
Abstract
Summary: The HydroCoil Embolic System (HES) comprises a platinum microcoil coated with an expansile polymer and is approved by the United States Food and Drug Administration for cerebral aneurysm occlusion. We report a series of five cases, two in the internal carotid artery and three in the vertebral artery, in which the HES was used for parent artery occlusion procedures. In each of these cases, the HES allowed rapid, short-segment occlusion.
The ideal treatment option for some types of intracranial vascular diseases may include parent artery occlusion (PAO). For example, large or giant ophthalmic segment aneurysms can be cured with carotid PAO (1, 2) and intracranial vertebral artery dissections can be treated with vertebral artery PAO (3, 4). Various devices have been used to achieve vessel occlusion, including detachable balloons and coils. Safe, reliable occlusion may be achieved with each type of device in most cases (1–4).
The Hydrocoil Embolic System (HES, MicroVention, Inc, Aliso Viejo, CA) has recently been developed for the endovascular treatment of intracranial aneurysms, and has been granted United States Food and Drug Administration approval for that application (5). The HES device consists of a carrier platinum coil coupled with an expandable hydrogel material, which increases sevenfold in volume when placed into a physiologic environment. Within aneurysm cavities, the expanded hydrogel achieves high rates of volumetric occlusion compared with that in platinum coils (6).
We hypothesized that the HES could be applied to achieve rapid, precise, targeted PAO procedures, even in short segments of vessel. On the basis of this hypothesis, we used the HES system in a series of patients presenting with cervical and intracranial pathologic findings requiring either vertebral or carotid PAO. We report herein our experience with the HES in PAO procedures.
Description of Technique
Clinical characteristics and other data are shown in the Table. In general, vessel access was achieved with 6F guiding catheters. Systemic heparinization was administered to achieve activated clotting times (ACT) greater than 250 seconds. The HES is available in multiple expanded diameters, secondary diameters, and lengths and can treat vessels ranging in diameter from 2 mm to 6 mm. For this case series, we used an HES-14 for vertebral PAO (n = 3) and internal carotid artery (ICA) PAO (n = 2) and an HES-18 for a carotid PAO procedure (n = 1). Before placement of HES devices, a detachable platinum coil, ideally an 18-type coil rather than a 10-type coil, was placed in each case. This initial coil served to stabilize the HES devices and is recommended on the basis of preclinical experience in which HES devices placed without such stabilizing platinum coils migrated distally as the polymer expanded (unpublished data). The initial platinum coil should be oversized 1–2 mm relative to the diameter of the parent artery, and as tight a basket as possible should be achieved with this coil.
Lesion types and devices utilized
Following detachment of the initial platinum coil, we proceeded with HES placement. The HES was relatively undersized compared with the parent artery diameter to achieve a dense-as-possible packing of the hydrogel-bearing devices. In our opinion, larger-diameter HES devices would have yielded less dense packing of the hydrogel material as compared with small-diameter devices. Placement of the first two HES devices was done relatively rapidly to achieve dense packing of devices before full expansion of the hydrogel material. Immediately following placement of the second HES device, control angiography was performed from the guiding catheter. Additional devices were placed as needed.
We catalogued the vascular disease, vessel location and diameter, and type and number of devices required to achieve vessel occlusion (Table).
