
Abstract
BACKGROUND AND PURPOSE: Postcontrast fluid-attenuated inversion recovery (FLAIR) imaging effectively depicts parenchymal and leptomeningeal metastases, as reported in limited patient groups. We compared postcontrast T1-weighted (T1W) and FLAIR imaging in a larger group.
METHODS: Sixty-nine patients with known malignancy and suspected cranial metastases underwent axial FLAIR and spin-echo T1W imaging with and then without intravenous gadopentetate dimeglumine. Postcontrast images were compared for lesion conspicuity and enhancement, number of parenchymal metastases, and extension of leptomeningeal-cisternal metastases.
RESULTS: Parenchymal metastases were demonstrated in 33 patients. Compared with T1W images, postcontrast FLAIR images showed more metastases in five patients, an equal number in 20, and fewer lesions in eight. Regarding lesion conspicuity, postcontrast FLAIR imaging was superior in five patients, equal in one, and inferior in 27. For enhancement, FLAIR imaging was superior in five, equal in five, and inferior in 23. Superior FLAIR results for lesion number, conspicuity, and enhancement were observed in the same five patients; in these patients, FLAIR imaging was performed as the second postcontrast sequence. Eleven patients had leptomeningeal-cisternal metastases; lesion conspicuity, extension, and enhancement were superior on postcontrast FLAIR images in eight. In five of eight patients, FLAIR imaging was performed as the second postcontrast sequence. Four patients had cranial-nerve metastases; in three, postcontrast FLAIR imaging was superior for lesion conspicuity and extension. In two of these patients, FLAIR imaging was the second postcontrast sequence.
CONCLUSION: Postcontrast FLAIR imaging is a valuable adjunct to postcontrast T1W imaging. Precontrast and postcontrast FLAIR imaging effectively delineates parenchymal metastases, particularly leptomeningeal-cisternal and cranial-nerve metastases.
The fluid-attenuated inversion recovery (FLAIR) technique is an inversion recovery pulse sequence with an inversion time that effectively nulls signals from the CSF at long-TE T2-weighted (T2W) imaging. The mild T1 effect of the FLAIR sequence is responsible for contrast enhancement on these heavily T2W images (1). FLAIR imaging of the brain is sensitive for detecting parenchymal lesions and is also promising in detecting extra-axial diseases such as subarachnoid hemorrhage, meningoencephalitis, and leptomeningeal metastases (2–14). In recent studies of limited patients, postcontrast FLAIR imaging was effective in the diagnosis of parenchymal tumors and leptomeningeal diseases (1, 9, 15–18). Our purpose was to compare postcontrast T1-weighted (T1W) and FLAIR images in depicting intracranial metastases in a larger patient group.
Methods
Sixty-nine patients (33 women, 36 men; mean age, 51 years; age range, 5–77 years) with a known primary malignancy and clinically suspected cranial metastases underwent MR imaging at 1.0 T. The distribution of the primary neoplasms was as follows: lung carcinoma in 31 patients, breast carcinoma in 15, both lung and breast carcinomas in one, stomach cancer in five, lymphoma in four, urinary bladder cancer in three, renal cell carcinoma in two, glioblastoma multiforme in two, colon cancer in one, pancreatic cancer in one, ovarian cancer in one, nasopharyngeal carcinoma in one, malignant schwannoma in one, and malignant melanoma in one. Institutional board approval and informed consent was obtained from each patient before their examination.
Following the acquisition of sagittal scout T1W images, axial T2W FLAIR and spin-echo T1W images were obtained before and after the intravenous administration of gadopentetate dimeglumine (GD) 0.1 mmol/kg over 1 minute. T1W (TR/TE/NEX = 380–460/8–17/3) and FLAIR (TR/TEeff/TI/NEX = 8002/149–192/2000/1) images were alternately obtained as the first contrast-enhanced images. The acquisition time was 2 minutes 50 seconds to 6 minutes 50 seconds for T1W sequences, and 2 minutes 40 seconds to 3 minutes 10 seconds for FLAIR sequences. All images were acquired with a section thickness of 5 mm, an intersection gap of 2 mm, a field of view of 18 × 18–22 × 22 cm, and a matrix of 256 × 192.
