
Abstract
BACKGROUND AND PURPOSE: Although CT findings of Kikuchi disease (KD), or histiocytic necrotizing lymphadenitis, are reported in several case reports, large-scale analysis of the disease has not been undertaken. We characterized the clinical and CT findings in a large group of patients with KD.
METHODS: Between 1990 and 2002, 96 patients (68 women, 28 men; mean age, 24.4 years) underwent biopsy of the cervical lymph nodes and had histologically proved KD at our institution. We reviewed their clinical and CT findings and recorded the total number of affected nodes; location and size of the lymph nodes; and characteristic findings including necrosis, perinodal infiltration, and contrast enhancement.
RESULTS: We identified 1196 affected lymph nodes (12.5 nodes per patient). The affected lymph nodes were 0.5–3.5 cm (mean, 1.62 cm). Perinodal infiltration was found in 78 patients (81.3%). Eighty (83.3%) had homogeneous nodal contrast enhancement. Nine patients (9.4%) had lymph nodes with a focal low attenuation, and seven (7.3%) had ring-shaped lymph nodes. Unilateral and bilateral cervical lymph nodes were affected in 76 and 20 patients, respectively. Lymph nodes were mainly located at levels II (IIA, 174 nodes; IIB, 254 nodes), III (222 nodes), IV (160 nodes), and V (VA 126 nodes, VB 130 nodes). Follow-up CT in 32 patients showed complete resolution in 14 and partially improved lymphadenopathy in 18.
CONCLUSION: Awareness of the various CT appearances of KD and follow-up CT may be helpful for more accurate diagnosis of the disease.
Kikuchi disease (KD), also known as Kikuchi-Fujimoto disease or histiocytic necrotizing lymphadenitis, is a self-limiting cause of cervical lymphadenopathy. First described in 1972 (1), KD is increasingly recognized in the literature; however, relatively few case reports include its radiologic findings (2–4).
This rare form of lymphadenitis preferentially affects young women, and most patients are under 30 years of age. KD is histopathologically characterized by cortical and paracortical necrosis with a lymphoreticular infiltrate and the absence of granulocytic infiltrates. Clinically, the most common presentation of this disorder is cervical lymphadenitis, although the lymphadenitis may also be generalized. Other complaints include low-grade fever, malaise, fatigue, and diarrhea. Sometimes, the condition is accompanied by weight loss, nausea, and vomiting. No specific laboratory tests are available for the diagnosis of KD, although leukopenia and atypical lymphocytes are frequently observed in the peripheral blood (5–7). Because KD is a benign and self-limiting disease, a proper diagnosis may help patients avoid unnecessary treatment.
Although CT findings have been described in several case reports, to our knowledge no large-scale analysis of radiologic findings has been conducted. Previous authors (2, 3) have reported enlarged, multiple lymph nodes that are homogeneously enhancing, without evidence of gross necrosis on CT. However, one case report (4) mentions two cases in which enlarged nodes showed atypical enhancement suggestive of macroscopic necrosis.
We reviewed the charts and histopathologic records of patients with KD who were treated at our hospital during the past 12 years. The clinical features and CT findings are discussed here.
Methods
We retrospectively reviewed the charts and histopathologic records of patients with KD diagnosed at Anam Hospital, Kuro Hospital, or Ansan Hospital, South Korea, from January 1990 to January 2002. A series of 96 patients who underwent CT of the neck and who had their diagnoses proved histologically by an excisional biopsy of a cervical lymph node. An experienced head and neck pathologist (Y.K.) reviewed all histologic specimens. Histologic confirmation was made when the lymph node showed classic morphologic features of KD and histologic variants (7, 8). These findings may vary but often meet the following criteria: 1) patchy irregular areas of eosinophilic necrosis in the paracortex and/or cortex, 2) pronounced fragments of nuclear dust distributed in an irregular fashion through the area of necrosis, 3) absence of granulocytes and paucity of plasma cells, 4) clusters of plasmacytoid T cells or plasmacytoid monocytes, and 5) numerous immunoblasts (transformed lymphocytes, predominantly of T cell phenotype).
Clinical characteristics, associated symptoms, and laboratory study results were collected from the medical records.
