
Abstract
Summary: We describe MR findings in three patients who experienced transient cortical blindness following cerebral angiograms. All angiograms were performed by using the same nonionic contrast medium. On the basis of similar clinical and radiologic findings, we believe that this entity is closely related to and probably has the same pathophysiology as posterior reversible leukoencephalopathy.
Cortical blindness is a rare but well-recognized complication of cardiovascular and cerebral angiographic procedures. It has an incidence of 0.3–1% following cerebral angiography (1); a slightly higher incidence is reported with vertebral angiography (2). CT findings of cortical blindness following angiographic procedures have been frequently reported (3); however, MR findings of cortical blindness following cerebral angiography have rarely been described (4). We report MR imaging findings in three cases of cortical blindness following cerebral angiography in which nonionic contrast media were used and in which a relative similarity of clinical and radiologic findings with that of posterior reversible leukoencephalopathy suggests a common pathophysiology.
Case Reports
Case 1
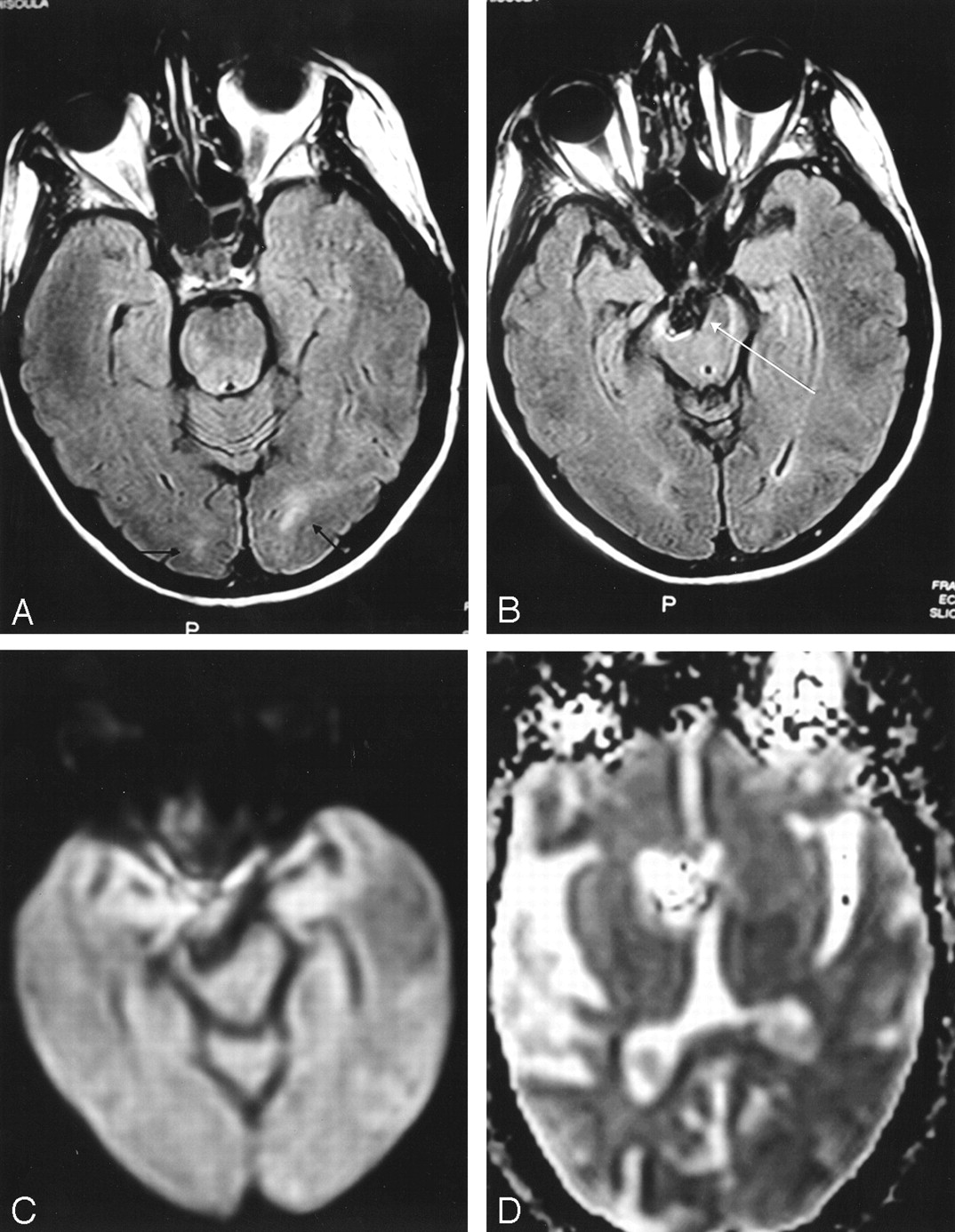
A diagnosis of a basilar artery aneurysm was established in a 45-year-old woman with a medical history of hypertension on the basis of routine CT findings. The patient underwent CT because of headaches. No subarachnoid hemorrhage was noted. A cerebral angiogram confirmed a 9 × 9-mm right superior cerebellar artery aneurysm, which was embolized with Guglielmi detachable coils. No intraprocedural or immediate postprocedural complications were noted. On the morning following the procedure (12 hours postprocedure), the patient was disoriented to time and place. There was no light perception in both eyes; pupils were reactive bilaterally. No motor deficits were noted. The patient appeared to develop Anton syndrome, with findings of confusion, cortical blindness, and denial of symptoms. Cranial CT findings appeared normal. MR imaging showed subtle scattered areas of increased T2 and fluid-attenuated inversion recovery (FLAIR) signal intensity abnormality in the occipital cortices bilaterally (Fig 1A and B). Corresponding isointense T1 signal was noted in this region. No restricted fluid motion was noted on diffusion-weighted images (Fig 1C and D). The patient began to receive steroids (decadron) and undergo hydration therapy. The next day (36 hours post procedure) the patient remained confused, but light perception had improved. The pupils were equal and reactive with right hemianopsia. No motor deficits were noted. The stroke team was consulted to evaluate the patient. An emboli-detection study with Doppler sonography was performed, and