
Abstract
Summary: We report a rare case of bilateral pericallosal artery ectasia with stenosis in a 49-year-old man complaining of frontal headache. CT showed a serpiginous calcified interhemispheric fissure lesion with contrast enhancement. Imaging of this lesion was pursued with MR and MR angiography; however, conventional cerebral angiography was needed to make a definitive diagnosis.
Dilatation, elongation, and tortuosity of the vertebrobasilar and distal internal carotid arteries are frequently encountered. Ectasia in branches of the anterior cerebral arteries without lipoma, however, is rarely seen (1–3). We report a case of ectasia of the pericallosal arteries and discuss its characteristic CT, MR imaging, and cerebral angiographic findings.
Case Report
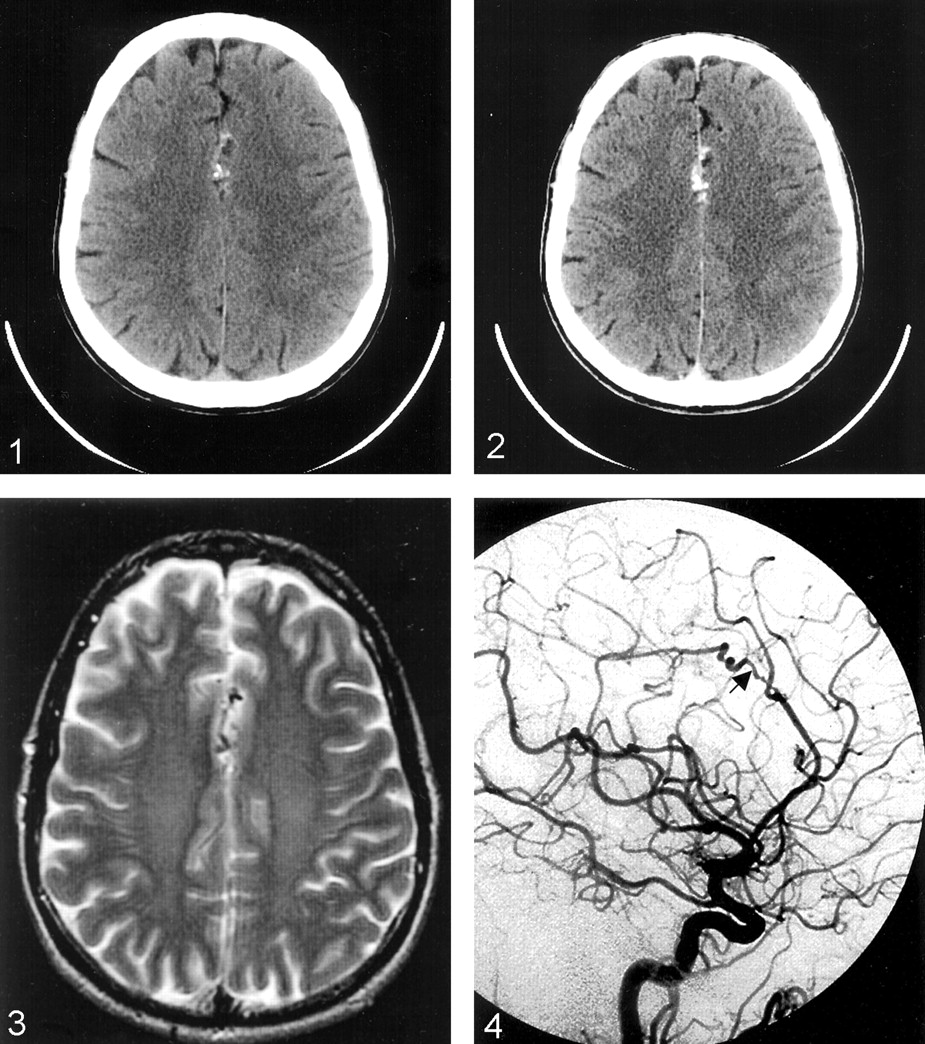
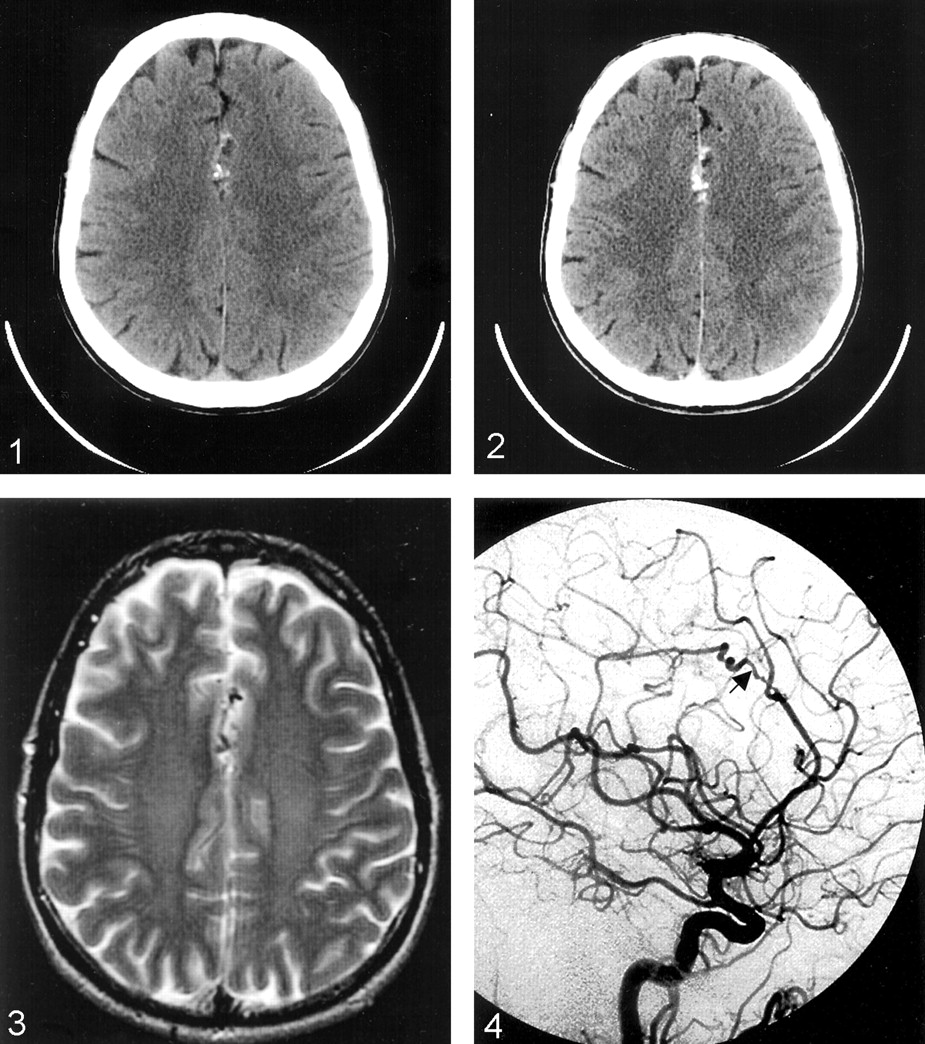
A normotensive 49-year-old man with no medical or surgical history and negative findings on neurologic and funduscopic examinations underwent CT for intermittent frontal headache that was unresponsive to 1 week of conservative treatment. CT revealed a hyperattenuated, interhemispheric-fissure lesion that enhanced after intravenous contrast agent administration. This lesion was suspicious for a calcified arteriovenous malformation (AVM) or dural fistula. To better characterize this lesion, the patient underwent MR imaging and MR angiography (MRA) studies. MR images showed calcifications and abnormal flow voids in the interhemispheric fissure closely following the corpus callosum without causing edema or mass effect. Upon contrast agent administration, these flow voids enhanced. MRA did not adequately demonstrate the distal anterior cerebral artery branches, although no other vascular lesions were seen.
