
Abstract
BACKGROUND AND PURPOSE: Multisection CT angiography is a minimally invasive technique that can provide high-resolution and high-contrast images of the arterial lumen and wall. To our knowledge, the ability of multisection CT angiography in detecting vertebral artery (VA) dissection has never been evaluated. We assessed the sensitivity and specificity of a routine, standardized, multisection CT angiographic protocol for the detection of VA dissection.
METHODS: We retrospectively reviewed multisection CT angiograms of 17 patients with VA dissection and 17 control subjects. The acquisition protocol for multisection CT angiography was 1.25-mm nominal section thickness, a table speed of 7.5 mm per rotation (9.4 mm/s), and a 0.8-second gantry rotation period. Two radiologists assessed the maximum intensity projection and axial source images. The sensitivity and specificity of this technique in depicting VA dissection were determined.
RESULTS: Conventional angiography depicted 15 normal and 19 dissected VAs (including five stenotic, seven occlusive, and seven aneurysmal dissections) in the patient group and 28 normal and six atherosclerotic VAs in the control group. Multisection CT angiography enabled successful diagnosis of all 19 dissected VAs and 48 (98%) of 49 nondissected VAs but misidentified a severe atherosclerotic lesion as an aneurysmal-type dissection. The sensitivity, specificity, accuracy, and positive and negative predictive values of multisection CT angiography in diagnosing VA dissection were 100%, 98%, 98.5%, 95%, and 100%, respectively.
CONCLUSION: Multisection CT angiography was a sensitive and accurate technique for the diagnosis of VA dissection.
Vertebral artery (VA) dissection is an increasingly recognized cause of posterior-circulation stroke in young and middle-aged adults (1, 2). Patients have a remarkably good prognosis; the arterial abnormality resolves in 63% to 88% of patients after 2–3 months (2–5). To prevent thromboembolic complications, anticoagulation with intravenous heparin followed by oral warfarin has been recommended for the first 3 months or for more than 3 months if luminal irregularities are still found on follow-up imaging study (6). Conventional angiography has long been the criterion standard for the diagnosis or follow-up of VA dissection (3). However, this technique is not without risk. A noninvasive method is, therefore, needed to detect, monitor, and follow up this condition. Previous studies have shown the usefulness of three-dimensional time-of-flight MR angiography combined with MR imaging for the detection of VA dissection (7, 8). The sensitivity and specificity are 20% and 100% for MR imaging and 60% and 98% for MR angiography (7). Single-level dynamic CT, with its high-contrast luminal enhancement, has also been suggested as a sensitive procedure to confirm intramural hematoma, but the need of direction with prior angiography limits its clinical use (9). Multisection CT angiography is a minimally invasive technique that can provide high-resolution and high-contrast images of the arterial lumen and wall. Reconstruction techniques, such as maximum intensity projection (MIP) or curved planar reformation, can further provide images mimicking conventional angiograms. To our knowledge, the ability of multisection CT angiography in detecting VA dissection has never been evaluated. The objective of this study was to assess the sensitivity and specificity of a routine, standardized multisection CT angiographic protocol for the detection of VA dissection.
Methods
Patients
Between July 2000 and April 2003, 30 patients in Chang Gung hospital were identified as having VA dissection. The diagnosis was based on a compatible clinical picture, distinctive angiographic features, a CT or MR confirmatory study, and/or normalized or improvement of the arterial abnormalities on subsequent investigations. Among them, 17 patients (11 men and six women; age range, 27–57 years; mean age, 43.00 ± 8.49 years) were included because they underwent both multisection CT and catheter angiographic studies within a 3-day period. The charts and imaging studies of these 17 patients were retrospectively reviewed. The main clinical presentations leading to imaging were headache or neck pain (n = 2), neurologic deficit (n = 2), altered mentality (n = 1), and neurologic deficit with headache or neck pain (n = 12). Two patients had a history of trivial trauma or massage. Two patients had angiographic evidence of vertebrobasilar dolichoectasia. One patient had angiographic evidence of fibromuscular dysplasia. The duration between the onset of symptoms and initial angiography was 1–31 days (mean, 9.4 ± 7.9 days). Sixteen patients received medical treatment, and one underwent an endovascular procedure to obliterate the dissected aneurysm. After treatment, 11 patients underwent follow-up imaging 3–6 months after the onset of symptoms (10 with CT angiography and one with MR angiography). In eight, images showed normalization or improvement of the abnormalities, and images in three showed an unchanged appearance.
