
Article Figures & Data
Figures
- Fig 1.
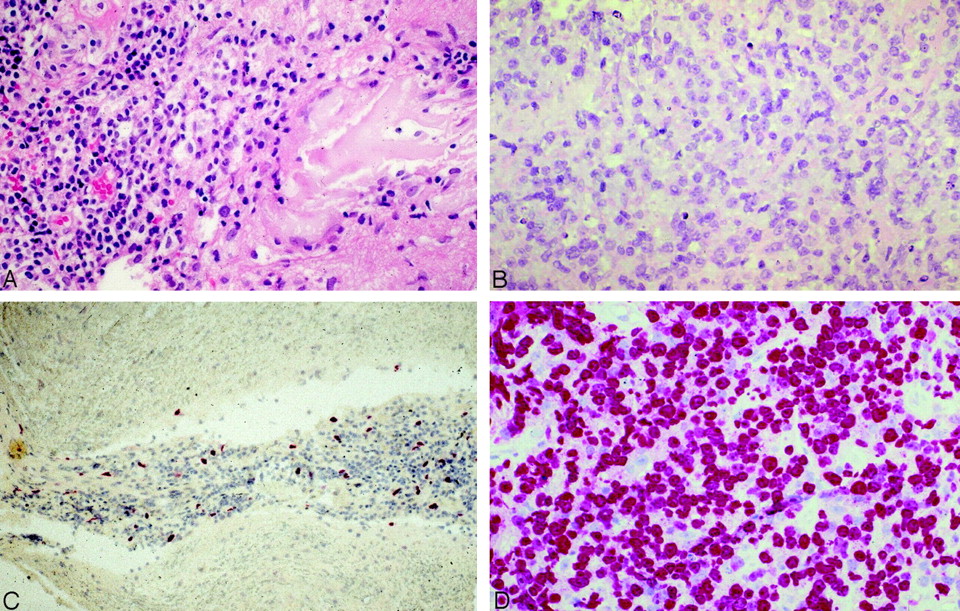
Histologic preparations of low-grade PCNSLs (patient 9; lymphoplasmacellular lymphoma), opposed to high-grade PCNSLs. A, Infiltrates of small, mature lymphocytes surrounded by amorphous substance (immunohistologic demonstration of light-chain deposits) and absence of blastic, immature cells (hematoxylin and eosin; original magnification ×400). The lymphocytes are positive for the B-cell antigen CD20 and show a predominant expression of the immunoglobulin light chain lambda, indicating monoclonality (not shown). B, Typical appearance of high-grade PCNSL, composed of immature blasts with large and partly bean-shaped nuclei and prominent nucleoli (hematoxylin and eosin; original magnification ×400). C, Lymphoma cells of low-grade PCNSL demonstrate a low growth fraction of only 2% (Ki-67 antibody; original magnification ×200). D, High-grade PCNSL with a typical high growth fraction of 95% (MIB-1 antibody; original magnification ×400). Note.—Reproduced from K. Jahnke et al, Br J Haematol 2005;128:616–624 (© British Society for Haematology).
- Fig 2.
Case 3, 60-year-old man with low-grade B-cell lymphoma (no further histologic specification). A, T2-weighted turbo spin-echo sequence. B, Precontrast T1-weighted spin-echo sequence. C, Postcontrast T1-weighted spin-echo sequence. On the precontrast T1-weighted image, the lymphoma (arrows) already demonstrates mild hyperintense spots, and only minor contrast enhancement is noted on the postcontrast T1-weighted sequence. In addition, on T2-weighted imaging, periventricular and basal ganglia edema is noted. Note.—Reproduced from K. Jahnke et al, Br J Haematol 2005;128:616–624 (© British Society for Haematology).
- Fig 3.
