
Abstract
BACKGROUND AND PURPOSE: Early reocclusion of recanalized arteries has been observed after thrombolysis for acute coronary occlusion and has been attributed to platelet activation after exposure to thrombolytic agents. We conducted a retrospective study to determine the rate of reocclusion during intra-arterial thrombolysis for acute ischemic stroke and the effect of reocclusion on functional outcome.
METHODS: Patients treated for acute ischemic stroke at our center between September 2000 and May 2002 received a maximum total dose of 4 U of reteplase intra-arterially in 1-U increments via superselective catheterization. Pharmacologic thrombolysis was supplemented by mechanical thrombolysis with balloon angioplasty or snare manipulation at the occlusion site. Angiography was performed after each unit of reteplase or mechanical maneuver, and the images were interpreted by a blinded reviewer. Reocclusion was defined as partial or complete initial recanalization with occlusion recurring at the same site as documented by angiography during the endovascular treatment. Reocclusions were treated by further pharmacologic and/or mechanical thrombolysis according to the discretion of the treating physician. Clinical evaluations were performed before and 24 hr, 7 to 10 days, and 1 to 3 months after treatment.
RESULTS: Forty-six consecutive patients underwent intra-arterial thrombolysis. Reocclusion was observed in eight (17%). Among these patients, initial sites of occlusion were in the following arteries: intracranial internal carotid artery (n = 2), M1 segment of the middle cerebral artery (n = 3), M1 and M2 segments of the middle cerebral artery (n = 2), and basilar artery (n = 1). The mean initial National Institutes of Health Scale score for these eight patients was 23.3 ± 6.2; mean time from symptom onset to treatment was 4.4 ± 1.2 hr. The reocclusions were treated by using additional doses of reteplase alone (n = 1), reteplase with snare maneuver and/or angioplasty (n = 5), reteplase with angioplasty or snare and then stent placement (n = 1), and angioplasty with stent placement (n = 1). The reocclusions resolved in six of eight patients after further treatment. Six patients died and two survived but were severely disabled at 1 month (modified Rankin Scale scores of 4 and 5, respectively). Independent functional outcome scores (modified Rankin Scale scores of 0–2) were significantly lower among patients with angiographically shown reocclusion than in those without (0 of 8 versus 17 of 38, P = .02).
CONCLUSION: Reocclusion occurs relatively frequently during intra-arterial thrombolysis for ischemic stroke and seems to be associated with poor clinical outcomes.
Clinical deterioration after initial improvement is often observed in patients treated with IV administered thrombolysis for ischemic stroke (1). Grotta et al (1), reporting on the incidence of such clinical deterioration after initial neurologic improvement with recombinant tissue-plasminogen activator (rt-PA) treatment in the National Institute of Neurologic Disorders and Stroke rt-PA Stroke Trial, suggested that this phenomenon might be a surrogate marker of cerebral arterial reocclusion. In their report, deterioration was defined as any 2-point increase in the National Institutes of Health Stroke Scale (NIHSS) score after an initial 2-point decrease after treatment. Early deterioration after initial improvement was identified in 81 (13%) of 624 patients; 44 had received rt-PA, and 37 had received placebo. Deterioration occurred more often in patients with higher baseline NIHSS scores and was strongly associated with poor outcome at 3 months (1). Subsequent investigations using transcranial Doppler ultrasonography monitoring during IV administered thrombolysis have supported the role of arterial reocclusion as a major contributor to secondary deterioration in patients with ischemic stroke (2, 3).
We conducted a retrospective study involving a review of clinical and radiographic data that had been collected prospectively as part of a study of patients undergoing intra-arterial thrombolysis for acute ischemic stroke (4). Our primary objective was to determine the rate of reocclusion of initially recanalized arteries by review of serial angiographic images. We also sought to identify demographic and clinical factors associated with reocclusion, especially functional outcome.