From a database of 266 symptomatic stroke patients with both conventional angiography and CT angiography examinations between July 2000 and February 2003, 17 subjects (11 men and six women, age range 26–56 years, mean 42.94 ± 8.74 years) were chosen as age- and sex-matched control subjects. Their main clinical presentations leading to imaging were neurologic deficit (n = 13) and transient ischemic stroke (n = 4).
Techniques
Digital subtraction angiography (DSA) was performed via the femoral artery. All images were acquired on an Integris V3000 (Philips Medical Systems, Best, the Netherlands) or an Infinix (Toshiba Medical Systems, Tokyo, Japan) imaging system. Arch aortograms were obtained, followed by selective catheterization of the common carotid arteries and the VAs. At minimum, frontal and lateral views were obtained. In our institution, several neuroradiologists review the catheter angiograms. For this study, one senior neuroradiologist (C.-J.C.) who knew the clinical information but who was blinded to the CT angiographic results retrospectively reviewed the DSA images. In evaluating the VAs, differentiating a dissected VA from an atherosclerotic VA is important. In this study, atherosclerosis of the VAs was diagnosed if luminal irregularities, stenoses, or occlusions were found not only in the VAs but also in the other cervical and intracranial arteries. The neuroradiologist classified the dissected VAs as follows: 1) stenotic type, which was irregular, scalloped, stringlike, or smooth stenosis of the VA extending a variable distance; 2) occlusive type, which gradually tapered or abruptly occluded the VA; and 3) aneurysmal type, which was pure aneurysmal dilatation of the VA or alternating narrowing and dilatation of the VA (string-of-pearls appearance). The location of dissection was classified as V1, V2, V3, or V4. V1 was the segment of the VA that passes into the neck and enters the transverse foramen of C6. V2 was the segment that ascends through the transverse foramen from C6 to C2. V3 exited the transverse foramen of C2 winds around C1 posteriorly in a tortuous manner and entered the dura at the foramen magnum. V4 began at the foramen magnum and united with the contralateral VA to form the basilar artery.
CT angiography was performed with a four-section scanner (LightSpeed, Qxi; GE Medical Systems, Milwaukee, WI). Patients were placed in the supine position after movable dental implants were removed, and they instructed to breathe quietly without swallowing during the scanning period. Helical acquisition started from the aortic arch proceeding to the circle of Willis and began 20 seconds after the start of a bolus injection of 120-mL nonionic contrast medium (Opitray 350; Mallinckrodt, St. Louis, MO) at a flow rate of 3 mL/s. A high-resolution helical protocol was performed by using a nominal section thickness of 1.25 mm, a table speed of 7.5 mm per rotation (9.4 mm/s), and a gantry rotation period of 0.8 second. The voltage of the X-ray tube was 120 kV, and the current was 280 mA. Transverse sections were reconstructed by using a modified 180° linear interpolation algorithm that incorporated views based on a balance between section profile broadening, helical artifact, and image noise. Sections were reconstructed at 0.8-mm intervals. Two trained radiologists (Y.-C.T., H.-L.H.) who were blinded to the results of conventional angiography and the patient’s clinical information independently reformatted and analyzed the CT images. Disagreements were resolved by consensus. The source axial CT images were processed into thin-slab MIPs by using a workstation (Advantage Windows 4.0; GE Medical Systems). Four MIP groups focusing on each V1-V4 segment and paralleling their long axis were reconstructed. The time for each case was around 10 minutes. MIP images were viewed first to get a general idea of the VAs. Axial source images were subsequently evaluated to confirm the findings on MIP images or to explore new findings missed on MIP images. Multiple window widths and levels were adjusted to allow clear delineation of the enhanced lumen, intramural hematoma, and calcification. Cases were discarded if the motion or dental artifacts interfered with image reading. The criteria for diagnosing VA dissection at CT angiography were as follows: 1) a narrowed centric or eccentric lumen surrounded by crescent-shaped, mural thickening and an associated increase in external diameter; 2) an abrupt or tapered occlusive lumen and an associated increase in external diameter; and 3) an aneurysmally dilated lumen or an alternatively dilated and narrowed lumen with or without crescent-shaped mural thickening or an intimal flap. Increased external diameter was evaluated by comparing it with the segment proximal to the dissection. The radiologists also classified the type and location of VA dissection according to the criteria just described. Increased external diameter, crescent-shaped mural thickening, and intimal flap were also recorded. At CT angiography, atherosclerosis of the VAs was considered present if luminal irregularities, stenoses, or occlusion were found with attenuated wall calcification, multiple-level involvement, or a normal external diameter.