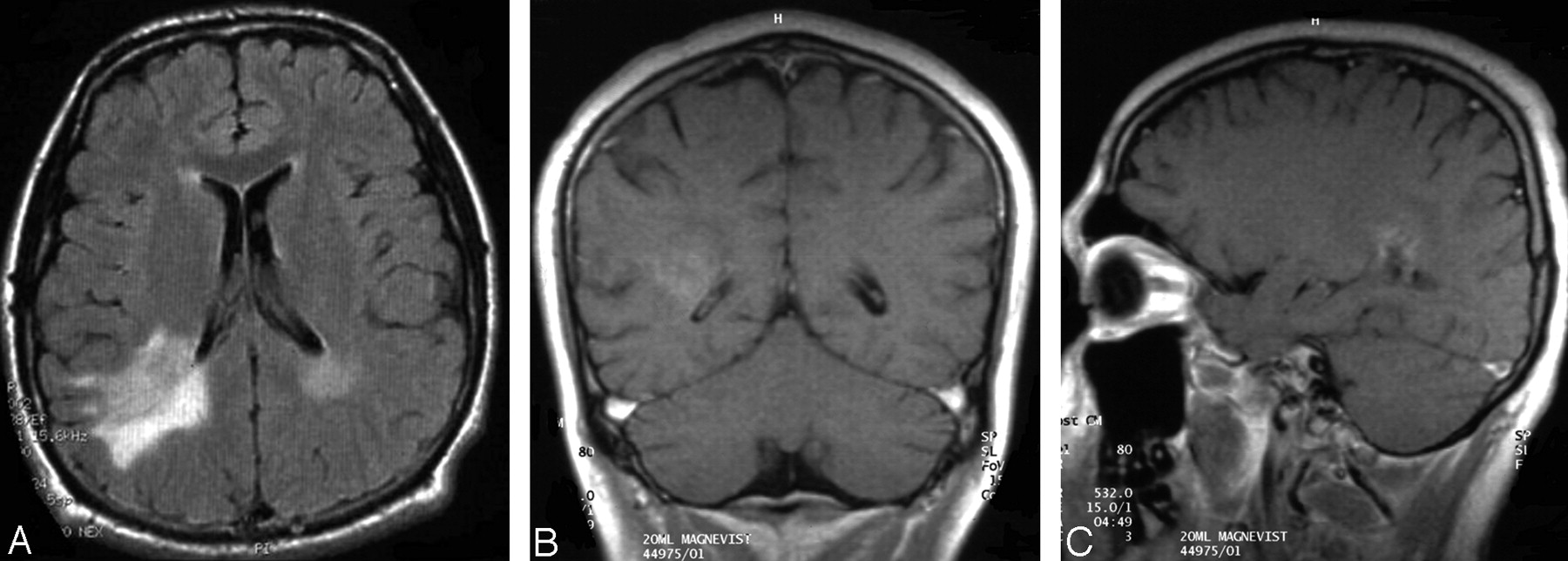
Case 9, 19-year-old man with low-grade B-cell lymphoma (subtype lymphoplasmacellular lymphoma). A, Extensive hyperintense appearance of the lesion adjacent to the posterior aspect of the right lateral ventricle in FLAIR sequence. B and C, Surprisingly low contrast enhancement on T1-weighted imaging. Moderate edema is noted on T2-weighted imaging (not shown).
- Fig 4.
Case 1, 58-year-old man with an intramedullary low-grade T-cell lymphoma. A, T2-weighted turbo spin-echo sequence. B, Postcontrast T1-weighted spin-echo sequence with 2 lymphoma manifestations, situated at the level of the cervicothoracic junction and the thoracic vertebrae 4 and 5 (arrows). Both lesions demonstrate pronounced local edema. The upper lesion shows a marked, homogeneous contrast enhancement, whereas the lower lesion demonstrates only mild contrast enhancement. This patient did not have cerebral lymphoma manifestations. Note.—Reproduced from K. Jahnke et al, Br J Haematol 2005;128:616–624 (© British Society for Haematology).
- Fig 5.
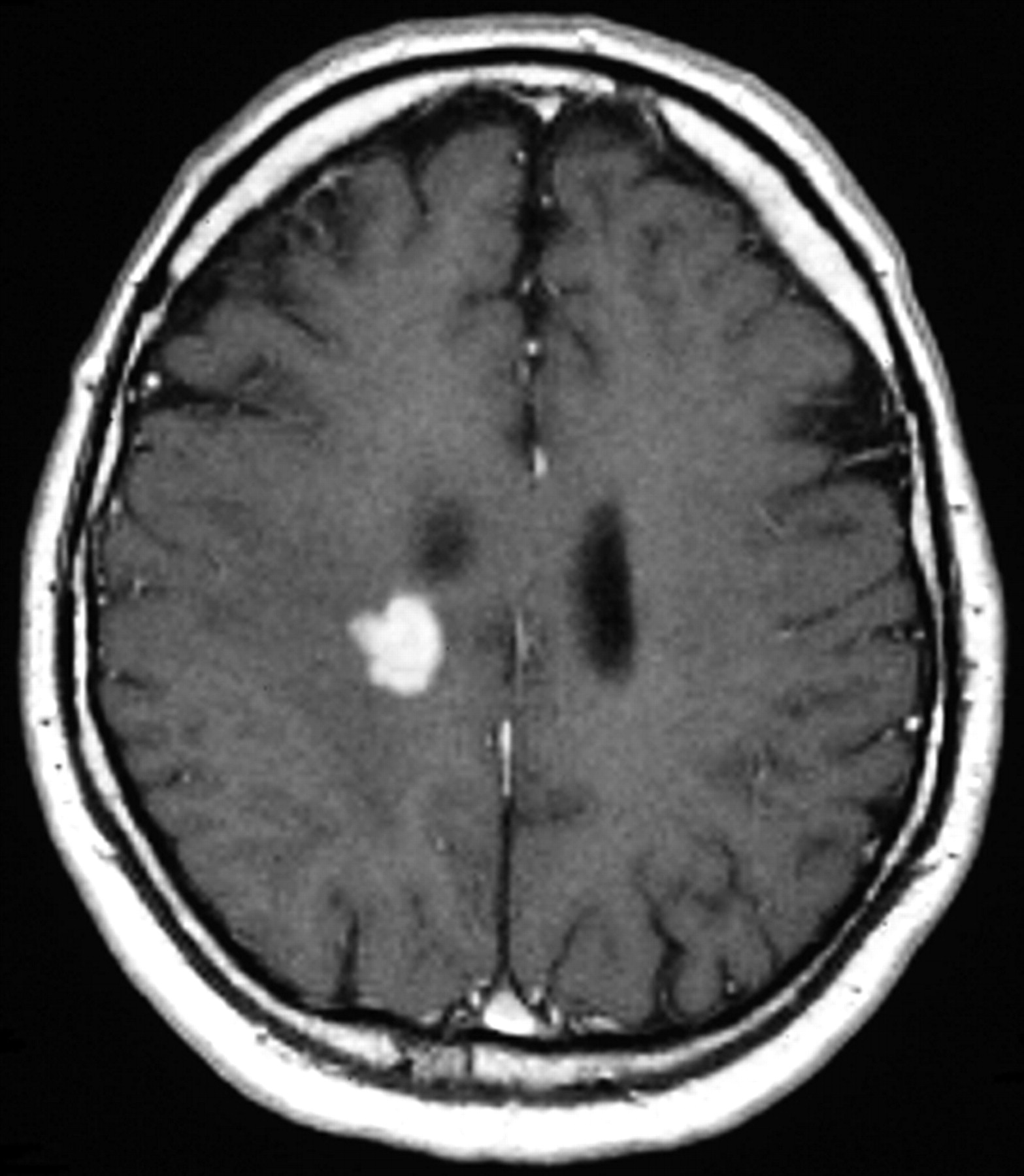
Case 2, 58-year-old man with T-cell lymphoma. A right periventricular lesion with strong and homogeneous contrast enhancement is noted on T1-weighted postcontrast spin-echo sequence. Despite radiologic features typical of high-grade PCNSLs, histopathologic investigation revealed a low-grade PCNSL with a growth fraction of 1%.
- Fig 6.
Case 10, 45-year-old man with low-grade B-cell lymphoma (no further histologic specification; arrows) with bifrontal hyperintense periventricular white matter lesions on A, T2-weighted, and B, FLAIR images. C, The lesions are not visible on T1-weighted precontrast imaging. D, No contrast enhancement is noted on the T1-weighted postcontrast section. E, This T2-weighted image additionally demonstrates a small area of hyperintensity located in the head of the corpus callosum.






