
Abstract
BACKGROUND AND PURPOSE: The configurations of detachable platinum coils have evolved over the last decade. Our objective was to assess the efficacy of the anatomically conformable three-dimensional (ACT) detachable platinum microcoil in the treatment of intracranial aneurysms.
METHODS: A series of 141 patients presented between May 2000 and August 2002 to a single neurointerventionalist for endovascular treatment of intracranial aneurysms. Eight patients were treated at another institute or are now overseas. The remaining 133 patients had 141 aneurysms, which were treated; 110 were ruptured and 31 were unruptured. The clinical conditions and aneurysm locations were recorded. The procedural technique was the same as that used with the Guglielmi detachable coil (GDC) device, though the coil detachment mechanism was unique. The ACT microcoil was used in almost all cases as the initial coil.
RESULTS: Complete (100%) occlusion was achieved in 104 (74%) aneurysms. Thirty four (24%) had subtotal occlusion (≥95%), and three (2%) had incomplete occlusion (<95%). The ACT coil conformed to both spherical and irregularly shaped aneurysms. No procedure-related deaths occurred, and there was no aneurysm rupture related to coil deployment. No postprocedural rebleeding was observed.
CONCLUSION: The ACT microcoil device is feasible as an alternative platinum coil device, offering some advantages over other currently available devices.
The use of detachable platinum coils to treat intracranial aneurysms has developed rapidly since 1992, when they were first introduced into clinical practice (1, 2). The original Guglielmi detachable coil (GDC; Target Therapeutics/Boston Scientific, Natick, MA) has undergone multiple evolutions in coil range, size, and configuration to include soft or ultrasoft, two-dimensional (2D) or three-dimensional (3D), and stretch-resistant coils to improve the range of aneurysms that can be treated and to promote better aneurysm packing (3). We describe a new anatomically conformable 3D (ACT) detachable platinum microcoil (Micrus Corporation, Sunnyvale, CA) with two unique features: 1) a truly spherical, highly conformable configuration of the first coil that assists in the production of a reliable outer basket and 2) a detachment system that detaches the coil from the delivery wire within 5 seconds. We evaluated the use of this device in a consecutive series of 141 patients presenting for endovascular coil treatment of an intracranial aneurysm.
Methods
A series of 141 patients with 150 aneurysms presented to a single neurointerventionalist for endovascular aneurysm treatment. Of these patients, 133 were treated at one institution, and eight were treated at another institution or were abroad at the time of follow-up and not included. At initial neurologic evaluation, a World Federation of Neurological Surgeons (WFNS) grade was assigned (4). Both the neurosurgeon (D.N.) and the neurointerventionalist (A.J.M.) completed these examinations. The assigned grades and presentations are shown in Table 1. Patients underwent both CT scanning and digital subtraction angiography to confirm the presence of subarachnoid hemorrhage (SAH) and a cerebral aneurysm. All patients except one were treated with the Micrus 10 system. Clinical outcome measures at follow-up were collected by using the modified Rankin scale (5) (Table 2). These measures were obtained by means of clinical assessment or questionnaire (6). The angiographic outcome was obtained by assessing the appearance of the aneurysm on digital subtraction angiograms or MR angiograms, as reviewed by the treating neurointerventionalist. Occlusion was categorized on the basis of three grades of occlusion, as described in Table 3. We excluded patients with aneurysms greater than 15 mm in luminal diameter for which a 0.018-inch coil device was considered more appropriate; however, one patient was treated with the Micrus 18 system when it became available. Patients randomly selected in the International Subarachnoid Aneurysm Trial (ISAT) (7) were also excluded in the early part of the study, but subsequent approval by the ISAT steering committee allowed us to use the Micrus device in ISAT patients after February 2001.
Clinical presentations and grades
Questionnaire used to assess modified Rankin scale scores
Aneurysm angiographic outcomes
Description of the Device
The platinum coil device was available as a spherical coil (MicruSphere) for initial placement and as helical (HeliPaq), J coils (InterPaq), and ultrasoft finishing coils (UltiPaq) for packing. The coils were sized 2–10 mm in the Micrus 10 system. The spherical coil, which conforms to both spherical and irregularly shaped aneurysms, was routinely used as the first coil in almost all cases (Figs 1–3).

