
Abstract
Summary: We present the case of bilateral anomalous origin of both vertebral arteries (VAs) in a 20-year-old male patient who presented for routine contrast-enhanced CT follow-up examination of the chest. Contrast-enhanced CT revealed abnormal origins of both the VAs from the aortic arch distal to the origin of the left subclavian artery. Following this, CT angiography was performed, which confirmed the findings. To our knowledge, this is the first report of anomalous origins of both VAs beyond the origin of the left subclavian artery. The possible embryonic mechanism and the clinical importance of this variant is also reviewed.
The vertebral artery (VA) is clinically described as the first branch of the ipsilateral subclavian artery; however, multiple variations in the origin of that vessel have been reported in the literature. This variation in the origin of VA is asymptomatic. Nonetheless, diagnosis of these abnormalities in cases of vascular diseases such as arteriovenous malformations or aneurysms, before cerebral angiography, is important to avoid wrongly interpreting nonopacifiation of VAs as a blockage or stenosis that may prove dangerous during the endovascular surgeries in the head and neck region.
Case Report
A 20-year-old male patient with a known case of spondyloepiphyseal dysplasia (SEMP-Strudwick type) with various congenital bony deformities of the limbs and the face and with past history of rickets and cholecystitis, was referred to our department for contrast-enhanced CT of chest as a follow-up examination after receiving antituberculous treatment for pulmonary tuberculosis. The chest CT (lung windows) was unremarkable, apart from few fibrotic changes in the bilateral upper lobes. On mediastinal window settings, the study revealed the aortic origin of left VA, which is a comparatively common