
Abstract
Summary: Localized amyloidosis is an uncommon benign disorder. The purpose of this report is to present the case of a 21-year-old man who had localized amyloidosis simultaneously involving the sinonasal cavities and the larynx. The rarer sinonasal lesion demonstrated CT findings of adjacent “fluffy” bone changes, possibly representing a new finding suggestive of this disorder. At MR imaging, the amyloid had signal intensity similar to that of skeletal muscle on T1- and T2-weighted images. After contrast material administration, the amyloid enhanced at most minimally, but peripheral enhancement about the mass was present. The importance of this case lies in the multifocal presentation of this uncommon disorder, and the imaging findings herein may provide a new sign of this paranasal sinus disease.
Amyloidosis is characterized by extracellular deposits of amyloid (1). Although uncommon, about 150 cases of amyloidosis have been documented since 1935 in the otolaryngology literature (2–5). There has, however, been a paucity of descriptions of its imaging findings in the head and neck (6). The purpose of this report is to present the CT and MR findings of this rare disorder concurrently involving the sinonasal cavities and the larynx.
Case Report
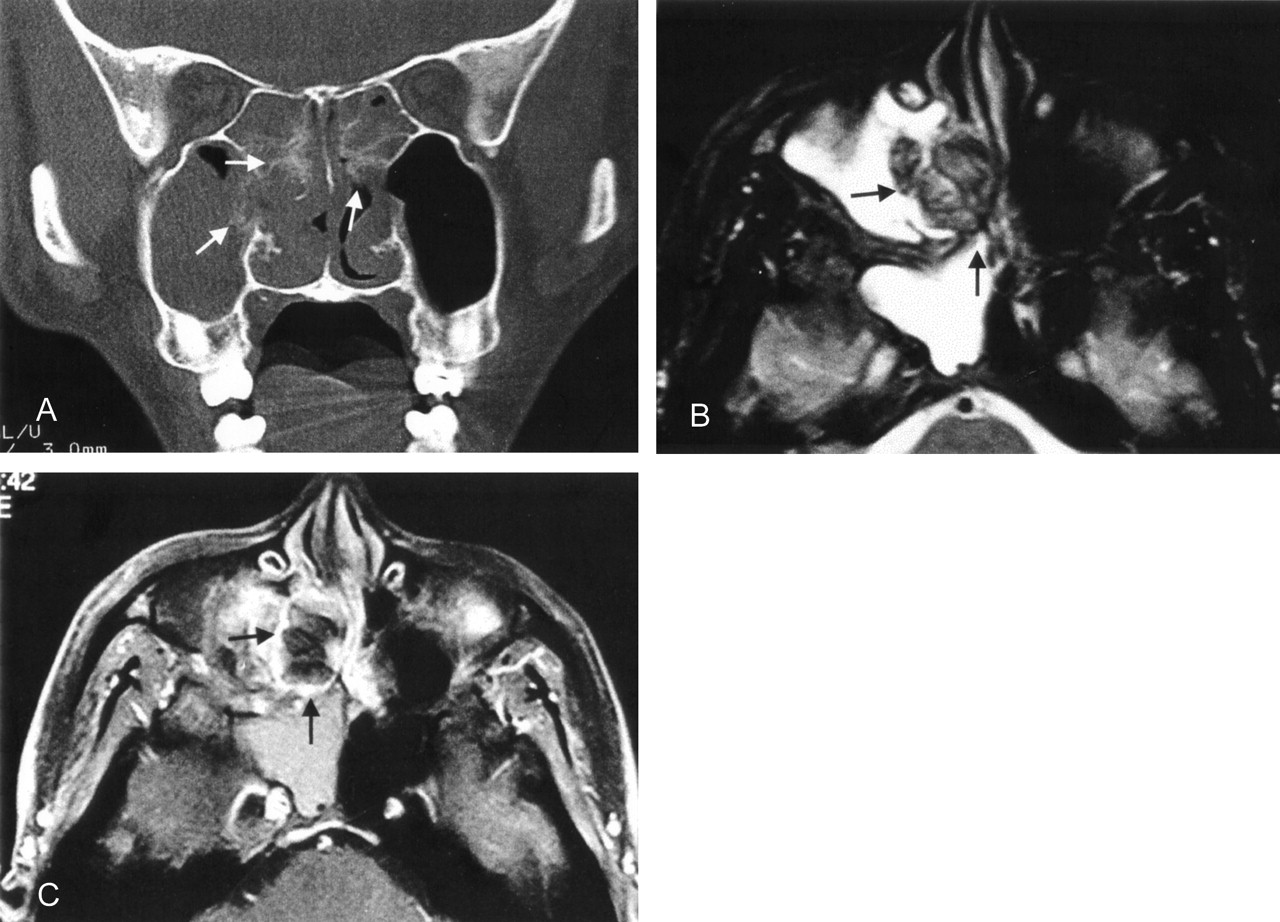
A 21-year-old man presented to the ear, nose, and throat clinic with a 1-year history of slowly progressive nasal stuffiness and dysphonia. Clinical examination demonstrated whitish, ulcerative, and swollen nasal conchae with serous secretions present in the adjacent osteomeatal infundibulum, ethmoid, and maxillary sinuses. Laryngoscopy disclosed a submucosal firm mass involving the left false fold and effacing the ipsilateral laryngeal ventricle. The patient denied any history of familial or hereditary disease or any notable allergies. CT and MR imaging studies were performed. The paranasal sinus CT showed that the affected bony conchae and sinus walls had a “fluffy” and somewhat hyperplastic reaction adjacent to the soft tissue mass