Methods
Patients and Techniques
Between September 2000 and May 2002, all patients with acute ischemic stroke referred to our institution for intra-arterial thrombolysis were entered into the aforementioned study. According to the study protocol, patients were to receive low dose intra-arterial reteplase and low dose IV administered heparin in combination with aggressive mechanical disruption of the clot if pharmacologic thrombolysis alone was ineffective for recanalization of arterial occlusion. Informed consent was obtained from a relative of each patient. The protocols for collection and reporting of data were reviewed and approved by the Institutional Review Board. The patients were deemed to be poor candidates for IV administered alteplase therapy by the referring neurologist for at least one of the following reasons (5, 6): 1) severity of stroke (severe neurologic deficits with an initial NIHSS score ≥16), 2) delay in presentation to the emergency department (≥3 hr after symptom onset), or 3) recent (within 2 weeks of stroke onset) major surgical procedure. Patients who presented after the 3-hr window for IV administered thrombolysis were considered for intra-arterial thrombolysis only if immediately performed CT did not show evidence of early infarction in more than one-third of the affected blood vessel distribution. Each patient was evaluated by a neurologist before and 24 hr, 7 to 10 days, and 1 to 3 months after treatment. Cranial CT was performed at presentation and immediately and 24 hr after completion of intra-arterial reteplase administration.
Endovascular Treatment Protocol
The endovascular treatment protocol has been previously described with respect to the first 19 consecutive patients in this study (4). Briefly, a 6-French guide catheter was placed in the internal carotid artery or vertebral artery proximal to the occlusion site. Each patient received IV administered heparin (30 U/kg of body weight) to achieve an activated coagulation time of >200 s. A 2.3-French microcatheter was advanced to the vessel occlusion in the proximity of the thrombus through the guide catheter and over a microguidewire. Reteplase (Retavase; Centocor, Inc., Malvern, PA; 1 U per 10 mL of sterile normal saline) was then infused at a rate of approximately 1 U during the course of 5 min. Angiography was performed after the delivery of each unit of reteplase to evaluate the status of recanalization. If partial or complete occlusion persisted after the first 2 U of reteplase was administered, mechanical disruption of the clot was undertaken with balloon angioplasty or a snare maneuver. Angioplasty was performed by using a Cross Sail (Guidant; Advanced Cardiovascular Inc, Temecula, CA), Open Sail (Guidant), or Ninja (Cordis, Miami Lakes, FL) angioplasty balloon catheter. Snare maneuvers were performed by introducing a 4-mm snare (Amplatz Goose-Neck Microsnare; Microvena, White Bear Lake, MN) through the 2.3-French microcatheter and advanced into the clot matrix. Multiple passes were made through the clot by using the fully extended loop of the snare to fragment, but not capture, the clot. Additional reteplase was administered to achieve complete recanalization until a maximum dose of 4 U had been administered. IV administered heparin was discontinued when the procedure was complete. After the first 19 patients were treated, the mechanical maneuvers were used more aggressively and stent placement was considered as an option. Use of angioplasty and snare were considered earlier in the procedure, and occasionally, both were used for the same lesion. However, 4 U of reteplase was the maximum dose used throughout the study period. The treatment of recurrent angiographic occlusion occurring after partial or complete initial recanalization was determined by the treating physician and varied depending on the situation.
Evaluation of Imaging Data
Immediate pre- and post-treatment angiographic images were obtained and graded by using a new grading scheme proposed by one of the investigators on the basis of the location of the occlusion and collateral supply to the affected regions (Table 1) (7). The grading scheme can be used to predict trends in clinical outcome in terms of functional recovery or death after thrombolysis. The scheme has six grades, with grade 0 denoting no occlusion and grade 5 denoting complete occlusion of either the internal carotid artery or the basilar artery. As previously mentioned, angiograms were obtained after each unit of reteplase was administered. Angiograms were also obtained immediately before and after every mechanical maneuver (angioplasty, snare, or stent placement). An investigator blinded to the clinical characteristics and outcomes of the patients reviewed and graded all angiographic images. Reocclusion was defined as angiographic documentation of initial complete or partial recanalization with occlusion recurring at the same site during the course of the endovascular treatment.
Grades of increasing severity of arterial occlusion
Postdischarge Outcome
Outcomes were determined by use of the modified Rankin Scale (8–10) for surviving patients 1 to 3 months after the procedure, either at the time of a clinic visit or during a telephone interview. Patients were classified as functionally independent if the modified Rankin Scale score was ≤2.
