
Abstract
Summary: We present two patients with posterior tilting of a basilar tip aneurysm after selective coiling. The cause and significance of this finding are discussed.
Unlike surgery, where clipping and manipulation of an aneurysm often alters its orientation, selective endovascular treatment should leave the aneurysm’s morphology and orientation intact. We report our observations of two patients with large ruptured basilar apex aneurysms in which there was a significant change in the aneurysm’s orientation following endovascular treatment with detachable coils.
Patient 1
A 53-year-old man with no significant medical history presented with the sudden onset of headache without neurologic deficit (Hunt and Hess grade I subarachnoid hemorrhage). Angiography showed a large basilar tip aneurysm consistent with the bleeding pattern seen at CT. On the same day, selective endovascular treatment of the aneurysm with Guglielmi detachable coils (GDC; Boston Scientific/Neurovascular, Fremont, CA; Fig 1A and B) was performed with satisfactory obliteration of the aneurysm without clinical complication. The patient was discharged neurologically intact 6 days after treatment.

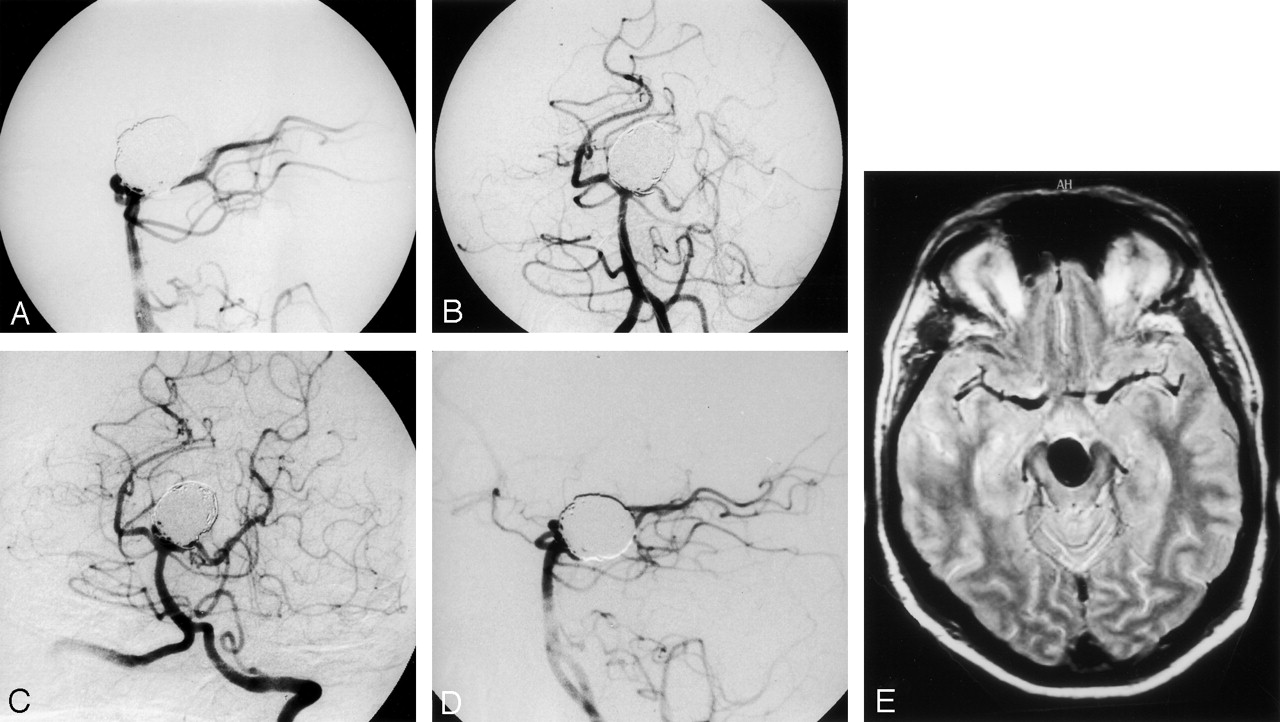
Case 1.
A and B, Immediate postembolization left vertebral angiogram. Lateral (A) and Towne’s (B) views show complete obliteration of the basilar tip aneurysm. (Note small coil protrusion in left P1 with a small clot.)
C and D, Left vertebral angiogram performed 5 months after embolization. Towne’s view (C) shows a small recurrence at the neck. Lateral view (D) shows backward tilting of the aneurysm when compared with the initial angiogram.
E, Axial proton density–weighted turbo spin-echo image (TR, 3500; TE, 22) 8 months after embolization shows aneurysm relationship with the interpedoncular cistern.