The images were transferred to a workstation and reviewed by three experienced radiologists at one sitting. Each radiologist independently evaluated precontrast and postcontrast FLAIR and T1W imaging side by side at the same time. In cases of disagreement, the final judgement was reached by consensus of the three reviewers. Parenchymal and leptomeningeal-cisternal metastases were assessed for lesion conspicuity and degree of contrast enhancement. In addition, the number of parenchymal metastases and the extent of the leptomeningeal-cisternal metastases were assessed.
Results
MR examinations revealed parenchymal metastases in 33 of 69 patients. Ten patients had solitary metastasis, while two patients had two parenchymal metastases, two patients had three lesions, and 19 patients had more than three. Four patients had associated cranial-nerve (CN) metastases, while five patients had associated leptomeningeal-cisternal metastases. Six patients had only leptomeningeal-cisternal metastases. Table 1 shows the distribution of cranial metastases.
Distribution of intracranial metastases
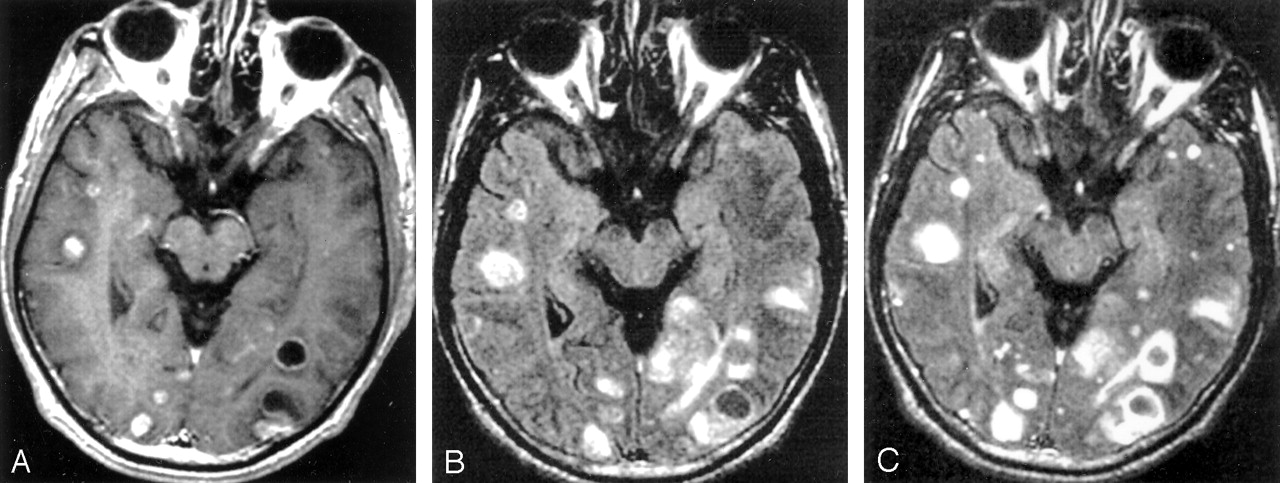
In the evaluation of parenchymal metastases, postcontrast FLAIR images demonstrated more parenchymal metastases in five patients than did T1W images, whereas they showed an equal number in 20 patients and fewer lesions in eight (Fig 1). When we compared the conspicuity of parenchymal metastases, contrast-enhanced FLAIR imaging was superior to contrast-enhanced T1W imaging in five of 33 patients, equal in one, and inferior in 27 (Fig 1). Similarly, the degree of contrast enhancement was superior with the postcontrast FLAIR sequence in five patients, equal in five, and inferior in 23 (Fig 1). In our evaluation of the number, conspicuity, and enhancement of parenchymal metastases, the postcontrast FLAIR sequence was superior to the postcontrast T1W sequence in the same five patients. In all of these patients, FLAIR imaging was obtained as the second contrast-enhanced sequence. Table 2 summarizes results from the evaluation of parenchymal metastases.