A typical neck CT examination (Somatom Plus S at Anam and Kuro Hospitals and Somatom Plus 4 at Ansan Hospital; Siemens Medical Systems, Erlangen, Germany) had been performed in the axial planes from the skull base to the upper mediastinum. Sections were 5-mm thick and contiguous, and images were obtained after the intravenous administration of 60–120 mill of non-ionic contrast medium (Ultravist [iopramide]; Schering, Berlin, Germany) based on the patient’s weight. An experienced radiologist (T.K.) reviewed the CT scans. A lymph node was counted as affected when it showed one of the following findings: increased size (maximum diameter compared with expected normal size for the respective region), abnormal shape (not oblong or lima bean–shaped but spherical), clusters of small lymph nodes, necrosis and perinodal infiltration, and increased contrast enhancement. (Normal nodes are less hyperattenuated than adjacent vascular structures on contrast-enhanced CT; differences between normal nodes and vascular structures are usually more than 10–20 HU.) We recorded the total number of affected lymph nodes per patient; the locations of lymph nodes according to the imaging-based nodal classification reported by Som et al (9); size (maximum diameter); and the presence of characteristic findings including necrosis, perinodal infiltration, and contrast enhancement.
Results
Patient Characteristics
The patients’ clinical characteristics are summarized in Table 1. The patients’ ages ranged from 12 to 40 years, and the male-female ratio was 1:2.43. All were natives of the Republic of Korea and had no notable history of travel outside the country. Leukopenia with a white blood cell count of less than 3900/mm3 in men and less than 3500/mm3 in women was noted in 30 patients (31.3%). None had profound leukopenia; that is, a white blood cell count of <2000/mm3. An elevated body temperature (37.5°C) was observed in 56 patients. The interval between when patients noticed symptoms and when they sought clinical help was measurable in days for 22 patients, weeks for 41 patients, and months for 33 patients. Lymphadenopathy generally resolved within 1–8 months. All patients were well, with complete resolution of the remaining lymph nodes at follow-up of 4 months to 11.2 years. Neither recurrence nor persisting KD has since been noted.
Clinical features of KD
CT Findings
CT findings are summarized in Table 2. We identified 1196 affected lymph nodes in 96 patients by means of CT. One patient had only one affected lymph node in the supraclavicular region. The remainder had multiple, affected lymph nodes (Fig 1), with a range of 4–30 lymph nodes. The maximum diameter of the affected cervical lymph nodes was 0.5–3.5 cm, and the mean maximum diameter was 1.62 cm. Perinodal infiltration was observed in 78 patients (81.3%). The appearance of perinodal infiltration differed from case to case, from mere obliteration of the adjacent fat plane to widespread increased attenuation involving nearly the entire cervical space. Eighty patients (83.3%) had homogeneous lymph nodes. Although the attenuation of lymph nodes was less intense than that of vascular structures, it was higher than that of adjacent musculatures. Nodes contained prominent areas of low attenuation, suggesting gross nodal necrosis in 16 patients (16.7%). In nine patients (9.4%), areas of low attenuation were focal and eccentric. In seven patients (7.3%), areas of low attenuation were located centrally with a thin peripheral rim and ring-shaped appearance (Fig 2).

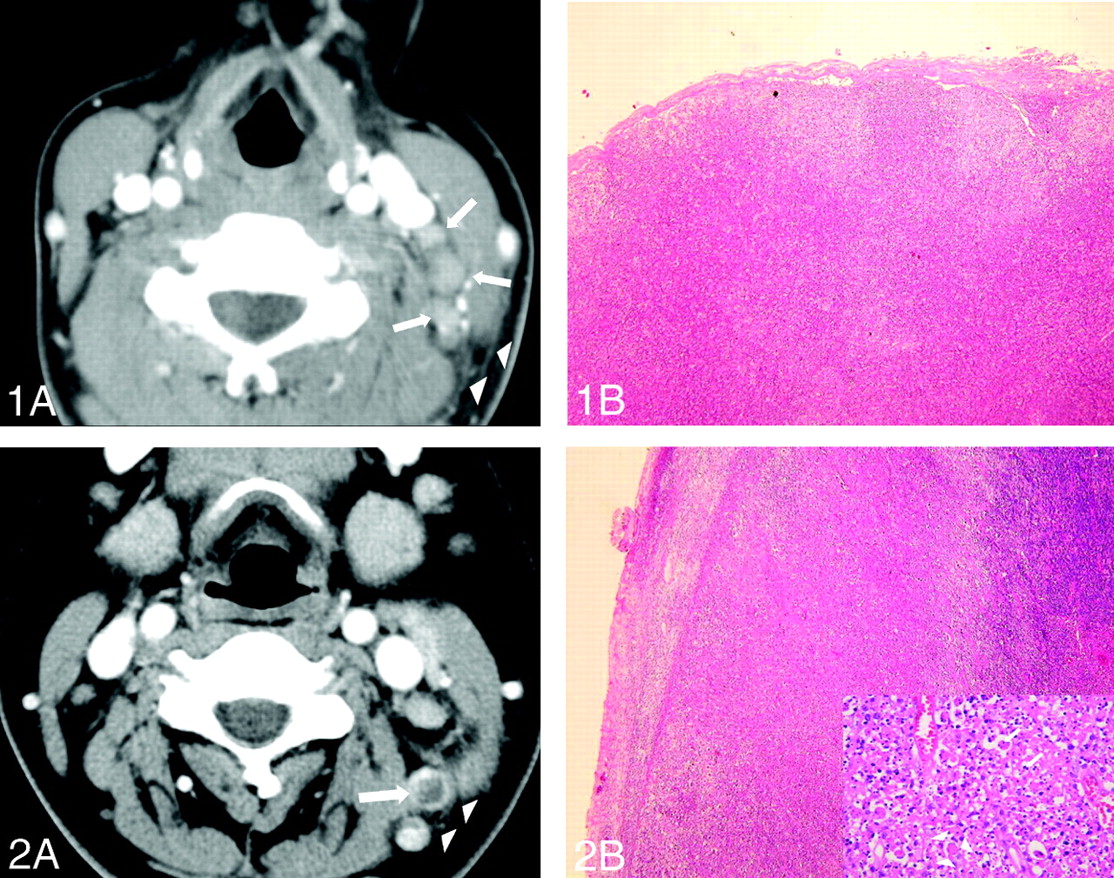
Images obtained in a 28-year-old woman presenting with a 2-week history of fever, myalgia, and tender cervical lymphadenopathy.
