
Abstract
Summary: A 4-year-old boy developed progressive neck pain and an expansile osteogenic lesion of C2; the diagnosis was an aneurysmal bone cyst. An image-guided biopsy with 3D CT planning was performed followed by Ethibloc injection into the aneurysmal bone cyst. Subsequent CT and MR images demonstrated embolization material in the vertebrobasilar system, and the patient died of brain stem and cerebellar infarction 23 hours after the intervention. The course of events and technical considerations are discussed.
Aneurysmal bone cysts (ABCs) are benign bone lesions that account for approximately 1–6% of all bone tumors. They typically occur in the 2nd decade of life and most often affect the long bones. The spine is involved in only 3–20% of cases (1). In the spine, ABCs typically involve the posterior elements but are not uncommon in the vertebral body and may eventually extend to more than one vertebra, leaving the disk space intact. They tend to expand the vertebral body with cortical thinning or destruction and not infrequently cause vertebral collapse (vertebral plana). Clinically, cervical-spine ABCs present with pain, stiffness, swelling, torticollis, and reduced range of motion. Because of the rarity of this lesion, no standard therapeutic regimen exists. The recurrence rate after surgical resection or curettage is considerable.
Ethibloc (Ethnor Laboratories/Ethicon, Norderstedt, Germany) is an emulsion of zein, alcohol, oleum papaveris, propylene glycol, and a contrast medium. It thickens immediately when in contact with aqueous solution (2, 3). Its approved uses include injection of pancreatic ducts and lymphatic cystic malformations. Recently, however, it has been reported to be effective (in an off-label use of the device) in inducing fibrosis and secondary reossification of vertebral ABCs (4). We report herein an unfortunate fatality of a 4-year-old boy following percutaneous Ethibloc injection into an extensive ABC in the vertebral body and the posterior elements of C2, when the vertebrobasilar system was inadvertently embolized.
Case Report
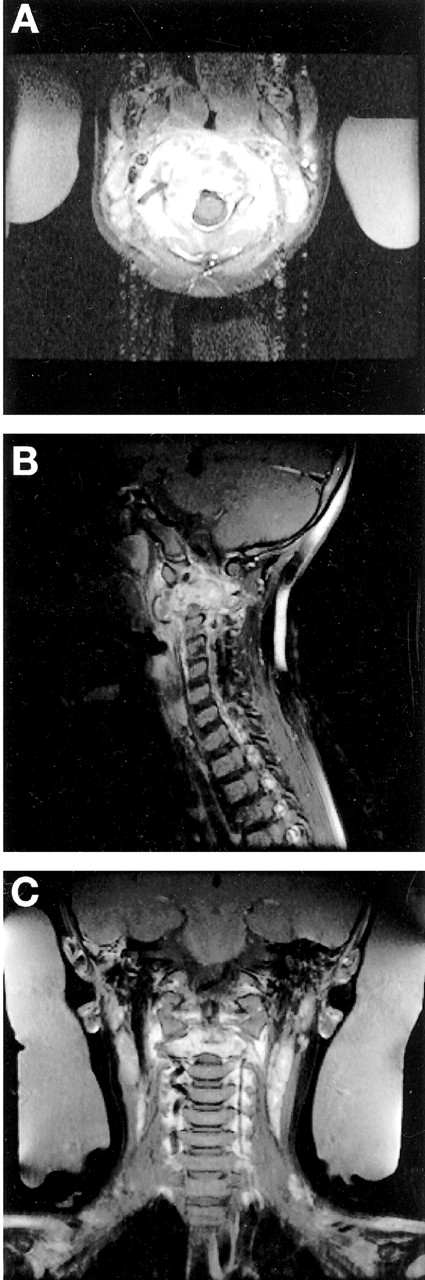
A 4-year-old boy presented with a 4-month history of rapidly increasing neck pain, to the point that he had difficulty holding his head up when first seen at this institution. He complained of dysesthesia in both arms and legs but was otherwise neurologically intact. Conventional radiography, CT, and MR imaging of the cervical spine revealed an expansile cystic lesion of the posterior elements to the right and of the vertebral body of C2 with fluid-fluid levels and slight enhancement of the internal septation (Figs 1–⇓3). The lesion surrounded the right vertebral artery and was consistent with the diagnosis of an ABC. The patient was seen in a combined complex spinal deformity clinic by an orthopedist and neurosurgeon. Because radical excision of the ABC would have required both an anterior and posterior surgical approach and fusion of the spine from the occiput to C3, with considerable risk and morbidity, the patient was referred to the interventional service. In the meantime, the patient experienced further exacerbation of neck pain.