Images obtained in a 57-year-old-man with small-cell lung cancer reveal multiple, enhancing, solid and cystic parenchymal metastases. The number, conspicuity, and contrast enhancement are superior on the postcontrast FLAIR image compared with the postcontrast T1W image. In this patient, FLAIR was performed as the second postcontrast sequence.
A, Contrast-enhanced T1W image.
B, Nonenhanced FLAIR image.
C, Contrast-enhanced FLAIR image.
Evaluation of parenchymal metastases on contrast-enhanced images
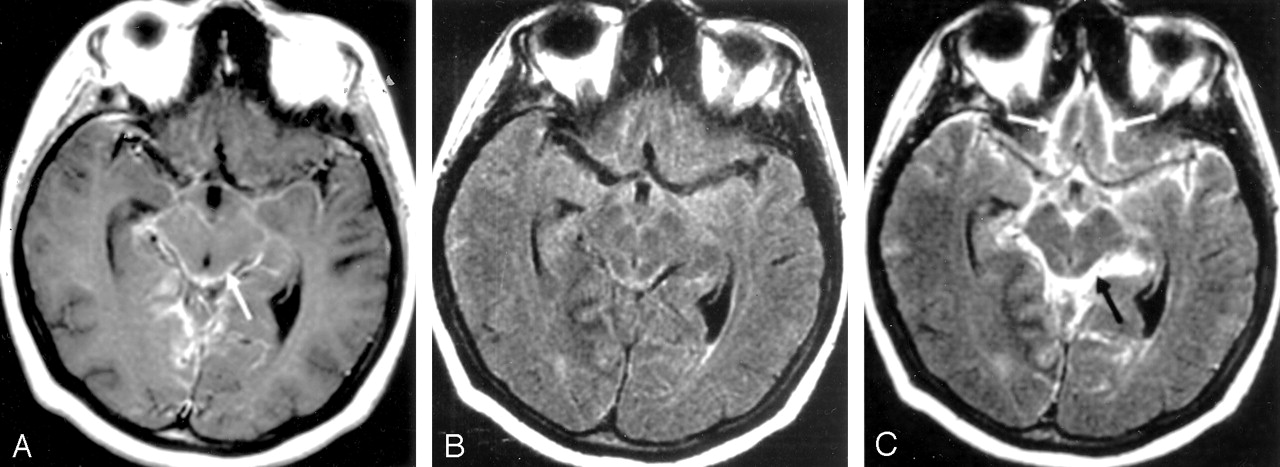
Leptomeningeal-cisternal metastases were found in 11 patients. Five of these patients also had positive CSF cytologic results. In eight patients, postcontrast FLAIR imaging surpassed postcontrast T1W imaging in terms of lesion conspicuity, extension, and degree of enhancement (Fig 2). FLAIR images were acquired as the second postcontrast sequence in five of these eight patients. Table 3 summarizes results from the evaluation of leptomeningeal-cisternal metastases.

Images obtained in a 45-year-old-woman with breast cancer. The conspicuity, extension, and contrast enhancement of the lesions are superior on the postcontrast FLAIR image (C) than on the postcontrast T1W image (A). The leptomeningeal enhancement of frontal lobes (white arrow) is not conspicuous in A as compared with C. For this patient, T1W imaging was performed as the second postcontrast sequence.
A, Contrast-enhanced T1W image shows abnormal enhancement in the basal cisterns (arrow) and leptomeninges consistent with metastases.
B, Nonenhanced FLAIR image.
C, Contrast-enhanced FLAIR image also shows the abnormal enhancement of the leptomeninges (white arrow) and basal cisterns (black arrow).