Statistical Analysis
Age, sex, mean time to treatment, occlusion site, angiographic grade initially and at the conclusion of treatment, NIHSS score initially and at 7 days, and modified Rankin Scale score at 1 to 3 months were compared among patients with and without angiographically shown reocclusion. Continuous and categorical variables were presented as means with SDs and frequencies, respectively. Means and frequencies were compared by using analysis of variance and χ2 methods, respectively (JMP statistical software, Cary, NC).
Results
A total of 46 patients underwent intra-arterial thrombolysis for acute ischemic stroke (mean age 70.4 ± 16.1 years; 27 were men). Initial NIHSS scores ranged from 5 to 43. An average of 21.2 serial angiograms were obtained per patient.
Angiographically shown reocclusion was observed in eight (17%) patients. Among these patients, initial sites of occlusion were in the following arteries: intracranial internal carotid artery (n = 2), M1 segment of the middle cerebral artery (n = 3), M1 and M2 segments of the middle cerebral artery (n = 2), and basilar artery (n = 1) (Table 2). The mean initial NIHSS score was 23.3 ± 6.2 (mean ± SD); the mean time from onset of symptoms to treatment was 4.4 ± 1.2 hr. Two examples of angiographically shown reocclusion (patients 2 and 4) are provided in Figures 1 and 2. Arterial reocclusions were treated by use of an additional dose of reteplase alone (n = 1), reteplase with snare maneuver and/or angioplasty (n = 5), reteplase with angioplasty or snare and then stent placement (n = 1), and angioplasty plus stent placement (n = 1). The reocclusion resolved partially in six of eight patients after additional treatment. Of the eight patients, six died and two survived with severe disability at 1 to 3 months after treatment (modified Rankin Scale scores of 4 and 5, respectively).

Patient 2.
A, Cerebral angiogram shows occlusion of the right middle cerebral artery (M1 segment, grade 3A).
B, Partial recanalization of the M1 and M2 segments is observed after the administration of 2 U of reteplase.
C, Reocclusion is observed involving the M2 segment of the middle cerebral artery.
D, Recanalization is observed in the middle cerebral artery after administration of an additional 1 U of reteplase.

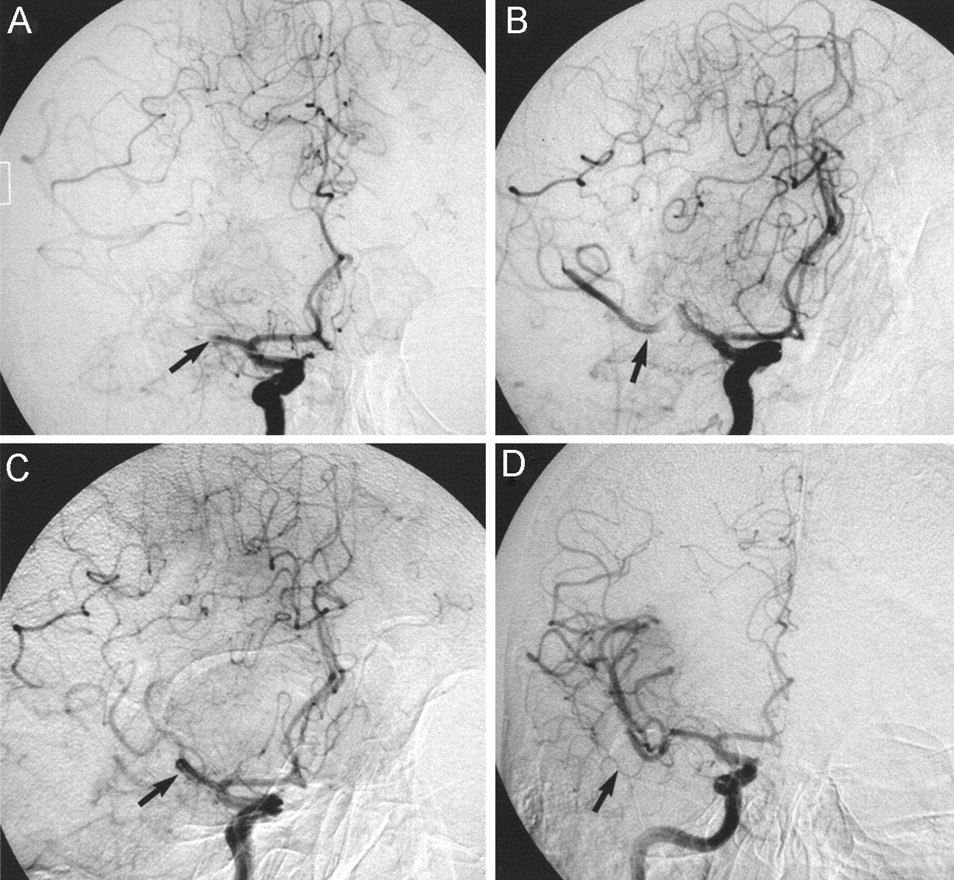
Patient 4.