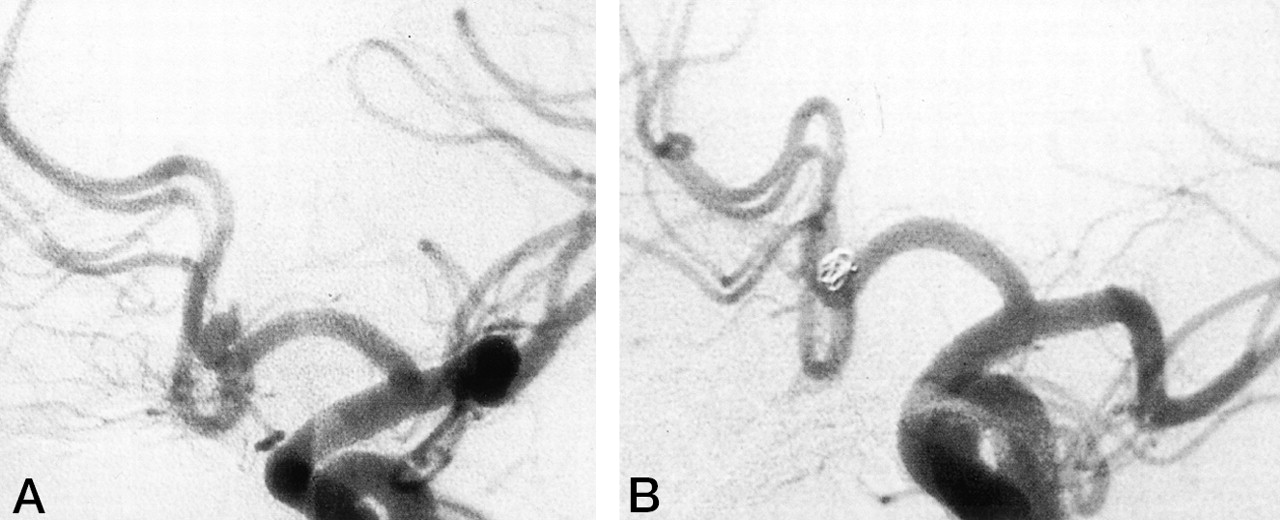
Patient 1.
A, Small, wide-necked, ruptured aneurysm of the anterior cerebral artery.
B, After treatment with a single, spherical ACT coil.

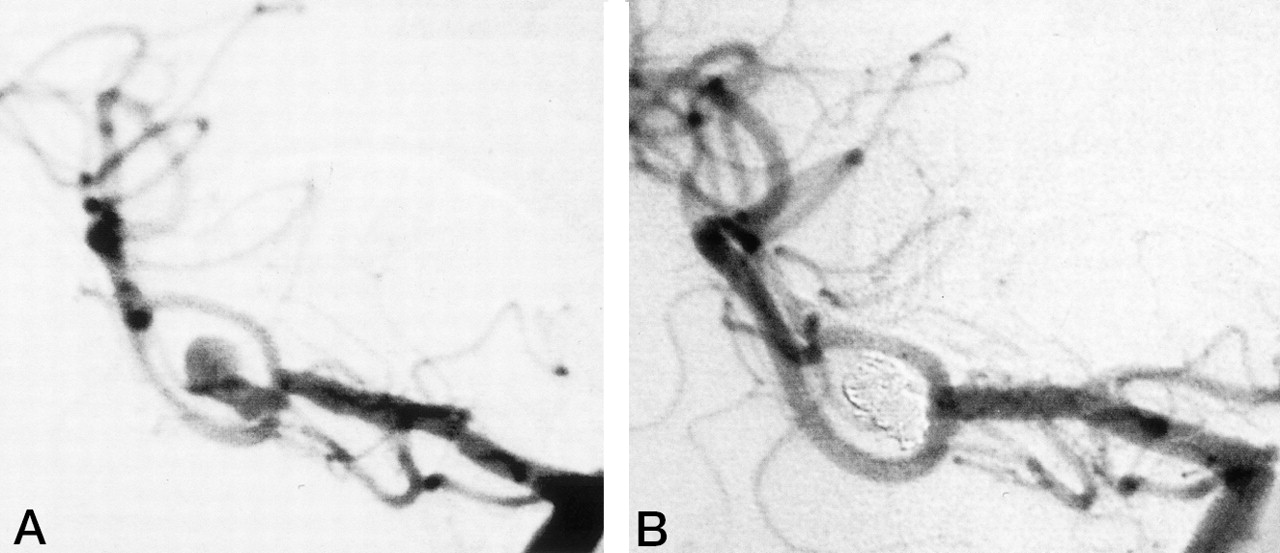
Patient 2.