that filled both nasal fossae (right greater than left) and the ethmoid sinuses (Fig 1A). At MR imaging, the lesion had low to intermediate signal intensity on both T1- and T2-weighted images and demonstrated peripheral enhancement on the contrast-enhanced study. The remaining soft tissues within the paranasal sinuses had high T2-weighted signal intensity, which is typical of obstructive secretions (Fig 1B and C). The MR study demonstrated a submucosal lesion in the larynx involving the left false cord and obliteration of the left laryngeal ventricle. The lesion also had low T1- and T2-weighted signal intensities and enhanced primarily along its periphery (Fig 2 A and B). The patient underwent surgical excision of both lesions and had an uneventful recovery. Histopathologic analysis with Congo Red stain confirmed the diagnosis of amyloidosis. Immunohistochemical examination revealed a positive staining pattern for six and eight light chain immunoglobulins. A thorough systemic workup for additional amyloid deposits revealed no evidence of other disease.

A, Coronal CT viewed at wide window settings shows fluffy calcifications (arrows) of the turbinates and sinus walls adjacent to a nasal mass. Soft tissue windowing shows entrapped secretions and inflammatory mucosal thickening in the right maxillary and sphenoid sinuses.
B, Axial T2-weighted MR image (TR/TE, 3000/96 ms) through the paranasal sinuses, demonstrates a predominantly hypointense lesion (arrows) involving the right sinonasal cavity. In contrast, entrapped secretions in the right maxillary and sphenoid sinuses have high T2-weighted signal intensity.
C, Contrast-enhanced, axial fat-suppressed T1-weighted image (TR/TE, 540/12 ms) demonstrates peripheral enhancement of the lesion (arrows).

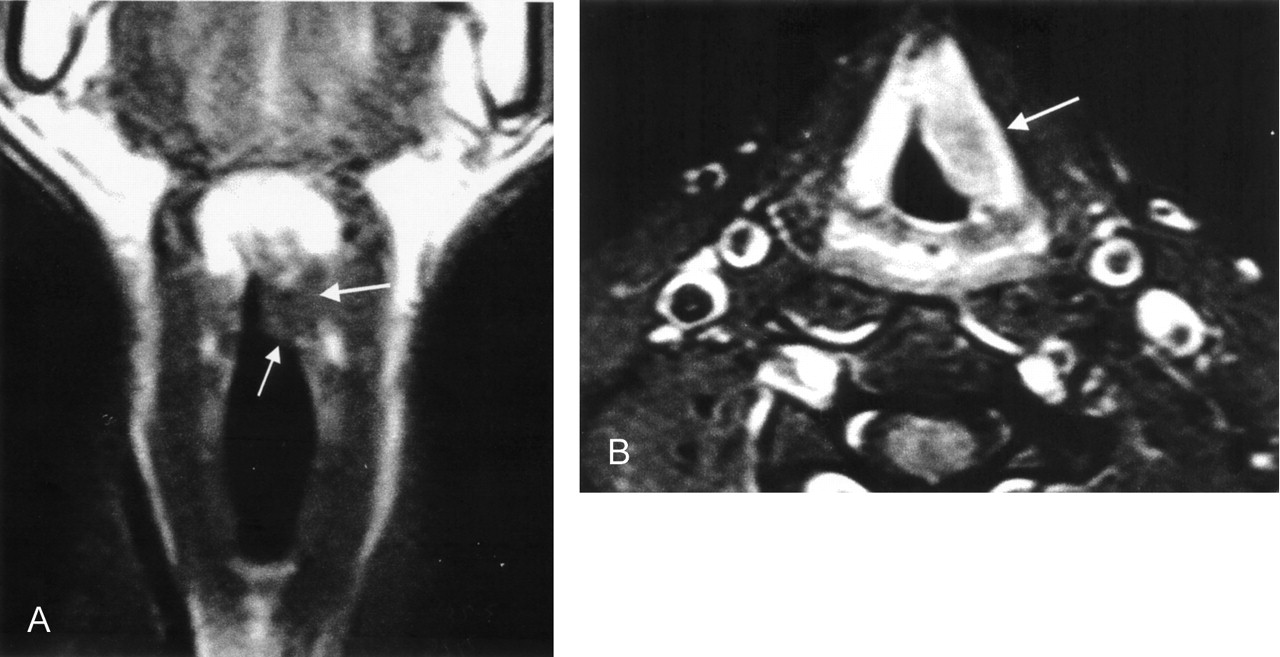
A, Coronal T1-weighted image through the larynx demonstrates a mass (arrows) involving the left false vocal cord with hypointensity similar to adjacent muscle. The lesion also has low signal intensity on T2-weighted images (not shown).