Lateral (A) and open-mouth odontoid (B) conventional radiographs of the cervical spine show the osteodestructive lesion in C2.

Preinterventional postgadolinium T1-weighted MR images of the cervical spine in the axial (A), sagittal (B), and coronal (C) planes show an irregular, enhancing, expansile lesion in the body and the lamina of C2 surrounding the right (dominant) vertebral artery.

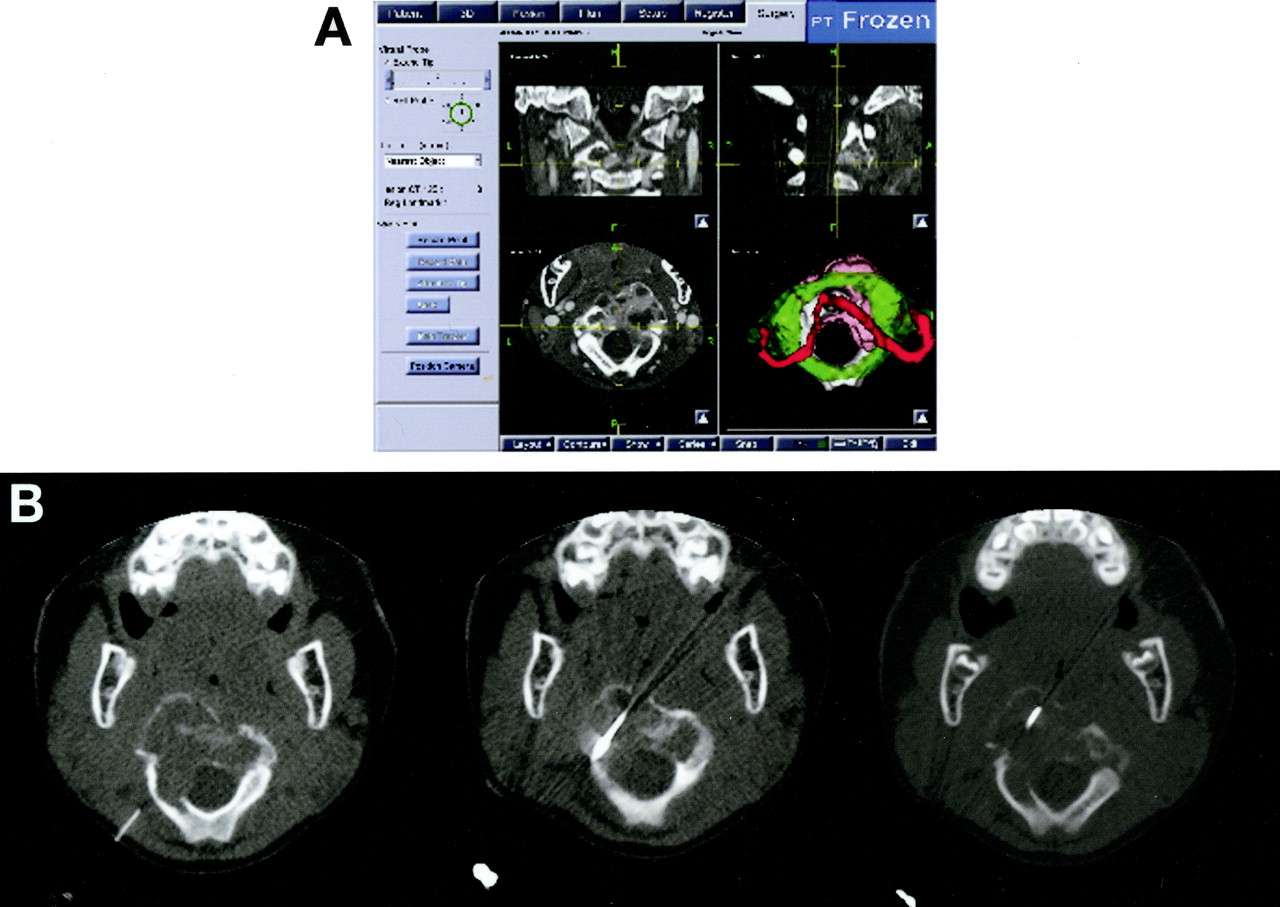
3D CT planning and reconstruction scan (A) of the upper cervical spine depicts the multicystic lesion and superimposed C1 (green) as well as the vertebral arteries (red). The trajectory of the biopsy needle can be seen in three subsequent axial CT scans (B).
