tetraplegia (Fig 1).

Clinical-imaging correlation plotting the patient’s serum sodium concentration, imaging studies, and quantitative ADC measurements. “Hospital days” are counted from the day the patient presented at the outside hospital with hyponatremic encephalopathy. The patient was transferred to a tertiary care center on day 11. MR image was obtained on day 12 (day following hospital transfer) and showed restricted diffusion within the central pons and no signal abnormality on the remaining conventional MR images.
MR imaging after transfer (day 12) demonstrated restricted diffusion within the pons without a corresponding signal intensity abnormality on the T2-weighted or fluid-attenuated inversion recovery (FLAIR) images (Fig 2). Quantitative apparent diffusion coefficient (ADC) measurements were obtained with regions of interest centered over the central pons and hemispheric cerebellar white matter (see Figs 1, 2D, and 3D). The diagnosis of developing CPM was made. Repeat MR imaging (day 17) demonstrated interval development of a trident-shaped area of increased signal intensity in the central portion of the pons on T2-weighted and FLAIR images with an interim increase of associated restricted diffusion signal intensity abnormality (Fig 3). There was no evidence for extrapontine myelinolysis.

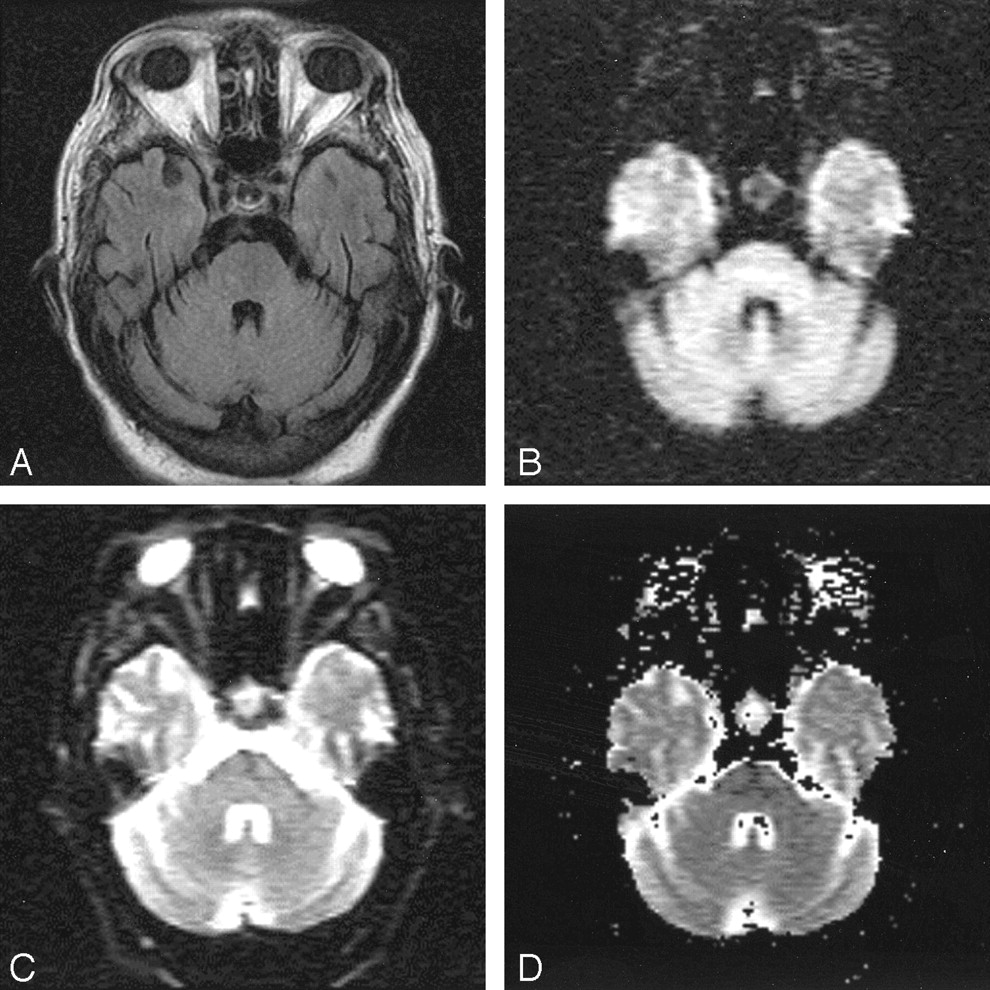
MR image of the patient’s head obtained on hospital day 12, 1 day after maximum hypernatremia, and within 24 hours of onset of tetraplegia.
A, FLAIR image (TR, 11,002; TE, 140; NEX, 1) is normal, as were proton density–and T2-weighted spin-echo images (not shown).
B, An abnormally hyperintense finding is present within the central pons on the isotropic DWI obtained with a b value of 1000.
C, There little change noted on the echo planar image obtained at b = 0.
D, The ADC map shows that hyperintensity at DWI does indeed represent restricted diffusion. (See Figure 1 for quantitative ADC results.)