Statistical Analysis
Interobserver agreement for the detection, classification, and localization of VA dissections was evaluated and expressed by using κ statistics. Agreement was excellent when κ was greater than 0.80, good when κ was 0.80–0.61, moderate when κ was 0.60–0.41, fair when κ was 0.40–0.21, and poor when κ value was less than 0.20. The sensitivity, specificity, accuracy, and positive and negative predictive values of multisection CT angiography in detecting VA dissection were calculated.
Results
Catheter Angiography
In the patient group, conventional angiography depicted 15 normal (nine right, six left) and 19 dissected (eight right, 11 left) VAs. Two patients had bilateral involvement. Among the 19 dissected VAs, five (26%) were classified as stenotic dissection; seven (37%), as occlusive dissection (including six tapered and one abrupt); and seven (37%), as aneurysmal dissection (including five with a purely dilated lumen and two with alternating luminal narrowing and dilatation) (Figs 1–3). Twelve (63%) of 19 dissections were at the V4 segment; three (16%), at the V3–4 segment; three (16%), at the V3 segment; and one, (5%) at the V1–2 segment. In the control group, conventional angiography depicted 28 normal (15 right,13 left) and six atherosclerotic (two right, four left) VAs. Among the six atherosclerotic VAs, five had a mildly irregular lumen, and one had obviously alternating regions of luminal dilatation and narrowing (Fig 4). All had associated atherosclerotic changes at the other cervical and intracranial arteries.

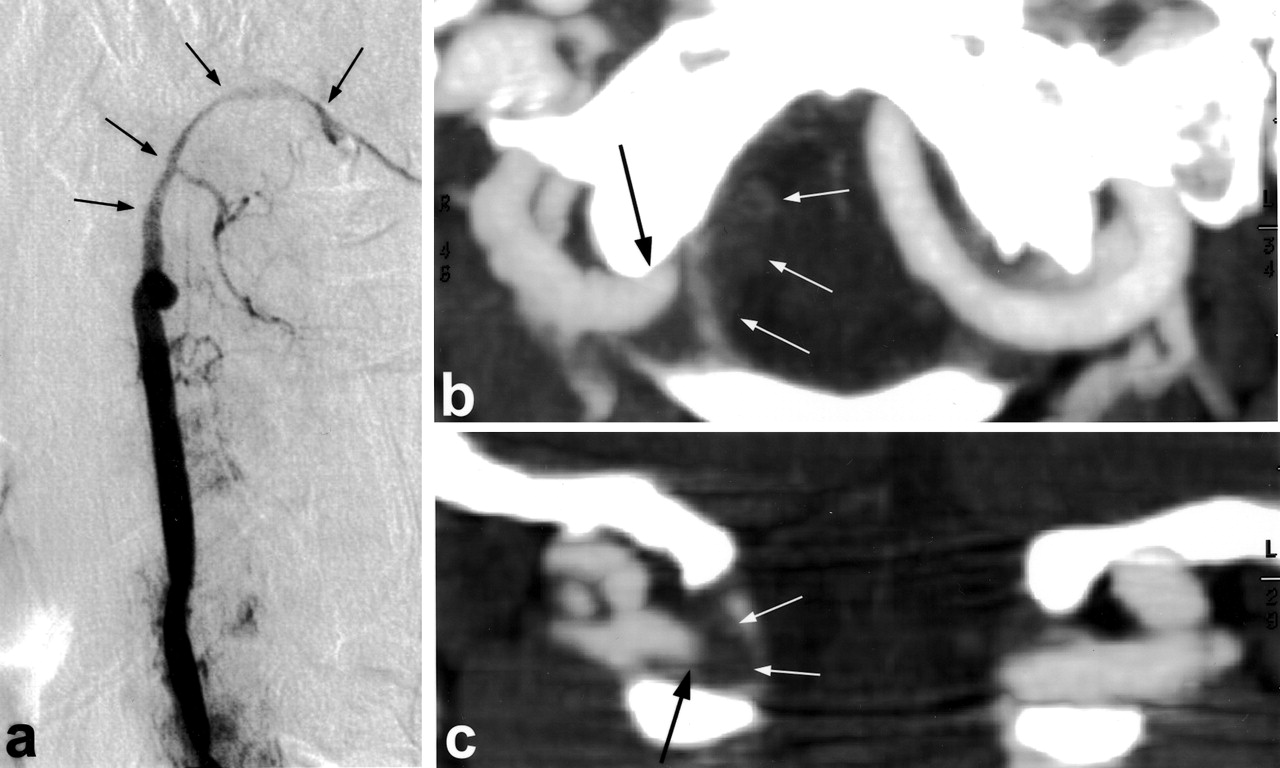
Images obtained in a 53-year-old woman with a sudden onset of occipital pain and unsteady gait. a, Conventional angiogram of the left VA in an oblique projection shows alternating regions of luminal narrowing and dilatation at the V4 segment (arrows). b and c, Axial source CT angiograms show a target appearance (narrowed eccentric lumen surrounded by crescent-shaped mural thickening and an enhanced wall) at the bilateral intracranial VAs (arrows). An associated increased external diameter of the dissected artery is noted. d, MIP CT angiogram demonstrates the same picture of an alternatively narrowed and dilated lumen (black arrows) and the intramural hematoma (white arrows)

Images obtained in a 57-year-old man with a sudden onset of severe headache and neck stiffness. a, Conventional angiogram of the right VA in a lateral projection shows a dissection aneurysm at the V4 segment (arrow). b and c, MIP CT angiograms more clearly demonstrate the multiple faces of this dissection aneurysm (arrow). d and e, Axial source CT angiograms at the level of the aneurysm and its upper part show no evidence of intramural hematoma (arrow).