findings were negative. Steroid and hydration therapy were continued, and albumin therapy was added. The following day (60 hours post procedure) the patient’s symptoms showed marked improvement, with mild persistent right hemianopsia that was improving every day according to the patient. Near-complete visual improvement was noted at the end of 9 days, and the patient was discharged while placed on Norvasc, a tapering dose of Decadron, and Zantac. At discharge, ophthalmologic examination showed the pupils to be round and equally reactive to light, with a mild persistent right visual field defect. One week later, follow-up examination showed the patient had fully recovered from her field defect.

FLAIR MR images show hyperintensities (arrows) in occipital cortices bilaterally (A, B). Coil treatment of the right superior cerebellar artery aneurysm (long arrow) can be seen. No restricted diffusion noted on the diffusion images (C, D).
Parameters: TR, 6000; TE, 128; FOV, 24; TI, 2000; FA, 90°; matrix, 192 × 256; bandwidth, 12.5.
Case 2
A 74-year-old woman with a history of coronary artery disease and hypertension presented with acute-onset headache and dizziness. Two years earlier, she had a coronary artery bypass procedure and since then had done well. MR imaging done at that time showed 70% left internal carotid artery stenosis and a 7–8-mm basilar tip aneurysm. A cerebral angiogram performed during this admission showed 50% stenosis of the proximal left internal carotid artery, 10–15% stenosis of the right internal carotid artery, and a 7-mm basilar artery tip aneurysm. No intraprocedural complications occurred. One hour after the procedure, the patient complained of complete bilateral blindness and confusion. No light perception or color vision was noted in either eye. Pupillary light reflexes and extraocular movements were intact. A noncontrast CT scan revealed a gyriform hyperattenuation in the left parieto-occipital region, which was thought to represent extravasated contrast due to disruption of the blood-brain barrier owing to angiography (Fig 2A and B). The ventricular system appeared normal, and no mass effect or midline shift was noted. Aspirin and Decadron were prescribed. MR imaging performed the next day showed subtle, increased T2 and FLAIR signal intensity abnormality in the left occipital cortex in a relatively inferior location when compared with the CT abnormality (Fig 2C and D). The large area of abnormality seen on the CT scan was not appreciated on the MR imaging study. No restricted diffusion was noted to suggest acute ischemia as a cause for her symptoms. Over the next 24 hours, the patient’s vision gradually improved, with complete recovery of color vision and light perception to baseline and no residual visual field defects.