It was elected to perform percutaneously a biopsy of the lesion, followed by injection of Ethibloc. Three-dimensional C2 reconstructions were created to display the vertebral artery and plan the needle trajectory (Fig 3A and B). The patient was placed under general anesthesia with spinal precautions, in the prone position. A bone trephine needle was inserted through a 2-mm skin incision 4 cm to the right of the midline and advanced at 3–4-mm increments under CT fluoroscopy guidance through the lamina of C2 into the body. Two biopsies were taken for tissue diagnosis and sent for pathologic analysis. The needle was then advanced toward the anterior limit of the cyst under CT fluoroscopy guidance. No significant bleeding occurred from the biopsy cannula at any stage. Ethibloc was injected at 0.5-mL increments up to a total volume of 2.5 mL, and repeat CT fluoroscopy images were obtained after each injection.
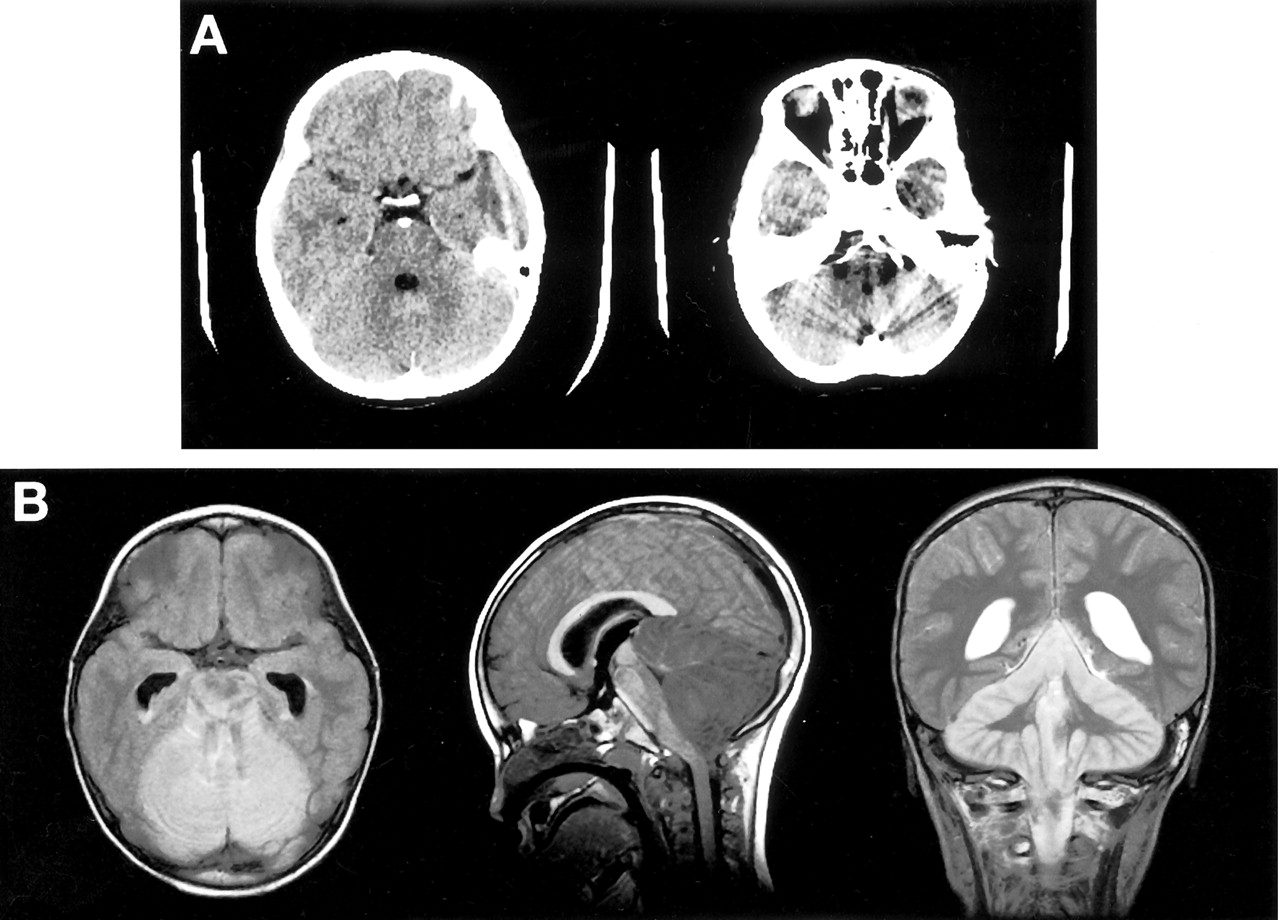
The postinterventional CT scan demonstrated that most of the ABC was filled with Ethibloc. Some epidural and paravertebral veins also showed filling. In retrospect, there was also filling of the right vertebral artery and proximal basilar artery. The patient partially emerged from anesthesia and was extubated and transferred to the recovery room but did not fully regain consciousness despite full narcotic reversal. One and a half hours later, he developed sunsetting of his eyes and sluggish pupillary reaction to light. The patient showed no response to central pain and extended all four extremities to a peripheral painful stimulus. An