Images obtained in a 51-year-old man with a sudden onset of vertigo, nausea, vomiting, and subsequent loss of consciousness. a, Conventional angiogram of the right VA shows a smoothly tapered occlusion of the VA starting from the proximal V3 segment (arrows). b and c, MIP CT angiograms show the dissection is actually starting from the junction of V3 and V4 (black arrow) with an abrupt occlusion. The faint shadow of intramural hematoma is noted at the junction of V4 and V3-V4 junction (white arrows).

Images obtained in a 49-year-old man with numbness of the left hand and dizziness for several days. a, Conventional angiogram of the right VA shows luminal irregularities at the intracranial verebrobasilar artery, especially the V4 segment, where alternating regions of narrowing and dilatation are noted (arrows). Luminal irregularities and occlusion were seen at the carotid systems (not shown). This is a case of atherosclerotic vascular disease. b, MIP CT angiogram shows the similar appearance of an alternatively dilated and narrowed lumen (arrows) at the V4 segment. c and d, Axial source CT angiograms at the levels of dilatation and narrowing show no evidence of mural thickening (arrow).
Multisection CT Angiography
All CT angiograms allowed us to read the VAs without interference from artifacts. Multisection CT angiography enabled the correct identification of all 19 dissected VAs and 48 (98%) of 49 nondissected VAs. One VA with atherosclerosis was misinterpreted as an aneurysmal-type dissection at CT angiography because of the appearance of alternating regions of luminal dilatation and narrowing (Fig 4). The sensitivity, specificity, accuracy, and positive and negative predictive values of multisection CT angiography in diagnosing VA dissection are shown in the Table.
Results of multisection CT angiography in diagnosing VA dissection
With respect to classifying dissection, CT angiography showed 89% (17 of 19) agreement with conventional angiography. Two findings were mismatched: One was a stenotic dissection that was misinterpreted as a tapered occlusion because of poor visualization of the threadlike remaining lumen on CT images. The other was a tapered occlusion that was interpreted as an abrupt occlusion because of different times in the administration of contrast medium and because of the vascular opacification between conventional angiography and CT angiography (Fig 3).
With regard to the localization of dissection, CT angiography showed 95% (18 of 19) correlation with conventional angiography. One dissection interpreted as V3-V4 tapered occlusion at conventional angiography was classified as a V4 abrupt occlusion at CT angiography (Fig 3). κ values for interobserver agreement for the detection, classification, and localization of VA dissection were 0.910, 0.937, and 0.816, respectively.
On CT angiograms, all 19 dissected VA had an increased external diameter, as compared with only 1 (2%) of 49 nondissected VAs. Fifteen (79%) of 19 dissected VAs showed crescent-shaped mural thickening, as compared with none of the nondissected VAs. None of the dissected or nondissected VAs had an intimal flap.
Discussion
When a tear occurs in a VA and allows blood to enter the wall, the extravasated blood can dissect through the media, under the intima, resulting in luminal narrowing or occlusion. Alternatively, in a subadventitial plane, this results in aneurysmal expansion of the arterial lumen beyond its normal confines (10, 11). Some have reported that aneurysmal expansion of the VA usually occurs in the V4 segment because this segment has a thicker internal elastic lamina but no external elastic lamina, a thinner adventitia, and fewer elastic fibers in the media (3, 12). Extracranial VA dissections, however, usually involve the V3 segment because this segment is movable and more exposed to minor trauma (13). Our finding that 100% (seven of seven) of aneurysmal-type dissections occurred at the V4 segment and 86% (six of seven) of extracranial VA dissections occurred at the V3 segment is compatible with those of previous reports.