finding. What was remarkable, however, was the origin of left VA distal to the origin of left subclavian artery. It further showed an anomalous vessel arising from the posteroinferomedial surface of the aortic arch and then going in the right paratracheal region, beyond which the course was not traceable. As a result, we performed CT arch aortography of the patient after injecting 100 mL of iodinated contrast media via the left antecubital vein at the rate of 3.0 mL/s starting from the D10 level until the base of skull. The origin of left VA from the aortic arch beyond the origin of the left subclavian artery was confirmed. It entered the ipsilateral foramen transversarium of the 7th cervical vertebra. The aberrant vessel arising from the posteroinferomedial surface of the aortic arch distal to the origin of the left VA, coursed behind the trachea and the esophagus and in front of D4 vertebral body to reach the right paratracheal region and entered the right foramen transversarium of the 7th cervical vertebra. Thus, the aberrant vessel was in fact the right VA with anomalous origin (Figs 1 and 2). The origin of the right VA from the ipsilateral subclavian artery was lacking, thus ruling out duplication of the VA from the aortic arch and the subclavian artery. This right VA was of smaller diameter than the left VA. After entering the foramen transversarium, both the VAs revealed a further normal course with normal formation of the basilar artery (Figs 3 and 4). The anatomic relationship of the rest of the supraaortic arteries was confirmed to be normal.

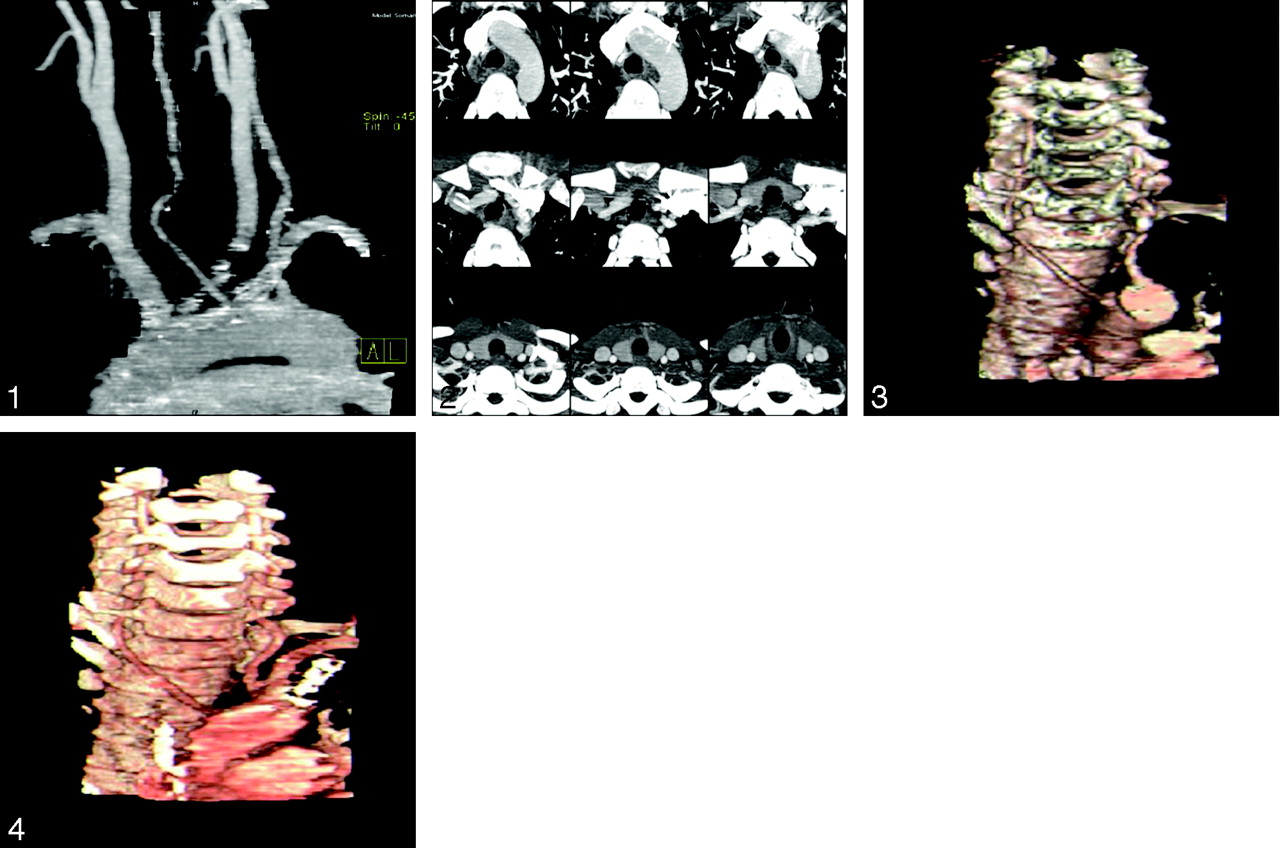
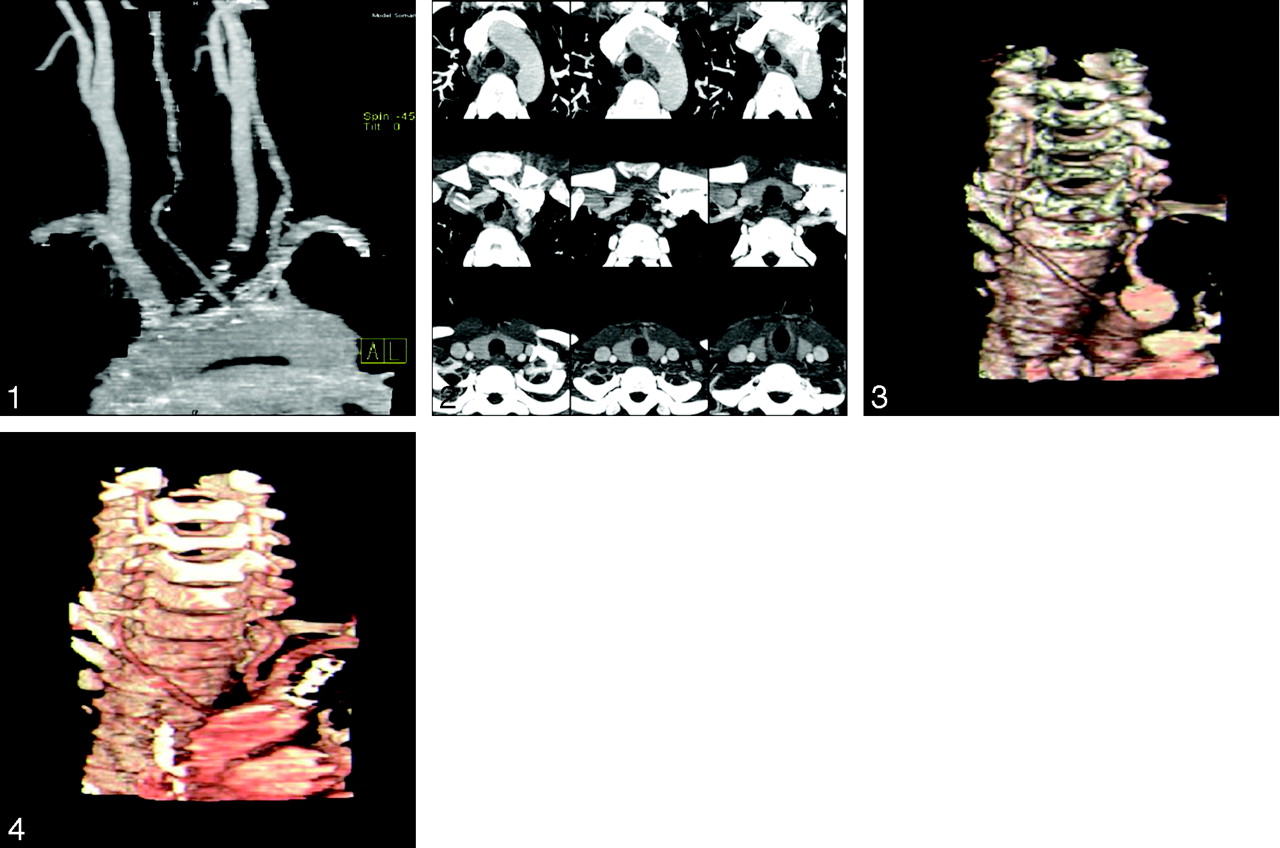
Maximum intensity projection (MIP) image depicting the origin of all the supraaortic branches, including the anomalous origin of both the VAs from the arch, beyond the left subclavian artery.