emergent CT scan revealed Ethibloc in the vertebrobasilar system with brain stem infarction (Fig 4A). The patient was reintubated and transferred to the intensive care unit. Interventions such as cerebral angiography, cerebral embolectomy, and cerebral bypass surgery were considered but were thought to offer no diagnostic or therapeutic benefit. The patient’s condition continued to deteriorate, and 12 hours later no brain stem reflexes were noted. An MR image showed brain stem and cerebellar infarction, ventricular dilatation, no flow in the vertebrobasilar artery system, and upward as well as downward herniation of the cerebellum (Fig 4B). An electroencephalogram was isoelectric, and the child was declared brain dead 23 hours after the intervention.

Postinterventional CT scans of the head with Ethibloc filling of the vertebrobasilar system (A), causing cerebellar and brain stem infarction. Signal intensity changes in the brain stem and the cerebellum, cerebellar swelling with brain stem compression, and up- and downward herniation are shown on axial FLAIR, sagittal T1-weighted, and coronal T2-weighted MR images (B).
At autopsy, the brain weighed 1510 g (normal for age is 1191 g). The cerebellum and the brain stem were significantly swollen with upward and downward herniation of the cerebellum. The vertebral, basilar, bilateral anterior inferior cerebellar, bilateral superior cerebellar, and bilateral posterior cerebral arteries were filled with and completely occluded by Ethibloc. The microscopic evaluation demonstrated that the ABC was largely filled with Ethibloc.