A, Ruptured aneurysm of the middle cerebral artery bifurcation with a spherical dome and proximal tubular segment.
B, After treatment with a 6-mm, spherical ACT coil and four small helical coils.

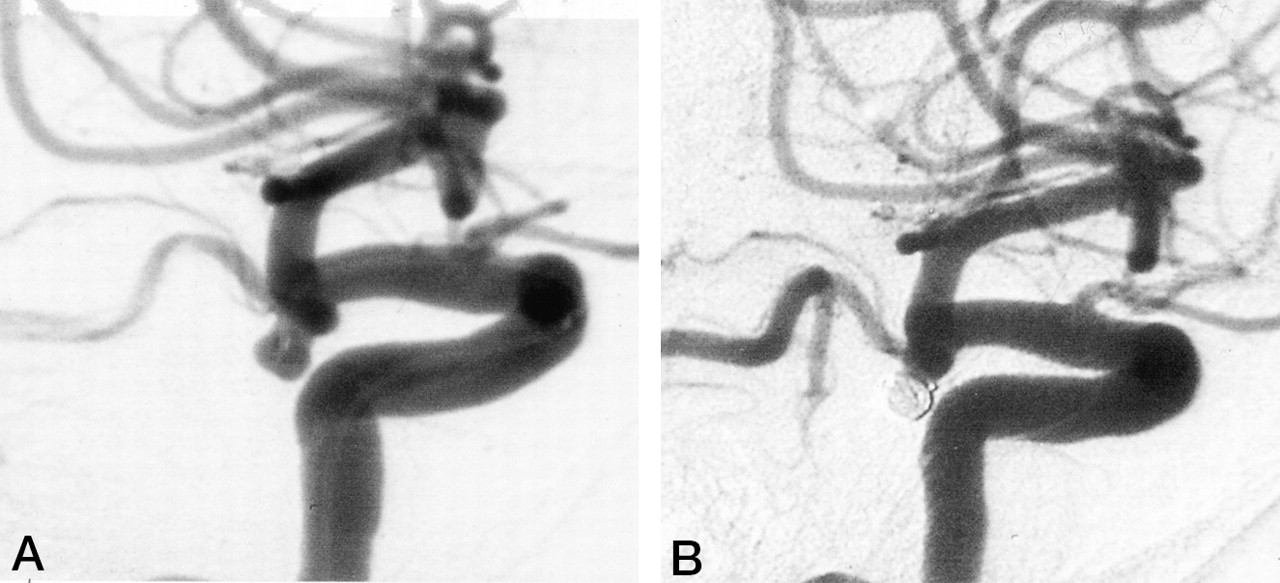
Patient 3.
A, Wide-necked, ruptured aneurysm of the posterior communicating artery.
B, After treatment with a 5-mm, spherical ACT coil as a basket followed by several small helical coils.
The coil is detached by fracturing a tensioned polyester fiber after a 5-second current cycle is applied to an insulated, resistive heating coil in the device-positioning unit. The detachment junction zone has some flexibility to allow angulation relative to the tip of the microcatheter.
Procedural Technique
The technique was the same as that used with the GDC device. The relevant cerebral vessel was catheterized with a 6F guide catheter. The aneurysm was catheterized with a 0.14-inch or 0.10-inch microcatheter, often a Rebar 14 (Microtherapeutics, Irvine, CA), a Tracker Excel 14 (Target Therapeutics/Boston Scientific, Fremont, CA), or a Prowler 14 (Cordis, Miami Lakes, FL), with appropriate stream shaping of the catheter tip. Catheter position is verified by means of angiography, and the first coil delivered under a subtraction roadmap. The balloon remodeling technique was used in 19 patients. In seven patients, a combination of Micrus ACT coils and GDC coils were used. All patients underwent anticoagulation during the procedure with systemic heparinization to maintain an activated clotting time of about twice the baseline. Heparinization continued for 24 hours after treatment. This regimen was used unless neurosurgical intervention was recently performed or planned to follow embolization.
Results
Patient age range was 25–88 years, with a mean of 54 years. Eighty-one patients were women, and 52 were men. A total of 110 patients presented with SAH; 29 of these patients had a poor clinical grade (WFNS grade of 4 or 5) at the time of the treatment. The remainder had a good clinical grade (WFNS grade of 1–3) after SAH. The locations and sizes of the aneurysms are shown in Table 4. A total of 680 coils were deployed, with a mean of 4.9 coils per aneurysm and a median of 5 coils per aneurysm. In total, 141 aneurysms were treated. The sizes ranged from 2 to 15 mm in lumin diameter.