Serial axial MIP images demonstrating the anomalous origin of both the vertebral arteries from the aortic arch beyond the left subclavian artery, along with the aberrant course of the right vertebral artery behind the esophagus and the trachea to reach the right paratracheal region and then to enter the right transverse foramina.

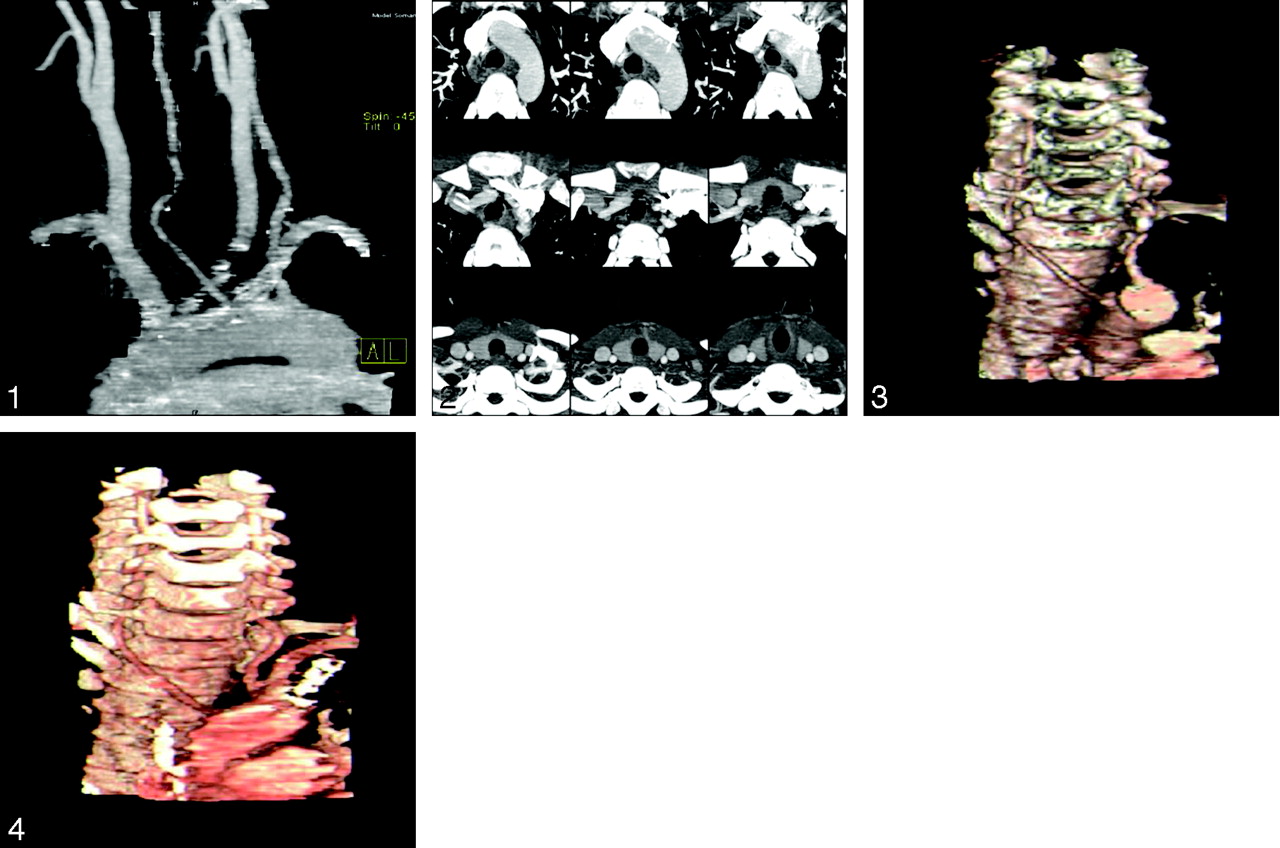
Volume rendered images showing the aortic arch origin of both the vertebral arteries.