A, Cerebral angiogram shows occlusion of the right internal carotid artery (supraclinoid segment, grade 5).
B, Recanalization is observed after administration of thrombolytics and snare maneuver. The filling defect at the junction of the internal carotid and middle cerebral arteries (arrow) indicates the presence of residual thrombus.
C, Reocclusion of the supraclinoid segment of the internal carotid artery is observed after administration of further thrombolytics.
D, Recanalization of the middle cerebral artery after stent placement in the M1 segment of the middle cerebral artery.
Clinical characteristics of patients with acute ischemic stroke for whom angiography showed reocclusion after initial recanalization
No significant differences were noted in the demographic or clinical characteristics of the eight patients who did and the 38 who did not develop angiographically shown reocclusion (Table 3). The mean initial NIHSS score was similar in the two groups (23.3 ± 6.2 versus 22 ± 8.7, P = .7). The initial angiographic severity of occlusion, as determined by the grading scheme, was similar in both groups. Although there were no significant overall differences in final angiographic grades between the groups, complete recanalization (grade 0) was achieved in more patients for whom reocclusion was not shown (13 of 38 versus 0 of 8). The rate of independent functional outcome (modified Rankin Scale score of 0–2) was significantly lower in the group with angiographically shown reocclusion (0 of 8 versus 17 of 38, P = .02). The rate of reocclusion was not significantly different among the first 19 patients compared with the latter 27 patients in whom more aggressive mechanical disruption of thrombus was performed (1 of 19 compared with 7 of 27, P = .1).
Comparison of demographic and clinical characteristics and outcomes for patients whose angiograms did and did not reveal reocclusion
Discussion
Serial angiography performed throughout the endovascular procedure provides a unique opportunity to evaluate dynamic changes at the site of occlusion during thrombolysis. We observed a high rate (17%) of early reocclusion among patients treated with endovascular therapy. Partial recanalization was ultimately achieved in six of eight patients with reocclusion. At follow-up evaluation, 17 of 38 patients without angiographically shown reocclusion were functionally independent in contrast to none of the eight patients with reocclusion. This observation suggests that reocclusion adversely affects the outcome of endovascular therapy for ischemic stroke.
Rate and Timing of Reocclusion after Thrombolysis in Ischemic Stroke
Sixty consecutive patients with stroke treated with IV administered alteplase within 3 hr of symptom onset and with MCA occlusion shown by pretreatment transcranial Doppler ultrasonography were monitored for ≤2 hr after alteplase bolus by Alexandrov and Grotta (2). Reocclusion was defined as a decrease in Thrombolysis in Brain Ischemia Grading Scheme flow by ≥1 grade and no hemorrhage shown by repeat CT. Recanalization was complete in 18 (30%), partial in 29 (48%), and absent in 13 (22%) patients. Reocclusion occurred in 16 (34%) of 47 patients with any initial recanalization. Specifically, reocclusion occurred in four (22%) of 18 patients with complete recanalization and in 12 (41%) of 29 patients with partial recanalization. Reocclusion was detected in four patients before administration of the alteplase bolus, in three by 30 min after the bolus had been administered, in three by the end of the infusion, and in six by 60 to 120 min after the bolus. Deterioration after initial improvement occurred in eight (50%) of 16 patients with reocclusion after any recanalization compared with 10% of patients who did not develop reocclusion (stable recanalization). At 3 months, good outcomes (modified Rankin Scale scores of 0–1) were achieved by 33% of patients with reocclusion compared with 50% of patients with stable recanalization. The mortality rate was 33% in patients with reocclusion and 8% in patients with stable recanalization.