Aneurysm location and size
Clinical Outcomes
Table 5 shows the patients’ pretreatment WFNS grades after SAH and their modified Rankin outcome at last follow-up. Outcome measures were obtained by means of clinical assessment or questionnaire (6). Follow-up was 1–29 months, with an average of 15 months. No instances of delayed rebleeding were observed during follow-up. Thirteen patients died; all had a recent SAH. Ten patients with a poor clinical grade at the time of treatment died as a result of the severity of the initial bleed. Regarding the other three patients, one had a clinical grade of 2 with severe hemispheric vasospasm, one died of liver cancer 6 months later, and one died from head trauma. No procedure-related deaths occurred, and there was no aneurysm rupture related to coil deployment. The mortality rate was 8%.
Clinical outcomes
Angiographic Outcomes
Complete angiographic occlusion (100%) was achieved in 104 (74%) aneurysms. Thirty-four (24%) had subtotal occlusion (≥95%), and three (2%) had incomplete occlusion (<95%). These occlusion categories were estimates made by the treating neurointerventionalist. Ninety-four aneurysms were evaluated after radiographic follow-up: 79 with angiography and 15 with MR angiography. Stable occlusion was shown in 88 (95%) aneurysms evaluated with follow-up imaging thus far. There have been five successful repeat treatments: three were endovascular, one involved coils, and two involved a liquid polymer (Onyx; MTI, Irvine, CA). Two patients required surgery. One patient underwent cranitomy and clipping, and one patient required revascularization and trapping of the aneurysm. Angiographic follow-up was 2–22 months, with an average of 10 months. Among the patients still due for radiographic follow-up, 35 aneurysms were pending evaluation. The results are summarized in Table 3.
Procedural Complications
One rupture due to microcatheter perforation occurred in a patient with a small, unruptured pericallosal aneurysm. The aneurysm was immediately treated with coils, and the patient had a good clinical outcome. No coil-related perforation was observed in this series, and there were no intraprocedural adverse clinical events attributable to the coil device.
One parent-artery occlusion resulted from overpacking at the anterior communicating artery, which compromised the A2 segments of the anterior cerebral artery bilaterally. However, there was adequate flow from the posterior circulation through the pericallosal collaterals, and the patient’s clinical result was given a modified Rankin score of 2 at follow-up.
One coil migrated into the distal right middle cerebral artery when a second coil displaced the first despite balloon remodeling; this occurred during the treatment of a 3-mm internal carotid artery aneurysm. An attempt to remove this coil with a snare was unsuccessful. The patient received anticoagulants for 4 days after the procedure, and antiplatelet therapy was continued for 2 months. No clinical sequelae occurred, and the artery remained open, as observed at exploratory surgery for a posterior communicating aneurysm 1 year later. There was one incidence of coil stretching and fracture; this occurred after excessive manipulation resulted in a coil length being left in the middle cerebral trunk during treatment of a right middle cerebral artery aneurysm. The patient recovered well with a modified Rankin score of 1. Complete occlusion was noted at 6-month follow-up angiography. Two patients with middle cerebral artery aneurysms had thromboembolic complications after coiling. They both developed hemiparesis and aphasia and were given abciximab (Reopro; Eli Lilly, Indianapolis, IN) in the postanesthesia recovery unit. Their deficits resolved within several hours. At follow-up, both patients’ clinical outcome was a modified Rankin score of 1. The overall procedure-related morbidity rate was 3%.
Technical Complications
In the early period (in 2000), two cases of partial detachment failure occurred. This type of failure resulted when the coil remained adherent to the device positioning unit after the detachment cycle was performed but later became detached in the microcatheter during retrieval and was redeployed by advancing the positioning unit. In one case, a loop of coil was present in the parent artery without adverse clinical sequelae. In the other case, the patient had a poor clinical grade (WFNS grade 5) after SAH and died from disease-related complications. There was one complete detachment failure with removal of the coil. Occasionally, more than one detachment cycle was required to detach the coil. With modifications to the detachment system, this problem is now uncommon.