Volume rendered images showing the anomalous origin of both the vertebral arteries from the arch of aorta beyond the left subclavian artery.
Discussion
Although the VA is classically described as first branch of ipsilateral subclavian artery, multiple variations in the origin of the VA have been reported in the literature, such as the VAs can arise from the aortic arch, the common carotid, or the internal or carotid arteries. They also may have duplicate origin from the arch and the subclavian artery (1). The most frequent variant (2.4–5.8%) is the left VA arising directly from the aortic arch between the left common carotid artery and left subclavian artery (1). In such cases, the VA generally enters the transverse foramen of C4–C5 rather than C6 (2). On the other hand, aortic arch origin of the right VA is a rare anatomic variant. In such instances, the right VA generally arises distal to the supraaortic trunk. In a literature review in 1999, Lemke et al (1) found only nine cases in which the right VA originated from the aortic arch. In that study, the right VA originated between the left common carotid and the subclavian artery (one case), between right subclavian and the right common carotid artery in absence of formal innominate artery (one case) and distal to the left subclavian artery (seven cases). A bilateral aortic origin of VAs represents an exceptional anatomic variant (2). There are only two previously reported cases of the arch origin of the bilateral VAs. In one of them, both VAs arose proximal to the left subclavian artery (3). In the other reported case, the left VA arose between the origins of the left common carotid and left subclavian arteries and the aberrant right VA arose from the descending aorta distal to the origin of the left subclavian artery (4). On the other hand, in our case, both VAs had an aortic arch origin, distal to the left subclavian artery, an anatomic configuration that, to our knowledge, has not previously been reported. The incidence of an aortic arch with more than five branches is low. In his comprehensive review in 1916, Poynter (5) recorded only 31 cases of aortic arch with five branches and four cases with six branches. In seven of these 35 cases, both VAs arose from the aortic arch. The aortic branching pattern in proximal to distal progression was as follows: (1) innominate artery (IA), right vertebral artery (RVA), left common carotid artery (CCA), left VA and left subclavian artery (SA) (four cases); (2) right SA, right VA, right CCA, left CCA, left VA and left SA (three cases).
The variant of the right VA originating from distal to the left SA or as a last branch of aortic branch has been previously published in eight cases (1, 4). To the best of our knowledge, however, anomalous origin of both the VAs directly from the aortic arch and both distal to the left SA has not been previously reported.
To understand the hypothetical development of the anomalous origin of the VA, knowledge of embryonic development of the aortic arch and the brachiocephalic vessels is necessary (3). Embryologically, the right SA develops partially from right primitive dorsal aorta. During this process, the caudal part of the dorsal aorta is obliterated just before the confluence with the left dorsal aorta and the C7 intercostal artery continues as the SA (3, 5). The VA arises from the postcostal longitudinal anastomosis between the C1 and the C7 intercostal arteries and the cervical intercostal obliteration zone (6). A separation of the right VA origin from the SA is due to either migration of the VA into dorsal aorta or separate development of VA from C6 or C8 intercostal artery instead of C7 intercoastal artery (2, 3). If the VA arises from the C8 intercoastal artery and the physiologic obliteration of the right dorsal artery is distal to C7 intercostal artery, however, only the origin of right VA is moved to the left. In this process, the right SA originates from the right side of aorta and the right VA originates from the left side of the aortic arch, distal to the left SA, (2), as in the case presented here. The aberrant origin of the left VA directly from the aortic arch is due to persistence of the 8th intersegmental artery (3). Thus, the aortic branching pattern observed in our patient is due to the combination of the persistent 8th intersegmental artery and from an aberrant right VA from the C8 intercostal artery with secondary proximal migration.
In most of the cases reported in the literature, anomalous origin of the VA did not result in clinical symptoms. Some patients complained of dizziness, however, which was thought to have no connection to the anomalous origin of the VA. Although some have hypothesized that an anomalous origin and distribution of a large cervical artery might result in cerebral hemodynamic perturbation with secondary cerebral changes, no conclusive evidence suggests that an anomalous VA origin predisposes an individual to cerebrovascular disorders (1, 5). The true value of detecting anomalous origin is in the diagnostic gain before vascular surgeries of supraaortic arteries, and the knowledge of potential VA origin variants appears to be mandatory for planning aortic arch surgery or endovascular interventions. Anomalous VA origin also represents a potential pitfall in diagnostic cerebrovascular injury. One or both VAs may be wrongly assumed to be occluded or diseased, either by eluding catheterization during angiography or by lying outside the region of interest during noninvasive studies such as CT angiography, MR angiography, or Doppler sonography.
- Received April 9, 2004.
- Accepted after revision May 2, 2004.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}