A, CT scan shows multiple small and medium lymph nodes (arrows) on the left side of the neck (level III). Note the obliteration of perinodal fat at levels III and V and in the adjacent superficial space (arrowheads).
B, Photomicrograph of a surgical specimen from a lymph node shows patchy areas of lymphohistiocytic infiltration that does not distort the otherwise normal lymph node architecture (hematoxylin-eosin stain, original magnification ×40).

Images obtained in a 34-year-old woman.
A, CT scan shows small lymph nodes on the left at levels IIB and V. Note the ring-shaped nodal necrosis (arrow) mimicking that of tuberculosis or metastatic lymphadenopathy. Adjacent perinodal infiltration is also seen (arrowheads).
B, Photomicrograph of surgical specimen of lymph node shows a geographic pattern of eosinophilic necrosis and sheets of histiocytes (hematoxylin-eosin stain, original magnification ×40). Inset, High-powered view of a necrotic focus shows abundant karyorrhectic debris (arrows) and crescent-shaped histiocytes (original magnification ×400).
Summary of CT findings in lymph nodes in KD
Enlargement of the lymph nodes was right-sided in 34 patients, left-sided in 42, and bilateral in 20. However, most patients with bilateral involvement had an asymmetrical distribution. The location of the 1196 lymph nodes in the 96 patients is summarized in Table 3. Most of the nodes (89.1%) were at levels II, V, III, and IV (in order of decreasing frequency). There was a small number of level I, VI, or VII and supraclavicular lymph nodes. We also had a few cases with involvement of the parotid or superficial nodes. There was no case of involvement of the retropharyngeal nodes.
Location of cervical lymph nodes in KD
Thirty-two patients (34%) underwent follow-up imaging studies with CT, sonography, or both within 1–8 months. Follow-up CT findings were complete resolution in 14 patients or a decreased number and size of lymph nodes with a decreased extent of perinodal infiltration in 18 patients.
Discussion
KD, also called Kikuchi-Fujimoto disease or histiocytic necrotizing lymphadenitis, is a rare cause of cervical lymphadenopathy. Early series noted a dramatic female predominance; however, more recent reports show only a slight female preponderance ranging from 1.1:1 to 2.75:1 (5–7). Our data showed no significant difference. Most patients in previous studies were younger than 30 years, with a mean of 25.5–30.0 years (5–7). Our patients were aged 12–40 years, with a mean of 24.4 years.
The etiology of the disease remains unclear. Various infections are postulated to be causes; these include Toxoplasma species, Yersina enterocolitica, Epstein-Barr virus, rubella, paramyxovirus, and parainfluenzavirus. Some findings indicate that interferon γ, interleukin-6, or apoptotic cell death may play a role in the pathogenesis of KD (8, 10, 11).
Negative laboratory results are important for excluding other disorders. White blood cell counts in the normal range are common, but leukopenia is frequently mentioned and consistent with KD, occurring in 25.5–58.3% of cases (12). Our data showed similar results and revealed no case of profound leukopenia. Because of the absence of a specific diagnostic tool for KD, radiographic examination is important. CT and MR imaging are the useful imaging modalities for patients with cervical lymphadenopathy, although sonography has also been used (2, 4). Although CT poses a radiation hazard, it is the preferred method to evaluate head and neck diseases because of its cost-effectiveness. It also enables an evaluation of the extent of disease and provides the opportunity to look other lesions that could explain the lymphadenopathy. MR imaging and sonography had also been performed in our patients, but the number of cases was too small to analyze statistical significance of the image findings.