B, Contrast-enhanced axial T1-weighted, fat-suppressed image demonstrates a minimally enhanced submucosal lesion (arrow) surrounded by intense mucosal enhancement.
Discussion
Amyloidosis refers to a heterogeneous group of disorders that share the idiopathic extracellular accumulation of amyloid in tissues. If the deposition is extensive, it may interfere with organ or tissue function and even lead to death (7). Amyloid is a linear, nonbranching, fibrillar proteinaceous material that is arranged in a highly organized fashion (1). Amyloidosis is now classified as primary amyloidosis, myeloma-associatedamyloid, localized amyloid (laryngeal), secondary amyloidosis, familial amyloidosis, senile amyloidosis, and dialysis-associated amyloidosis (8, 9). In a large review, 70% of the cases were primary, 19% were localized, 4% were familial, and 3% were secondary (7).
About 19% of the cases involved the head and neck, and the larynx is the most commonly affected area, although amyloid has been reported in virtually all head and neck sites (10, 11). To our knowledge, only two case reports have described the simultaneous involvement of the larynx and the sinonasal cavities (12, 13).
Although the otolaryngology literature has described amyloidosis in detail, little has been mentioned regarding its imaging appearance in the radiology literature. Calcification has been mentioned as a nonspecific CT finding (6). In the paranasal sinuses, however, this case had a “fluffy” appearance in the sinonasal cavity bones adjacent to the amyloid deposits. It is possible that the deposition of the proteinaceous amyloid fibrils in the submucosal layers of the sinonasal cavities incited an osteoblastic reaction that resulted in the “fluffy” bone changes noted. Although sinonasal calcifications can also be seen in inspissated secretions, fungal mycetomas, cartilaginous tumors, and olfactory neuroblastomas, the “fluffy” bone changes have not been seen with these diseases.
The MR findings of a prolonged T2 relaxation time and signal intensity characteristics similar to those of skeletal muscle on T1-weighted and T2-weighted images have been described in the radiology literature (6). This is not surprising in light of the fact that that the highly organized ∃-pleated sheet ultrastructure of amyloid is similar to the multilayered, myofibrillar ultrastructure of skeletal muscle (14).
Although the amyloid itself does not enhance with contrast material administration, peripheral enhancement in the region of the amyloid deposits has been noted. This may be caused by the foreign-body giant-cell reaction that is evoked about the amyloid deposits (15). The lack of enhancement of the amyloid deposits helps to distinguish them from cellular tumors, all of which enhance to varying degrees. As mentioned above, CT findings of desiccated secretions and fungal mycetomas can be seen as hyperattenuated foci, and MR may disclose low T2-weighted signal intensity or signal intensity voids. However, these inflammatory diseases do not cause the “fluffy” bone changes in the adjacent sinonasal walls noted in the case of amyloidosis.
In the larynx, the amyloid deposits are submucosal and homogeneous and are not associated with the cartilage changes. They are firm lesions that tend to occur in the supraglottic larynx, although all laryngeal sites may be affected (7). The differential diagnosis includes other submucosal diseases such as laryngeal sarcoidosis, lymphoma, and pseudotumor. Submucosal lesions such as paragangliomas and hemangiomas are more localized on CT scans and MR images, and the entire lesion enhances.
Although the final diagnosis of a mass requires that the pathologist be the final arbiter, in this patient the “fluffy” bone appearance in the paranasal sinus walls occurring concurrently in a patient with a submucosal supraglottic mass may suggest the diagnosis of this rare disorder.
References
- Received April 10, 2003.
- Accepted after revision June 30, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.