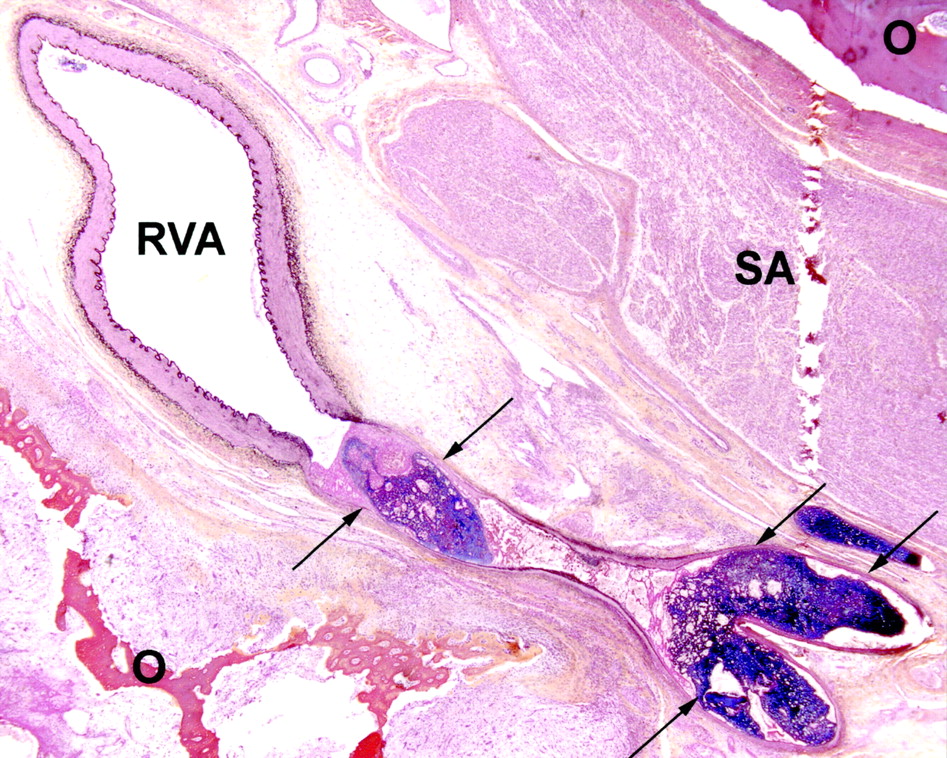
There was no injury to the vertebral artery; however, Ethibloc was seen in the lumen of a small branch artery of the vertebral artery at the C2 level with this small artery locally distended and with its wall necrotic with an adjacent acute inflammatory reaction (Fig 5). Recent thrombus was present at the orifice of the branch artery from the right vertebral artery. No direct communication between the aneurysmal bone cyst and this branch artery was evident despite serial thin (5-μm) sections of the decalcified vertebral body and a well-defined needle tract was not seen in the sections. No other side branches of the right vertebral artery were found at C2. Review of the CT images obtained at the time of the injection in relation to the landmarks of C2 indicated that the site of the injecting needle was 8 mm above the solitary side branch and 9–10 mm beyond the outer limit of the bone on the right side of C2. Thus, the needle could not have entered the right vertebral artery anywhere along its course. Although the route taken by the Ethibloc into the branch artery could not be defined, it is inferred that Ethibloc passed through the tumor into the branch artery and retrograde along the branch artery into the right vertebral artery.

Histopathologic section from autopsy shows Ethibloc (purple staining material) together with recent thrombus filling a side branch of the right vertebral artery (RVA). The side branch is distended, with necrosis of the arterial wall (arrows). Osteoid (O) and loose fibrovascular tissue of the aneurysmal bone cyst is seen on both sides of the arterial branch. Sectioning artifact (SA) is also seen. (Block 28, C2 vertebra, level 352, Movat’s pentachrome stain, ×20 original magnification.)