To better characterize the nature of this vascular lesion, complete cerebral angiography was performed. It revealed bilateral, torturous pericallosal arteries without early venous drainage. The left pericallosal artery was noticeably stenotic immediately proximal to the region of ectasia. The carotid bifurcation and internal and external carotid and vertebrobasilar arteries were completely normal. No evidence of atherosclerotic disease, fibromuscular dysplasia, or vasculitis was seen. An MR imaging study of the cervical spine and CSF analysis were performed to search for a cause of the persistent frontal headaches. Serum analysis and echocardiography were performed to rule out collagen vascular diseases. No abnormality was found. The next day, the patient reported notable improvement in his frontal headaches despite no change in treatment. He was discharged and has not had recurrence of his headaches after several months of neurologic follow-up (Figs 1–4).

CT scan without contrast enhancement shows calcified interhemispheric lesion.

Postcontrast CT scan shows enhancing interhemispheric lesion.

Axial T2-weighted MR image shows interhemispheric flow voids.

Left lateral carotid angiogram. Arrow indicates region of stenosis and pericallosal ectasia.
Discussion
The torturous and elongated nature of this vascular anomaly fit the description of previously described cases of pericallosal arterial ectasia and dolichoectasia of the anterior cerebral atrteries (1–3). Dolicoectasia is more frequently encountered in the vertebrobasilar system, but it has also been described to exist in the middle and anterior cerebral arteries (4–6). Vertebrobasilar dolichoectasia can present with seizure, headache hydrocephalus, ataxia, dementia, stroke, and several cranial nerve deficits (7). These findings have been attributed to direct compression of intracranial structures and infarcts (7, 8). Anterior cerebral artery dolichoectasia has been associated with headaches, seizure, visual field defects, and mania (1–3, 5). There has been one report of subarachnoid hemorrhage caused by rupture of an A1-segment dolichoectatic vessel (6).
Initially, this case was suspicious for dural fistula or AVM owing to findings of calcification at CT and flow voids at MR imaging. Although vertebrobasilar artery dolichoectasia can be visualized using MR imaging and MRA, this technique cannot be relied upon for imaging distal anterior circulation lesions (4).
It was only by cerebral angiography that we were able to determine that the interhemispheric vascular anomaly seen using CT and MR imaging was indeed ectatic pericallosal arteries rather than an AVM or dural fistula. With angiography, the anatomy and flow dynamics of the entire intracranial and extracranial carotid and vertebrobasilar arteries could be studied. Although fibromuscular dysplasia has been reported in the A1 segment of the anterior cerebral artery, no findings suggestive of fibromuscular dysplasia were seen (9). No atherosclerotic plaques were noted in any arteries of the head or neck.
Acquired dolichoectatic intracranial arteries have been attributed to arteriosclerosis, hypertension, septic emboli, lipomas, and trauma (10). Congenital dolicoectasia is thought to be caused by defects in the arterial wall or migrational abnormalities (2). The histologic charateristics of these vessels frequently show hyaline degeneration of muscular layers and abrupt gaps in the internal elastic membrane (5, 10, 11). Accordingly, patients with polycystic kidney disease and Marfan syndrome have an increased incidence of dolichoectasia (12). Cases with concurrent medial frontal lobe thickening have been reported as well, which suggests a neuronal migration abnormality along the anterior cerebral artery (2).
Dilated and torturous intracranial arteries can be calcified and harbor atherosclerotic plaques. These areas of focal atherosclerosis and calcification can be caused by turbulent forces against the endothelium. In histologic studies, dolichoectatic arteries have been shown to have multiple, abrupt gaps of the internal elastic membrane where tissue of the media bulges through forming plaquelike excrecences into the arterial lumen (5). Because atherosclerotic stenosis and vessel-wall defects appear similar angiographically, it is unknown whether our patient’s stenotic left pericallosal artery is caused by a focal defect in the arterial wall or formation of an atherosclerotic plaque.
The cause of bilateral pericallosal artery ectasia with unilateral focal stenosis in this patient is not determined. It is possible this lesion is congenital, because the patient has no history of intracranial infection, trauma, or atherosclerosis, and no lipoma was visualized at MR imaging. Because the headaches resolved with no real intervention and have not recurred after several months of follow-up, the patient’s headaches may have been an incidental finding.
We hope this case reminds readers that this condition may mimic the CT and MR imaging findings of the AVM. Cerebral angiography may be needed for definitive diagnosis until enough experience is accumulated on the CT and MR imaging appearance of this lesion.
References
- Received June 15, 2003.
- Accepted after revision November 18, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.