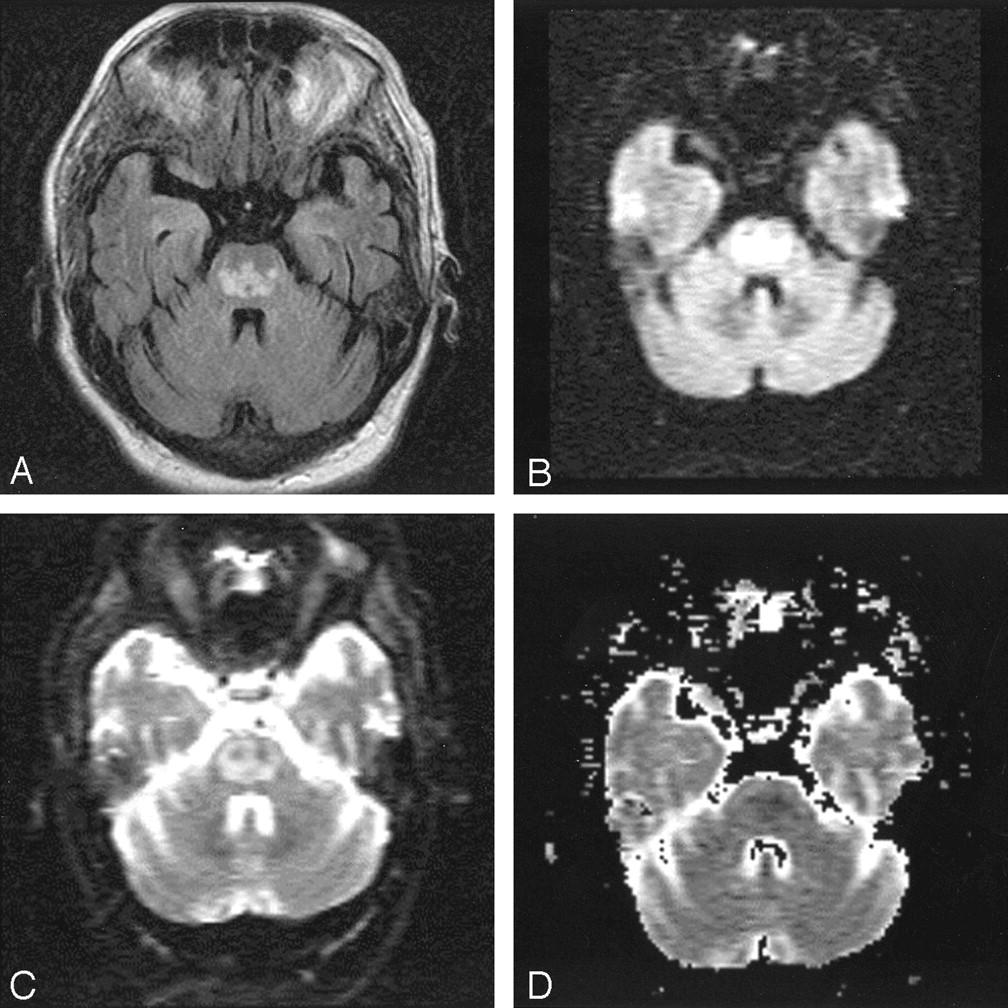
MR images of the patient’s head, obtained on hospital day 17, 3 days after renormalization of overcorrected hypernatremia.
A, FLAIR image now demonstrates the classic trident-shaped pontine signal intensity abnormality.
B, The extent of DWI signal intensity abnormality in the pons has also become more extensive, assuming a trident-shape.
C, The b = 0 image has also become abnormal in the interim.
D, The ADC map again shows that the high DWI signal intensity corresponds to restricted diffusion (see Figure 1).
Discussion
“Central pontine myelinolysis” was first termed in 1959 by Adams to describe a symmetric, demyelinating focus prominent in the central pons (6). The original patient population included only chronic alcoholics. This condition, however, has also been found in the malnourished, transplant recipients, or chronically debilitated patients (6, 7), in particular, those in whom electrolyte abnormalities include hyponatremia that is rapidly over-corrected. Symptoms of CPM include tetraplegia, pseudobulbar palsy, and acute changes in mental status leading to coma or death without intervention. Similar histologic symmetric lesions were later identified in extrapontine locations, including the white matter of the cerebellum, thalamus, globus pallidus, putamen, and lateral geniculate body, a condition termed “extrapontine myelinolysis” (EPM) (7, 8).
The pathophysiology of CPM has not been well understood. Although the original description of CPM by Adams (6) made no mention of electrolyte disturbance, it has become clear that the pathophysiology of CPM relates to the physiologic balance of osmoles in the brain (9). Histologic studies have shown oligodendroglial cells are most susceptible to CPM-related osmotic stresses, with the distribution of CPM changes paralleling the distribution of oligodendroglial cells that normally embed large neurons within the central pons, thalamus, cortex, putamen, lateral geniculate, and other extrapontine sites (7, 9–11). The transverse pontocerebellar fibers are most frequently involved, followed by long rostrocaudal tracts. Histologically, there is preservation of neurons and axons, differentiating this process from a central pontine infarct (12). There is usually no inflammatory reaction associated with osmotic demyelination, differentiating the process from multiple sclerosis, which is characterized by marked perivascular inflammation.