Discussion
ABCs are rare lesions, and controversy persists regarding not only the etiology of this lesion, but also the best treatment. ABCs are composed of cavernous vascular channels separated by fibrous septa, which lack endothelial lining. They are thought to develop through thrombosis of intraosseous veins, through hemorrhagic outflow in a pre-existing bone lesion such as hemangioma, or secondary to a bone tumor. Under this concept, ABCs were classified in primary and secondary lesions. Primary ABCs are found in children and are not associated with any other tumors, whereas secondary ABCs are common in adults and develop in the context of fibrous dysplasia, chondroblastoma, osteosarcoma, or giant cell tumors of the bone. ABCs show typical imaging features on CT and MR images with cortical thinning and destruction and either multiple double fluid level cysts or an additional solid component. Nevertheless, many authors strongly recommend biopsy for tissue diagnosis (4, 5). Needle biopsy is the mode of choice to obtain tissue for histologic evaluation, although it carries the risk of hemorrhage or failure to make a diagnosis.
Because of the rarity of the lesion, no established therapeutic regimen exists. Traditionally, the treatment of choice of ABCs has been surgical resection, but the high recurrence rate (10–60%) in some series, especially after curettage, has led to other treatment options (6, 7). These include selective arterial embolization either as sole treatment or as an adjunct to surgery, radiation therapy, injection of methylprednisolon and calcitonin or radionuclides, and percutaneous Ethibloc injection.
En bloc total resection is associated with the lowest recurrence rate, although surgical resection may not be possible without significant risk and morbidity (8). A combined posterior and anterior approach with stabilization may be required. The ABC in the present case involved the anterior and posterior elements and encased the vertebral artery on the right side. Surgery in this case was considered to have significant risk and morbidity.
Ethibloc is a fibrosing agent that has been reported to have encouraging results in small series of benign bone cysts, and was recommended as primary management of ABCs, including those of the spine, by some authors (3, 4, 6, 9). Ethibloc is an emulsion of zein, alcohol, oleum papaveris, propylene glycol, and a contrast medium. It thickens immediately on contact with an aqueous solution causing it to convert to the consistency of chewing gum and then harden (2). Ethanol enhances the necrotic effect of zein and induces intravascular thrombosis, local inflammation, and, finally, fibrotic reaction, which may subsequently lead to reparative processes and remineralization by osteoblasts. Injection of Ethibloc into bone cysts is an off-label use of the device and in Canada requires approval from Health Canada. Before Ethibloc injection, the diagnosis of an ABC should be affirmed, because it may alter any subsequent histologic findings. It has been suggested that contrast medium is injected to ensure the intracavitary location of the needle and to exclude leakage into soft tissue or the venous system before Ethibloc injection (3, 4, 6, 9). The contrast agent is then aspirated and Ethibloc injected at a slow speed but at a higher pressure than that of contrast agent because of its high viscosity. The amount depends on the cyst size, but there is no clear standard given as how to calculate the volume required for the ABC. Reported complications after Ethibloc injection include inflammatory reactions, local pain, fever, local abscess, and pulmonary embolism. One report alluded to the inadvertent risk of leakage into the spinal vessels in spinal ABCs, but this has not been reported to date (6). To our knowledge, there is no report in the literature about the possible escape of embolization material into the arterial system.
We suspect that Ethibloc passed into a side branch of the vertebral artery running into the ABC. Retrograde communication between an ABC and the arterial supply has not previously been shown. The lack of a distinct needle tract in the sections in the region of the needle puncture is consistent with Ethibloc solidifying in the bone cyst and softening of the tissue due to decalcification, which was necessary to cut the sections but caused some artifactual tissue disruption on cutting the section. Alternatively, the needle possibly created a communication of the cyst with adjacent vessels, but this seems less likely.
Although Ethibloc injection for the treatment of ABCs has been reported to be a promising tool with total or partial regression rates of 87% and 13%, respectively, in the series of Guibaud et al (4), possible embolic complications such as the fatal case reported herein should be considered.
References
- Received June 30, 2003.
- Accepted after revision October 21, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.