Findings at conventional angiography are helpful but not always diagnostic of VA dissection. When specific radiographic signs such as pseudoaneurysm, intimal flap, or a double-lumen appearance are found, the diagnosis is usually confirmed. However, these features are infrequent, seen in less than 10% of VA dissections (11). More often, irregular stenoses or occlusions are found; these are less specific for VA dissection and may be observed in arteries with atherosclerosis or partially recanalized embolic occlusion. Therefore, the diagnosis may be suspected unless the angiographic findings are interpreted in conjunction with the clinical presentation or follow-up studies. With the advance of CT and MR techniques, CT and MR angiography are gradually replacing conventional angiography in the diagnosis of arterial dissection because they can show the intramural hematoma itself, which is especially important in the diagnosis of dissection with subtle luminal abnormalities or nonspecific occlusion. The excellent ability of CT angiography in depicting extracranial internal carotid artery dissection has been reported (with a sensitivity and specificity of 100%) (14). In the current study, we found that CT angiography is also excellent in detecting VA dissection, with a sensitivity of 100% and a specificity of 98%.
As described in reports on carotid dissection (14), an increased external diameter and crescent-shaped mural thickening were the best criteria for diagnosing dissection by use of CT angiography findings. In our series, 19 (100%) of 19 dissected VAs had an increased external diameter, and 15 (79%) had crescent-shaped mural thickening. These criteria, however, should be applied with caution. Both signs can also be found in nondissected VAs: 2% (one of 49) in our series and 7% (three of 44) in the series reported by Leclerc et al (14).
CT angiography is expected to depict more lumens that are opacified than that by conventional angiography because two-dimensional CT images allow the detection of slight difference in contrast, and the contrast material is administered over a relatively long time (15). Our results are consistent with this opinion, and this is why we saw disagreement between conventional and CT angiographic results in classifying a tapered occlusion versus an abrupt occlusion. With regard to delineating the tiny remaining lumen, however, multisection CT angiography seems inferior to conventional angiography. One stenotic dissection was misinterpreted as a tapered occlusion because of poor visualization of the threadlike remaining lumen on CT images. The reason is uncertain. It might have been due to different injection pressures between conventional angiography (direct arterial injection) and CT angiography (venous injection). Some, however, may argue that disease progression between the two studies might have been the cause, because conventional angiography was performed 1–3 days before CT angiography in this study.
Previous groups have suggested problems with MR imaging and MR angiography in diagnosing VA dissection. These include the confusing high signal intensity caused by the venous plexus or fat surrounding the VAs, the isointensity of an intramural hematoma in the acute phase, and the low resolution to visualize the relatively small VAs (16, 17). In this regard, CT angiography is superior to MR imaging because of its higher spatial resolution and the absence of flow-related artifacts. Nevertheless, MR imaging is better than CT angiography in depicting a subacute or early chronic intramural hematoma because of its conspicuous high signal intensity on T1-weighted images (14, 16). However, both techniques are still unable to completely differentiate an intramural hematoma in an occluded dissection from a mural thrombus in an occluded vessel.
In conclusion, multisection CT angiography was a sensitive and accurate technique for the diagnosis of VA dissection in this series.
Footnotes
Supported by grant NSC 89–2314-B-182A-0 (C.-J.C.) from the National Science Council and grant CMRP 1112 (C.-J.C.) from Chang Gung Memorial Hospital, Taiwan, ROC.
References
- Received August 7, 2003.
- Accepted after revision October 8, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Vertebral artery hypoplasia and vertebral artery dissection: A hospital-based cohort study
- Cervical Arterial Dissections and Association With Cervical Manipulative Therapy: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association
- High-Resolution Double Inversion Recovery Black-Blood Imaging of Cervical Artery Dissection Using 3T MR Imaging
- Added Value of High-Resolution MR Imaging in the Diagnosis of Vertebral Artery Dissection
- Dissection of the internal carotid artery causing Horner syndrome and palsy of cranial nerve XII
- Recanalization of Vertebral Artery Dissection
- Vertebral Artery Dissection with a Normal-Appearing Lumen at Multisection CT Angiography: The Importance of Identifying Wall Hematoma
- B-Flow Imaging in Low Cervical Internal Carotid Artery Dissection