Axial noncontrast CT scan reveals a relatively large gyriform hyperattenuation (short arrows) in the left parietooccipital cortex (A, B). No mass effect is seen. FLAIR MR images show subtle hyperintensity (C, D) in the left occipital cortex (long arrow).
Parameters: TR, 3056; TE, 112; FOV, 24; FA, 90°; matrix, 192 × 256; bandwidth, 15.6.
Case 3
A 73-year-old woman with a history of hypertension and breast cancer presented to the emergency room secondary to a syncope episode that began 4–5 days before admission. The patient denied any symptoms of neck or chest pain, palpitations, or confusion before and after the episode of syncope. A CT scan of the brain revealed a large left-sided suprasellar mass that showed some calcification. MR imaging showed this mass to be a large, 2.7-cm left supraclinoid aneurysm; a subsequent cerebral angiogram confirmed it to be a large superior hypophyseal artery aneurysm. Twenty minutes after angiography, the patient complained of blurred vision in both eyes, with visual deficit being greater on the left side. This progressed to complete loss of vision over the next 30 minutes. Pupils were equal and reactive to light. No motor deficits were noted. Initial CT findings were negative. MR imaging performed 6 hours later showed increased T2 (Fig 3A and B) and FLAIR (Fig 3C and D) signal intensity abnormality in the occipital cortices bilaterally that was greater on the right side. Diffusion-weighted imaging did not reveal any abnormality to suggest acute ischemia (Fig 3E and F). Steroid treatment was begun immediately. Twenty-four hours following the procedure, the patient was able to see out of the right eye without any difficulty, although some blurring of vision persisted in the left eye. Repeat cerebral angiography was performed the next day (2 days post procedure) to investigate any possible embolic occlusion. No new angiographic findings were noted. Meanwhile, the patient’s vision in the left eye notably improved and gradually returned to normal on the 5th postprocedural day.

FLAIR (A, B) and T2-weighted (C, D) MR images show gyriform hyperintensities in both occipital cortices (arrows), larger on the right than on the left. No mass effect is noted. Diffusion imaging (E, F) does not show any restricted fluid motion.
Parameters for FLAIR match those used for Figure 1. Parameters for diffusion imaging: TR, 6000; TE, 103.1; FOV, 24; matrix, 100 × 100.
Discussion
Transient cortical blindness (TCB) is characterized by partial or complete loss of perceived vision, normal fundi, normal papillary reflexes, and unaltered extraocular movements (4, 5). The onset of TCB occurs from minutes up to 12 hours after angiography and is accompanied by headaches, mental state changes, memory loss, and, sometimes, denial of blindness. Symptoms may begin while the procedure is in progress or develop within 10 minutes of its completion. The return to normal vision may begin within the next few hours. In general, significant recovery occurs by 12 hours, although complete recovery may take as long as 5 days (5).
Cortical blindness due to intraarterial contrast material injection and a syndrome known as posterior reversible leukoencephalopathy (PRLE) appear to be related entities. Intraarterial contrast material apparently penetrates the blood-brain barrier by opening tight capillary junctions or enhancing endothelial pinocytosis (6). It then enters the cerebral cortex and adversely affects neuronal membranes. This type of neurotoxicity seems to be related to the chemical or ionic properties of the contrast medium as well as its hyperosmolarity, lipid solubility, and viscosity (5, 7). This adverse reaction has been reported for both ionic and nonionic contrast media (8) and is also mentioned on the product information. The toxicity is predominantly localized to the occipital lobes.