Discussion
Occlusion of intracranial aneurysms with platinum coils has become an integral part of the management of both ruptured and unruptured aneurysms (7–11). To date, more than 100,000 patients worldwide have undergone endovascular platinum coil treatment, nearly all with the Target Therapeutics/Boston Scientific GDC device (12). The proportion of patients treated with coils varies widely in different countries. ISAT results have shown that this technique has a major role in selected patients with ruptured aneurysms, improving 1-year clinical outcome in patients with a good clinical grade with small anterior circulation aneurysms suitable for both clipping and coiling (7).
The technical challenges of small and wide-necked aneurysms have reduced the applicability of the GDC device, as reported in some centers (9, 13). The availability of a wider range of coils with extremely compliant and soft configurations have important applications, particularly in the treatment of small aneurysms. These aneurysms represented more than 90% of patients presenting for treatment after rupture, as shown in the ISAT study (7). The introduction of balloon remodeling has further increased the proportion of intracranial aneurysms that are treatable with endovascular means. This technique is particularly applicable to side-walled aneurysms and, with newer conformable balloons, to certain bifurcation aneurysms.
The newly reported treatments with liquid materials (14) are likely to be applied to larger and wide-necked aneurysms first, in which the long-term durability of coil treatment is questionable. The low rate of procedure-related complications with platinum coils in this series and other recent series may be difficult to surpass in the short term (9). Current ongoing studies will help to determine the role of liquid agents.
Patients had aneurysms covering a wide range of shapes and sizes, from small, 2-mm aneurysms to irregular aneurysms as large as 15 mm. The ACT microcoil conformed to both near-spherical and irregularly shaped aneurysms (Figs 1–3). In certain instances, more than one spherical coil was used for separate lobules, and some have advocated the use of a spherical coil within a spherical coil in a Russian doll–type situation. The ACT microcoil seemed particularly useful for small aneurysms with relatively wide necks to provide a stable first basket, either with or without balloon remodeling. Complete or subtotal angiographic occlusion was achieved in all but three patients, and no device-related adverse events occurred. Three of 680 coils (from the first production) had some type of detachment failure. Any detachment problems appear to have been largely resolved. The nature of the junction zone of the coil with the positioning unit is based on a resistive heating coil that is quite flexible and that enables its use around relatively tight bends at the aneurysm neck (eg, small lateral-wall aneurysms) without causing undue catheter displacement. The rapid detachment mechanism is helpful, especially in large aneurysms. In seven patients, both GDC and ACT coils were used because of the lack of a correct helical ACT coil size. However, the coil platinum alloys are virtually identical, and the coils can be used together without difficulty through the same range of microcatheters.
The immediate clinical outcomes were satisfactory and comparable to those of the existing GDC device. Rupture during coil deployment did not occur in any patients in this series. The numbers were too small to determine if our rupture rate differed from the 3–5% associated with GDCs (8–11). There is no reason to suppose that the overall procedural complication rate differs from that of the GDC device.
The current data suggest that endovascular coil treatment is successful in preventing early and mid-term rebleeding (8, 15). The occlusions achieved with the ACT microcoil device are encouraging, but whether the long-term results differ from those of other available coils is unclear. The ability to achieve excellent acute occlusion by using the spherical first coil may or may not improve the long-term durability of the angiographic occlusion; however, no instances of delayed rebleeding occurred in this patient population during follow-up.
Conclusions
The Micrus ACT microcoil device is a feasible alternative platinum coil system, offering advantages over the currently available GDC device. The spherical coil offers excellent conformability and stability as an outer basket for aneurysm packing, and it seems particularly effective for small and wide-necked aneurysms. The rapid detachment mechanism is helpful, especially in large aneurysms. The Micrus coil device was safe and reliable in this series.
Acknowledgments
The authors would like to thank Julia Yarnold, FCR, MA, and Joan Rischmiller, RN, of the Neurovascular Research Unit, The Radcliffe Infirmary, Oxford, United Kingdom, for their help and support and Jan Newport for her assistance.
Dr A. J. Molyneux is a medical advisor to Micrus Corporation and has stock interest in the company. Dr D. B. Niemann has received educational grant support from Micrus Corporation and its distributors.
Footnotes
Presented at the World Interventional Neuroradiology meeting Val d’Isere, 2002, and the American Association of Neurological Surgeons/Congress of Neurological Surgeons Joint Meeting American Society of Interventional and Therapeutic Neuroradiology 2002.
References
- Received May 13, 2003.
- Accepted after revision October 18, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}