Representative case
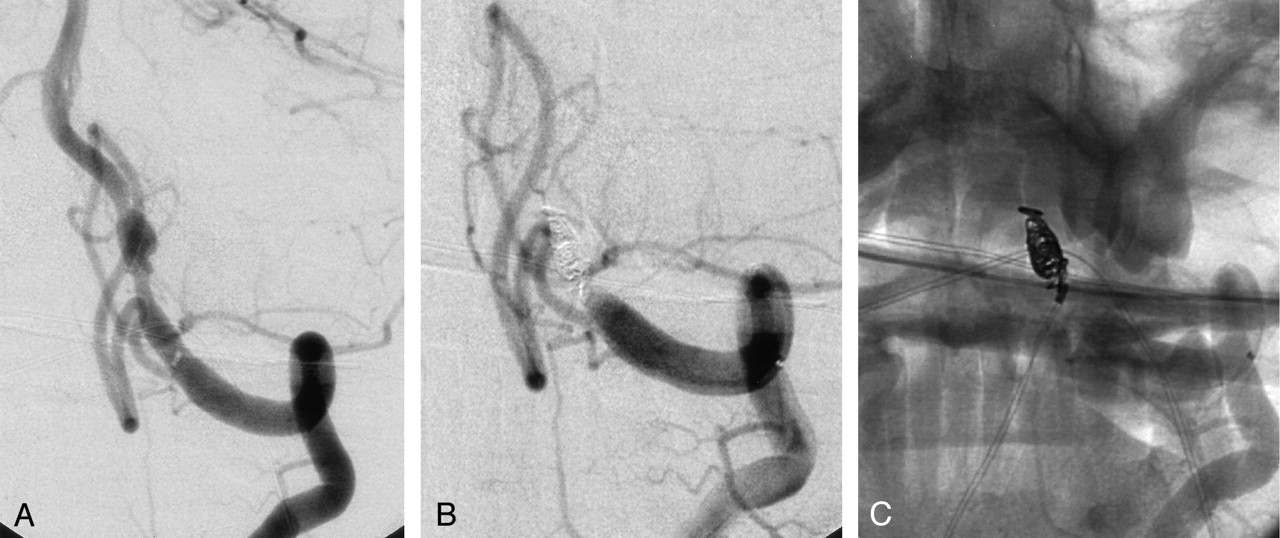
A 53-year-old male patient presented with acute subarachnoid hemorrhage. A cerebral angiogram demonstrated a dissection along the intracranial portion of the left vertebral artery. The dissection began approximately 10 mm distal to the left posterior inferior cerebellar artery (PICA) (Fig 1A). Occlusion of the dissected segment of the vertebral artery was considered the ideal treatment option. Furthermore, we hoped to avoid manipulation of the dissected portion of artery yet maintain patency of the PICA. To achieve these goals, short-segment occlusion of the left vertebral artery, immediately proximal to the most proximal aspect of the dissection, was undertaken. Using a 6Fr Envoy guiding catheter (Cordis Neurovascular, Miami Lakes, FL) and Excelsior microcatheter (Target, Boston Scientific, Fremont, CA) we placed a 4 mm T18 Micrus Spherical coil (Micrus Corp, Sunnyvale, CA) just proximal to the dissection. Subsequently, we placed two separate 2mm × 5 cm HydroCoil 14 devices within the initial platinum coil. Vessel occlusion was noted less than 5 minutes following deployment of the first HydroCoil (Fig 1B, C). The PICA was preserved.

A, Oblique digital subtraction angiogram of the left vertebral artery demonstrates a fusiform, dissecting aneurysm. The aneurysm is located approximately 10 mm distal to the origin of the posterior inferior cerebellar artery.
B, Oblique digital subtraction angiogram following coil occlusion of the left vertebral artery. The coils were placed in the segment of artery between the posterior inferior cerebellar artery origin and the proximal aspect of the dissection. The posterior inferior cerebellar artery was preserved.
C, Nonsubtracted image of the coil mass from the digital subtraction angiogram (B).
Discussion
This case series demonstrates that the HES can be used to achieve occlusion, even in short segments of vessel. In the case of vertebral PAO, device placement within vessel segments as short as 6 mm could achieve occlusion. Typically, a single platinum coil and two HES devices were needed for vessel occlusion. It remains possible that a single HES device could have achieved occlusion, but we chose to rapidly place at least two HES devices before performing control angiography to maximize attenuation of HES packing.
Preclinical experimentation with the use of HES in PAO has demonstrated durable occlusion of embolized arteries over 90 days. Significant thrombic organization proximal to the embolization site was observed (unpublished data).
Previous case series have detailed the use of detachable balloons and platinum coils, both fibered and nonfibered, for PAO procedures (1–4). Detachable silicone balloons have recently been withdrawn from the market. Nonfibered platinum coils may fail to achieve short-segment occlusion, given their nonthrombogenic nature. Fibered coils may offer improved ability to achieve vessel occlusion relative to nonfibered platinum coils. The HES expands to fill a larger volume of the vessel lumen, after it enters the artery, analogous to a balloon.
References
- Received February 2, 2004.
- Accepted after revision March 7, 2004.
- Copyright © American Society of Neuroradiology




{kind=link}