On the other hand, PRLE is a syndrome that is related to transplant immunosuppressive treatment, renal insufficiency, and hypertension (9). The sympathetic innervation of the vertebrobasilar arterial system is not as extensive or complete as that of the carotid arterial system; there is a relative lack of protective, sympathetically mediated arteriolar vasoconstriction during severe hypertension (10). This is thought to account for the predominance of posterior hemisphere lesions in eclampsia or hypertensive encephalopathy (9). Reversible edema, localized mainly to the occipital lobes, is a prominent feature. These edematous lesions often resolve upon control of blood pressure or reduction of immunosuppressive drugs. Clinical findings of visual impairment are similar to those seen in contrast-enhanced angiographic procedures. In one study of PRLE, nine of 15 patients developed visual symptoms, five of whom had cortical blindness, three showed homonymous hemianopia, and one had blurred vision (9). The neurologic symptoms resolved within 2 weeks. These similarities in the imaging and clinical findings of PRLE and cortical blindness following contrast material injections suggests they may share a common pathophysiology of disruption of the blood-brain barrier with resultant reversible injury to the occipital neuronal cortex exists. One of the possible common factors suggested is the release of endothelin, a peptide vasoconstrictor released by the endothelial cells of the brain (11). Endothelin release has been implicated in the pathophysiology of disorders associated with PRLE and has also been shown to increase human brain endothelial cell permeability in both PRLE and with the administration of radiographic contrast material.
CT findings of cases of cortical blindness secondary to contrast material injections have been frequently reported. These include hyperattenuated lesions in occipital and posterior parietal cortices and are thought to be secondary to contrast extravasation due to disruption of the blood-brain barrier following the angiographic procedure (4, 6). A repeat CT scan performed within the next 24–48 hours usually shows resolution of these findings. Case 2 showed a gyriform area of hyperattenuation in the left parieto-occipital cortex immediately following the angiographic procedure, which was not visualized on the MR imaging study performed the next day. Initial CT findings can also be absolutely normal, as seen in cases 1 and 3.
MR findings have not been frequently reported and include abnormal cortical T2 and FLAIR hyperintensities in the occipital and parietal cortices. Sometimes these lesions may be subtle, as seen in case 2, in which the initial CT scan showed a large abnormality in the left parieto-occipital cortex. Clinically, the patient improved quickly and was discharged. MR imaging performed just before discharge showed subtle T2 and FLAIR signal intensity abnormality in the inferior left occipital cortex. This would suggest that the initial CT abnormality had resolved and therefore was not definitely visualized on the subsequent MR imaging study. The absence of evidence of restricted fluid motion on the diffusion-weighted images in all cases seems to be an important finding, because this relatively excludes the possibility of acute ischemia secondary to shower of emboli during the angiographic procedure.
It seems that certain factors may increase the incidence of cortical blindness owing to angiographic procedures. All three patients had chronic hypertension, a factor that may increase susceptibility to osmotic disruption of the blood-brain barrier (12). Second, Omnipaque (Amersham Health, Inc., Princeton, NJ [300 mg/mL]) was used during the procedures as contrast media. Omnipaque is a monomeric nonionic contrast medium with an osmolality of 709 mosm/kg H2O. According to the records, the solution was not diluted with normal saline in any of the cases. Therefore, it is possible that the relatively higher osmolality of the contrast material solution (709 mosm/kg) when compared with that of blood (300 mosm/kg) may also have been a contributing factor to an increase in permeability of the blood-brain barrier, a phenomenon well known to occur with ionic contrast material solutions (6).
Conclusion
Unlike previously thought, cortical blindness after nonionic contrast medium administration does occur. We believe that hypertensive patients may be more susceptible to this complication, although this cannot be established with certainty. The period of blindness might last from a few hours to a few days. Although treatment with hydration, heparin, corticosteroids, and dextran is prudent in managing this condition, simple observation has proved equally effective in some other cases. There is no definite evidence to suggest that a certain treatment regimen improves the natural history of this disease, which is usually benign. Knowledge about this complication and relatively simple treatment are useful in effectively managing this condition. Physician recognition of this entity and reassurance of the patient are essential to a favorable outcome.
References
- Received February 21, 2003.
- Accepted after revision May 19, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Nationwide multicenter experience of contrast-induced encephalopathy following neurointervention: clinical course and outcomes
- Illustrative case of prosopagnosia after diagnostic cerebral angiography and systematic review of transient cortical blindness after cerebral angiography
- Cerebral catheter angiography and its complications
- Delayed leucoencephalopathy after coil embolisation of unruptured cerebral aneurysm