Evaluation of leptomeningeal-cisternal metastases on contrast-enhanced images
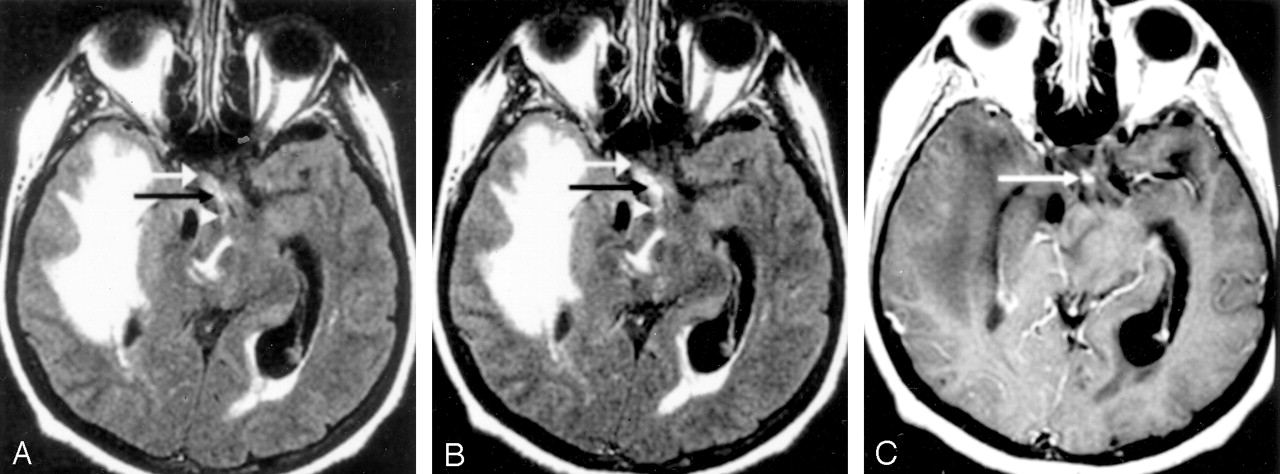
Four patients had CN metastases. In one patient, FLAIR images revealed involvement of the prechiasmal portion of the right optic nerve and extension to the optic chiasm and right optic tract. These findings were depicted as abnormal hyperintensity (Fig 3A) and marked contrast enhancement (Fig 3B) on precontrast and postcontrast FLAIR images, respectively. Only optic chiasmatic involvement was detected on the postcontrast T1W image, with no abnormal enhancement of the right optic nerve or right optic tract (Fig 3C). In another patient with involvement of the right optic tract, the metastasis was detected on precontrast and postcontrast FLAIR images (as abnormal hyperintensity) but not on the postcontrast T1W image. In a third patient with involvement of both the optic chiasm and left optic tract, the lesions were again detected on only precontrast and postcontrast FLAIR images, appearing as abnormal hyperintensity. In the patient with bilateral metastases of CNs VII and VIII, postcontrast T1W and FLAIR images were equal in the evaluation of lesion conspicuity, extension, and degree of contrast enhancement. Table 4 summarizes the results from evaluation of the CN metastases.

Images obtained in a 54-year-old-man with small-cell lung cancer. In this patient, FLAIR imaging was the second postcontrast sequence.
A and B, Nonenhanced (A) and contrast-enhanced (B) FLAIR images show involvement of the prechiasmal portion of the right optic nerve (white arrow) and extension to the optic chiasm (black arrow) and right optic tract (arrowhead). These findings appear as abnormal hyperintensity in A and as abnormal contrast enhancement in B.
C, Contrast-enhanced T1W image. Although involvement of optic chiasm is shown as abnormal contrast enhancement (arrow), involvement of the right optic nerve and right optic tract could not be detected.
Evaluation of cranial nerve metastases on contrast-enhanced images
Discussion
GD is frequently used as an intravenous MR imaging contrast agent to improve lesion detection and characterization. Although gadolinium shortens both the T1 and T2 relaxation times of tissues in which it accumulates, T1 shortening is the prominent effect at common doses. For intra-axial brain lesions, the blood-brain barrier must be disrupted for GD to enter the extracellular space. For extra-axial lesions, enhancement is observed in lesions with relatively high vascularity (9).