Two months later, the patient complained of intermittent diplopia, which subsequently deteriorated over the next several weeks. Neuro-ophthalmologic examination showed subtle left third nerve palsy. Angiography performed 5 (Fig 1C and D) and 8 months post embolization showed a slight recurrence of the aneurysm. The overall configuration of the recurrence was stable over the 3-month interval. In addition to the recurrence, however, an obvious posterior tilt and ptosis of the aneurysm was seen when compared with findings at initial angiography. MR imaging performed 8 months after treatment showed the aneurysm positioned in the interpedoncular cistern (Fig 1E).
Patient 2
A 42-year-old woman with acute onset of headache without neurologic deficit was emergently referred to our institution for embolization of a ruptured basilar tip aneurysm (Hunt and Hess grade I subarachnoid hemorrhage). Selective GDC embolization was performed the day after the hemorrhage. Because of coil protrusion toward the left P1 segment, the patient continued to receive heparin for 2 days after embolization (Fig 2A and B). Several hours after heparin was withdrawn, the patient developed a left internuclear ophthalmoplegia with left hemifacial numbness. Heparin was resumed for 2 additional days, and aspirin was administered for 3 months. A repeat angiogram failed to show thrombotic or embolic complications. The deficit resolved within 12 hours. MR imaging performed the next day showed a punctiform left paramedian mesencephalic infarct. Follow-up angiography 3 months later documented a small inferoanterior recurrence. A 6-month follow-up angiogram showed an increase in the size of the residual aneurysm, which was subsequently retreated by using GDC embolization. A small residual neck was still visible after retreatment. A 1-year follow-up angiogram showed regrowth of the aneurysm. Retreatment was attempted, but it was unsuccessful. The aneurysmal recurrence was stable over 30 months. Ultimately, the recurrence was retreated by using the Trispan neck-bridge device (Boston Scientific/Neurovascular) and GDC embolization. Review of the angiograms over a 3-year interval showed progressive backward tilting of the aneurysm and posterior bending of the basilar artery (Fig 2C–E). Some change in the aneurysm’s orientation was already present at 6 months and subsequently increased. The patient remained asymptomatic.

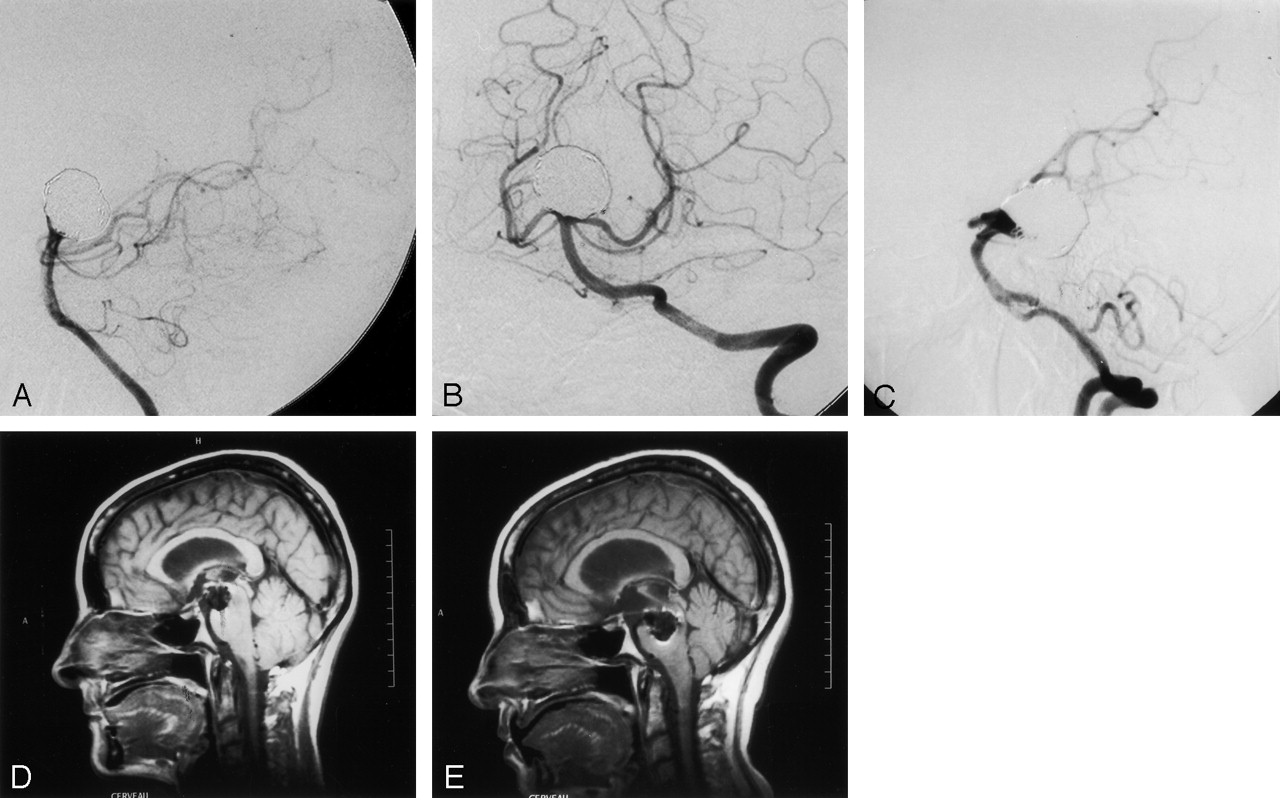
Case 2.