In our study, common CT findings in KD included multiplicity, homogeneity, and perinodal infiltration. Several case reports have mentioned similar CT findings, but different CT features have also been reported. Generally, CT features may mimic those of lymphoma; however, lymph nodes in KD are not as large as those in lymphoma (13, 14). The sizes of the lymph nodes in our study were variable but did not exceed 3.5 cm in greatest dimension, with a mean of 1.62 cm. In addition, most of the nodes (1124 of 1196, 94.0%) were in the range of 0.5 to 2.5 cm. This corresponds well with previous reports (5, 15). Therefore, one clue to the diagnosis of KD may be the pattern of lymphadenopathy; that is, an increased number of slightly enlarged lymph nodes. Lymphoma often produces a few or many moderately to markedly enlarged lymph nodes.
Another common feature of KD is perinodal infiltration, which may be observed in other nodal diseases, including lymphoma and metastasis; however, this is more characteristic of inflammatory diseases. Histologically, structures surrounding the lymph nodes are infiltrated by an attenuating perivascular and interstitial inflammatory cell population similar to that seen in nodal-based lesions. This population includes a mixture of lymphoid cells and histiocytes and the characteristic karyorrhectic debris (7). Perinodal infiltration on CT scans has also been mentioned in previous reports (3, 4), but its incidence or histologic background has not been described.
Nodal necrosis was another interesting feature of KD in our study and one not commonly mentioned. In most cases reported to date, the homogeneity of lymph nodes mimicking lymphoma has been mentioned. Only Na et al (4) reported that contrast-enhanced CT and MR imaging revealed variable degrees of nodal necrosis in two cases of KD. Sixteen (16.7%) of our 96 patients had nodal necrosis; this finding suggests that macroscopic nodal necrosis is not an unusual feature of KD. The chief histologic features of KD are variable degrees of necrosis in cortical and paracortical areas, with prominent karyorrhectic debris, proliferation of histiocytes and immunoblasts surrounding the area of necrosis, and the absence of granulocytes (5, 6). The rarity of extensive necrosis is well known in KD; clinically and histologically, KD is often mistaken for lymphoma. However, CT scans may sometimes reveal nodal necrosis in KD, and in such cases, KD can also mimic various nodal diseases with nodal necrosis, such as metastasis and tuberculosis (16, 17).
The sites of cervical lymphadenopathy are occasionally reported. Unilateral neck involvement is dominant. Cervical lymphadenopathy is common in the posterior cervical triangle and jugular carotid chain (12). In our series, the same sites were frequently affected. Seventy-six patients (79.2%) had unilateral neck nodes, and 20 (21.8%) had bilateral cervical lymph node enlargement. Although the frequency of bilateral involvement was somewhat higher than that reported in the literature, most cases showed an asymmetric predominance. In addition, we found that levels II-V were the preferred sites of lymphadenopathy. Level II was the most frequent site, followed by level V. Along the internal jugular vein, the upper level had more affected nodes. Lymph node enlargement can develop anywhere, but we observed no case of enlargement of the retropharyngeal nodes. Sometimes, affected nodes were found in the parotid, supraclavicular fossa, and mediastinal regions. According to the literature, KD is not limited to cervical lymphadenopathy; it can also involve the abdominal lymph nodes (16). However, we focused on the cervical region, and how frequently abdominal lymphadenopathy simultaneously occurs with cervical lymphadenopathy is not known.
In most of our patients, lymphadenopathy resolved completely or improved within 1–8 months without medical treatment, as proved by follow-up imaging studies in many patients. In this way, KD is different from other nodal diseases, such as tuberculosis, lymphoma, and metastasis. Therefore, follow-up CT may be helpful in evaluating patients with unusual CT findings mimicking those of nodal diseases other than KD.
In conclusion, the common CT features of KD is unilateral, homogeneous enlargement of multiple lymph nodes affecting levels II-V. Perinodal infiltration is also frequently found on CT scans. Most of the nodes did not exceed 2.5 cm in greatest dimension. Variable CT features, including nodal necrosis, are also noted; these findings can develop anywhere in the cervical region. Follow-up CT showed complete or partial regression of lymphadenopathy within months. Awareness of the various CT appearances of KD and follow-up CT may be helpful for more accurate diagnosis of the disease.
References
- Received October 24, 2003.
- Accepted after revision December 1, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}