Mechanism of Reocclusion
We have observed reocclusion in experimental models of ischemic stroke treated with intra-arterial thrombolysis (reteplase), even without mechanical disruption of clot (11, 12). These experimental findings in conjunction with our clinical observations suggest that clot formation and lysis is a very dynamic process. Several factors are involved in the reformation of thrombus at the site of occlusion, as studied in the coronary circulation (13). The plasmin generated by thrombolysis leads to the production of thrombin through several mechanisms (13). Thrombin is a potent platelet activator and converts fibrinogen to fibrin. Increased platelet activation is shown after thrombolysis (14–16). The platelets are responsible for counter-regulatory secretion of native t-PA inhibitor 1, which partially neutralizes the uptake of rt-PA introduced in an attempt to dissolve the thrombus, making the fibrinolytic agent, in effect, prothrombotic (17). Aggregating platelets provide a phospholipid surface for cleavage of prothrombin to thrombin (18). The use of mechanical disruption (such as balloon angioplasty, snare manipulation, or stent placement) may lead to disruption of atherosclerotic plaques or endothelial erosion that triggers platelet activation, adherence and aggregation, and also the exposure of tissue factor, which, in turn, activates the clotting cascade (13). The rate of reocclusion was not significantly different among the initial and subsequent group of patients in whom more aggressive mechanical disruption was considered but the uncontrolled nature of the observation limits definitive conclusion. An occlusive lesion consisting of thrombus superimposed on atherosclerotic plaque is more vulnerable to reocclusion. Dissolution of the thrombus leads to exposure of the thrombogenic plaque surface, thereby providing a template for the reformation of thrombus.
Adverse Effect of Reocclusion on Outcome
Several mechanisms may explain the association of reocclusion with the poor outcomes encountered in our study. Stable recanalization is less likely to occur in the setting of angiographically shown reocclusion. In addition, the eventual time required to reestablish flow is much longer in vessels that show reocclusion. This additional time is attributed to performing further angioplasty dilations and snare manipulations as well as stent deployment. We recorded angiographic data only for the duration of the procedure. The possibility that patients who developed initial reocclusion developed another occlusion in the hours after the procedure can be another explanation for poor outcome. Reocclusion may represent an intrinsically active thrombotic state with consequences in both the macro- and microvasculature. Platelet activation with subsequent stasis of flow through the microvascular circulation has been shown to worsen ischemic injury in experimental models (19).
Strategies to Prevent Reocclusion
After successful reperfusion, the target artery reoccludes in 5% to 15% of patients with myocardial infarction (14). The mortality rate is doubled in patients with reocclusion, and complications of left ventricular dysfunction, including heart failure and dysrhythmias, are markedly increased. Various strategies have been applied to reduce the rate of reocclusion in acute myocardial infarction. Most prominent are strategies directed toward inhibiting platelet activation (20). Two dose-range studies, Thrombolysis in Myocardial Infraction 14 (21) and Strategies for Patency Enhancement in the Emergency Department (22), evaluated the efficacy of thrombolytic agents in combination with platelet glycoprotein IIb-IIIa inhibitors. In both protocols, dose ranging with fibrinolytic therapy yielded similar results. The combination of essentially half-dose lytic with full-dose abciximab seemed superior to full-dose lytic alone in achieving improved perfusion at 60 and 90 min. Whether this effect is the result of a higher early perfusion rate or a lower reocclusion rate remains uncertain. The sample sizes are too small to provide accurate estimates of either the true rate of reocclusion or the longer term clinical implications of these sequelae. In the Global Use of Strategies to Open Occluded Coronary Arteries V trial (23), 16,588 patients with ST segment elevation myocardial infarction were randomized to receive either standard dose reteplase or half-dose reteplase in conjunction with full dose abciximab. The 1-month mortality rates were similar in the two treatment groups. The rate of reinfarction was lower in the combination treatment group, but the benefit was obscured by increased nonintracranial bleeding complications.