The mechanism of myelinolysis remains to be completely elucidated, but appears distinct from a demyelinating process such as multiple sclerosis; demyelination in CPM is characterized by intramyelinitic splitting, vacuolization, and rupture of myelin sheaths presumably because of osmotic effects. Macrophages with cytoplasm filled by myelin debris appear after several days (12).
The clinical course of CPM has been classically described as biphasic (13), beginning with a generalized encephalopathy caused by the hyponatremia, which usually transiently improves following initial elevation of sodium. This is followed by a second neurologic syndrome, which occurs 2–3 days following correction or over-correction of hyponatremia caused by myelinolysis. This latter phase is classically characterized by spastic quadriparesis and pseudobulbar palsy.
Conventional imaging findings (MR and CT) typically lag clinical manifestations, limiting the utility of imaging in early diagnosis of CPM. Because myelinolytic lesions are not demonstrated within the first 2 weeks by using conventional MR imaging pulse sequences, later imaging has been advocated to confirm the diagnosis (13). Furthermore, the diagnosis of CPM is not ruled out in the setting of normal imaging. CT is even less sensitive than MR imaging for detection of early changes of CPM (14, 15). MR imaging findings of CPM include symmetric signal intensity abnormality in the central pons at T2-weighted and FLAIR imaging. This may progress to classic hyperintense “trident-shaped” central pontine abnormality, with sparing of the ventrolateral pons and corticospinal tracts (1, 2, 15). There is associated decreased T1 signal intensity without enhancement or mass effect. The distribution of the imaging findings mirrors the demyelination pathophysiology.
DWI is a relatively new MR technique sensitive to the motion of water (16). Because the underlying process of CPM is the osmotic disturbance of water and electrolyte imbalance, it follows that DWI may be a better method to identify early pathophysiologic change. Current literature demonstrates DWI to be sensitive at very early time points after ischemic injury (17).
Our case demonstrated restricted diffusion as the first imaging manifestation of CPM, occurring within 24 hours of clinical onset of tetraplegia and before detection of abnormalities on conventional MR images, including T1-weighted spin-echo, T2-weighted spin-echo, and FLAIR images. Follow-up MR imaging performed 5 days later showed that the restricted diffusion signal intensity abnormality within the pons increased in both the size of the area involved and the magnitude of diffusion restriction. Further studies are needed to determine the progression of DWI signal intensity change, because the diffusion changes presumably do not remain restricted indefinitely.
Restricted diffusion has been reported by Cramer et al in two patients with CPM who underwent MR imaging at days 6 and 7, respectively, following onset of tetraplegia (5). Follow-up MR imaging performed at day 21 following onset of tetraplegia in the first of Cramer et al’s patients demonstrated high DWI signal intensity owing to the T2 “shine-through” effect, which suggests that the restricted diffusion does not persist beyond 3 weeks following onset of tetraplegia.
The mechanism for diffusion restriction in CPM remains to be elucidated. One can hypothesize that in the hypernatremic state water would be shifted from the extracellular interstitial compartment into either or both the intravascular compartment and within the glial cells. The decrease of free water in the interstitial space, combined with trapping of water within cells, would contribute to restricted diffusion. Furthermore, the osmotically related increase of water in the intracellular compartment would lead to cell swelling, which could contribute additionally to restriction of water movement in the interstitial space from mechanical considerations. It would be useful to repeat prior experimental studies such as those previously performed in animal models (18), but with the inclusion of MR DWI. Histologic correlation with DWI changes would likely lead to vastly improved understanding of CPM and may elucidate the choice of the most appropriate therapy for correction of hyponatremia without complication of myelinolysis.
Conclusion
This case report demonstrates the ability of DWI to depict imaging changes of CPM before these signs manifest at conventional MR imaging. DWI demonstrated restricted diffusion within the central pons in our patient within 24 hours of onset of tetraplegia. This case report supports use of DWI as a key imaging sequence in the early diagnosis of patients with suspected acute CPM, ideally allowing more prompt initiation of therapy before irreversible brain injury has occurred.
Footnotes
A portion of this work was presented as an educational exhibit at 88th Scientific Assembly of the Radiological Society of North America, December 1–6, 2002; Chicago, IL.
References
- Received March 3, 2003.
- Accepted after revision May 13, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Potentially Reversible and Recognizable Acute Encephalopathic Syndromes: Disease Categorization and MRI Appearances
- Treatment response in osmotic demyelination syndrome presenting as severe parkinsonism, ptosis and gaze palsy
- Response to IV immunoglobulin in a case of osmotic demyelination syndrome
- What to see when you are looking at confusion: a review of the neuroimaging of acute encephalopathy
- "Dazed and diffused": making sense of diffusion abnormalities in neurologic pathologies
- An unusual case of quadriparesis
- Isolated extra pontine myelinolysis presenting as acute onset parkinsonism
- Imaging evaluation of demyelinating processes of the central nervous system
- A trident in the brain, central pontine myelinolysis
- Central pontine myelinolysis in a case of cerebral malaria