Contrast-enhanced T1W imaging is still the criterion standard in the detection and characterization of intracranial lesions. Although FLAIR images are commonly thought of as T2W images with dark CSF (because of the mild T1 effect induced by the long inversion time), T1 shortening produced by GD can be seen as hyperintensity on FLAIR images. Thus, lesions that show enhancement on postcontrast T1W images also show enhancement on postcontrast FLAIR images (1, 19, 20). When the FLAIR sequence is performed only after the injection of contrast material, the observed hyperintensity may be due to either T2 lengthening or T1 shortening; this feature may limit the usefulness of a postcontrast FLAIR sequence alone. To overcome this difficulty, the FLAIR sequence should be performed both before and after the administration of contrast material (9).
In parenchymal metastases with long T2 relaxation times, GD enhancement of the hyperintense lesion may be difficult to see on postcontrast FLAIR images. At postcontrast T1W imaging, it is easier to detect a hyperintense lesion surrounded by a hypointense edematous area. Hence, T1W imaging is superior to contrast-enhanced FLAIR imaging for detecting parenchymal tumors (9). In our study, the conspicuity of parenchymal metastases was superior on postcontrast T1W images compared with postcontrast FLAIR images in 27 of 33 patients.
Wessbecher et al (21) studied precontrast and postcontrast long-TR (spin-echo and T2W) images with known enhancing intracranial lesions. They compared these images with postcontrast T1W images and found enhancing lesions on postcontrast long-TR images that were not depicted on postcontrast T1W images. This observation was attributed to delayed enhancement because the long-TR images were obtained after the T1W images were. The concern that delayed enhancement might effect our results led us to perform postcontrast FLAIR and T1W sequences alternately after the administration of GD. Postcontrast FLAIR images were superior to postcontrast T1W images in depicting the number, conspicuity, and enhancement of parenchymal metastases in five patients. Because FLAIR imaging was performed as the second contrast-enhanced sequence in all of these patients, the findings were attributed to the delayed enhancement.
Contrast-enhanced FLAIR images are highly effective in the detection of sulcal or meningeal infection, inflammation, and metastases (1, 9, 15, 16). Because of the suppression of CSF signal intensity, there is marked delineation of lesions, especially meningeal lesions, that abut the border of the CSF. In addition, the fact that slow-flowing blood is not usually hyperintense on postcontrast FLAIR images but frequently hyperintense on postcontrast T1W images partly accounts for the clearer distinction of enhancing meninges and enhancing cortical veins with FLAIR imaging (9). Our results support this finding. In eight of 11 patients, the conspicuity, extension, and enhancement degree of leptomeningeal-cisternal metastases were superior on contrast-enhanced FLAIR images compared with postcontrast T1W images. FLAIR was the second postcontrast sequence in five of these eight patients. Because contrast-enhanced T1W images were acquired after contrast-enhanced FLAIR images in three patients, the findings were not attributed to delayed enhancement.
In the limited number of CN metastases, contrast-enhanced FLAIR images were superior to contrast-enhanced T1W images in terms of the conspicuity, extension, and enhancement of neural metastases. Larger series with CN metastases are needed to compare these two postcontrast sequences.
Conclusion
A postcontrast FLAIR sequence is a valuable adjunct to postcontrast T1W imaging, and the routine use of FLAIR imaging before and after the administration of contrast material is particularly useful for delineating leptomeningeal-cisternal and CN metastases.
Footnotes
Presented at the 28th Congress of the European Society of Neuroradiology, Istanbul, Turkey, 2003.
References
- Received September 4, 2003.
- Accepted after revision October 30, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Compressed Sensitivity Encoding Artificial Intelligence Accelerates Brain Metastasis Imaging by Optimizing Image Quality and Reducing Scan Time
- Utility of Contrast-Enhanced T2 FLAIR for Imaging Brain Metastases Using a Half-dose High-Relaxivity Contrast Agent
- Leptomeningeal contrast enhancement and blood-CSF barrier dysfunction in aseptic meningitis