Antithrombotic therapy has been proposed as an adjunct to thrombolytic therapy in the treatment of patients with myocardial infarction. We used a low dose IV administered heparin bolus (30 U/kg) at the time of thrombolysis for acute ischemic stroke. For six of the eight patients with reocclusion after initial recanalization, activated coagulation time measurements were available and were in therapeutic ranges, as specified in a previous report (24). Whether higher doses of heparin or low molecular weight heparin might have led to a reduction in the rate of reocclusion remains undetermined. In the Heparin and Aspirin Reperfusion Therapy II study (25), 400 patients were randomized to receive accelerated alteplase therapy along with either enoxaprin or unfractionated heparin for 3 days. Reocclusion at 5 to 7 days occurred in 5.9% of patients receiving enoxaprin and 9.8% of those receiving unfractionated heparin. Other antithrombotic strategies, such as selective inhibitors of factor X and thrombin, are presently being evaluated as adjunctive therapy to thrombolysis (26).
Conclusion
Our review suggests that reocclusion occurs relatively frequently during intra-arterial thrombolysis with mechanical disruption of thrombus for ischemic stroke and seems to be associated with poor clinical outcome. The results may not be representative of patients undergoing pharmacologic thrombolysis alone. Further studies are required to develop strategies to reduce the rate of reocclusion during endovascular treatment of acute ischemic stroke.
Acknowledgments
The authors thank Paul H. Dressel for preparation of the illustrations. Dr. Hopkins receives research support from and is a consultant for Cordis; in addition, he has a financial interest in Medtronic. Dr. Qureshi has received grant support from Centocor Inc., Malvern, PA, and COR Therapeutics, South San Francisco, CA.
References
- Received May 6, 2003.
- Accepted after revision July 29, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of dual antiplatelet therapy on patients with minor stroke after thrombolysis: a systematic review and meta-analysis
- Reciprocal Interaction of 24-Hour Blood Pressure Variability and Systolic Blood Pressure on Outcome in Stroke Thrombolysis
- Importance of truncal-type occlusion in stentriever-based thrombectomy for acute stroke
- Incidence and Clinical Significance of Acute Reocclusion after Emergent Angioplasty or Stenting for Underlying Intracranial Stenosis in Patients with Acute Stroke
- Infarct growth despite full reperfusion in endovascular therapy for acute ischemic stroke
- Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association
- Microcatheter to Recanalization (Procedure Time) Predicts Outcomes in Endovascular Treatment in Patients with Acute Ischemic Stroke: When Do We Stop?
- Periprocedural antithrombotic strategies in acute ischemic stroke interventional therapy
- Multimodal endovascular reperfusion therapies: Adjunctive antithrombotic agents in acute stroke
- Indications for the performance of intracranial endovascular neurointerventional procedures. A scientific statement from the American Heart Association Council on Cardiovascular Radiology and Intervention, Stroke Council, Council on Cardiovascular Surgery and Anesthesia, Interdisciplinary Council on Peripheral Vascular Disease, and Interdisciplinary Council on Quality of Care and Outcomes Research
- Occurrence and Predictors of Futile Recanalization following Endovascular Treatment among Patients with Acute Ischemic Stroke: A Multicenter Study
- Intra-Arterial Recanalization Techniques for Patients 80 Years or Older with Acute Ischemic Stroke: Pooled Analysis from 4 Prospective Studies
- Indications for the Performance of Intracranial Endovascular Neurointerventional Procedures: A Scientific Statement From the American Heart Association Council on Cardiovascular Radiology and Intervention, Stroke Council, Council on Cardiovascular Surgery and Anesthesia, Interdisciplinary Council on Peripheral Vascular Disease, and Interdisciplinary Council on Quality of Care and Outcomes Research
- Endovascular Approaches to Acute Stroke, Part 1: Drugs, Devices, and Data
- Factor V Leiden Mutation in Reocclusion After Intra-Arterial Thrombolysis
- Interventional Acute Ischemic Stroke Therapy With Intracranial Self-Expanding Stent
- Interventional Management of Stroke
- Intra-arterial therapies for acute ischemic stroke
- Self-Expanding Stents for Recanalization of Acute Cerebrovascular Occlusions
- Multimodal Reperfusion Therapy for Acute Ischemic Stroke: Factors Predicting Vessel Recanalization
- Aggressive Therapy With Intravenous Abciximab and Intra-Arterial rtPA and Additional PTA/Stenting Improves Clinical Outcome in Acute Vertebrobasilar Occlusion: Combined Local Fibrinolysis and Intravenous Abciximab in Acute Vertebrobasilar Stroke Treatment (FAST): Results of a Multicenter Study
- Reocclusion Rates After Intra-Arterial Thrombolysis for Acute Stroke