A and B, Immediate postembolization left vertebral angiogram. Lateral (A) and Towne’s left anterior oblique (B) views show complete obliteration of basilar tip aneurysm.
C, Left vertebral angiogram obtained 30 months after initial embolization. Lateral view shows backward tilting of the aneurysm and posterior bending of the basilar trunk with an anterior recurrence of the aneurysm.
D and E, MR sagittal T1 spin-echo (TR, 595; TE, 14) image obtained 36 hours (D) and 3 years (E) after initial embolization. The posterior and downward migration of the coil mass is nicely depicted. On the final MR image (E), note the enlargement of the lateral and third ventricles with anterior compression of the aqueduct of sylvius. Note the recurrence of the anterior portion of the aneurysm.
Discussion
Surgical intervention for basilar tip aneurysm is difficult and is associated with high morbidity. The challenge arises from operating in a location deep in the brain, often with limited surgical accessibility and in association with delicate anatomic structures in close proximity to the lesion (1). In the early 1990s, controlled detachable coils were introduced as a less invasive alternative for treating aneurysms. The location of the aneurysm is less important than the morphology of the aneurysm, when one considers patients for endovascular therapy. In general, basilar tip aneurysms are favorable for microcatherization and therapy with coils (2, 3). Surgical complications from brain and nerve retraction are avoided with endovascular approaches; however, selective embolization can be associated with other immediate and long-term complications, primarily hemorrhagic or ischemic strokes or both (2–4).
After selective embolization, the two patients demonstrated a change in orientation of the aneurysm. Whether it has to be considered as an incidental finding without clinical implication might be answered by our first patient. In this case, we believe that tilting of the aneurysm led to compression of the left third nerve, resulting in a new, progressive unilateral third nerve palsy.
In the second patient, angiography performed over a 3-year time span demonstrated tilting of the aneurysm with marked posterior bending of the basilar trunk. The final MR image showed enlargement of the lateral and third ventricles, which were likely due to anterior compression of the aqueduct of sylvius by the aneurysm (Fig 2E). The patient, however, remained asymptomatic.
It is not known whether the dramatic change in orientation of aneurysms after endovascular therapy described in this report could occur in another location. The fact that the basilar tip is anatomically unrestricted, “floating in the interpedoncular cistern,” may make this structure susceptible to reorientation.
There are several hypothesis that could explain these morphologic changes. A change in the orientation of the hemodynamic inflow away from the fundus could lead to reorientation of the aneurysm. The “supportive” nature of inflowing pressurized blood is eliminated by the presence of the coils, thus allowing the aneurysm to “fall.” Because there is no vasovasorium in intracranial arteries, the walls of nongiant aneurysms depend on flow within the aneurysm for their viability. As a wall degenerates, there is reduced support for the coil mass, which could lead to reorientation. Another possibility is that the pulsatile flow into the anteriorly situated residual aneurysm accounts for the reorientation of the aneurysm. A final possibility is that the weight of the coils themselves leads to ptosis and reorientation based on added weight in the aneurysm fundus.
Conclusion
With the endovascular approach for the treatment of intracranial aneurysm, the endocranial environment adjacent to the aneurysm is theoretically unmodified. Coils within an aneurysm usually do not change the morphology of the aneurysm unless there is significant recanalization with subsequent aneurysmal growth. We have presented two patients whose aneurysms demonstrated fundal ptosis after endovascular embolization. This interesting finding, which seems to be rare, can have clinical repercussions, as demonstrated in the case of our first patient. It is not known whether such a change in orientation could be present in other locations. The anatomic environment of the basilar artery may make it more prone to fundal ptosis postembolization than other vessels.
- Received May 12, 2003.
- Accepted after revision June 22, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}