Tables
Patient no. 1 2 3 4 5 6 7 8 9 10 Sex/age (y) M/58 M/58 M/60 F/61 F/61 M/58 M/60 F/60 M/19 M/45 Clinical symptoms Focal motor/sensory deficits Hemiparesis Ataxia, diplopia, neuropsychologic deficits, somnolence Cerebellar syndrome, neuropsychologic deficits Focal sensory deficits Epilepsy (grand-mal) Epilepsy (grand-mal), ataxia, nmestic deficits, incontinence None Epilepsy (grand-mal status) Neuropsychologic deficits KPS (initially/at last follow-up), % 40/30 80/90 80/50 80/80 80.60 70/90 60/60 70/100 20/100 20/100 Median time to diagnosis (months) 1 1 1.5 2.5 0.5 32 2 0.5 3.5 6.5 Biopsy site Cervicothoracic spinal cord Right parietal Left basal ganglia Left parietal Right thalamus Left temporal Right frontal Left occipital Right temporal Left frontal Histopathology, growth fraction (Ki67/MIB-1) T-cell (perivascular infiltrates; small, mature lymphocytes); Ki-67/MIB-1: 20% T-cell (perivascular infiltrates; small, mature lymphocytes); Ki-67/MIB-1: 1% B-cell, not specified (perivascular infiltrates; small, mature lymphocytes with round nuclei); Ki-67/MIB-1: 1% B-cell, not specified (perivascular infiltrates; small, mature lymphocytes with round nuclei); Ki-67/MIB-1: 5% T-cell (perivascular infiltrates; small, mature lymphocytes with irregularly shaped nuclei); Ki-67/MIB-1: <5% B-cell, lymphoplasmacellular (small, mature lymphocytes with round, eccentric, nuclei); Ki-67/MIB-1: <5% Follicular lymphoma (diffuse variant), grade 1 (small cells with cleaved nuclei (centrocytes), 3 large cells per hpf with scant, basophillic cytoplasm, round to oval nuclei, 1–2 nucleoli (centroblasts); Ki-67/MIB-1: <5% B-cell, not specified (infiltrates with small, mature lymphocytes with round nuclei); Ki-67/MIB-1: 15% B-cell lymphoplasmacellular (small, mature lymphocytes with round, eccentric, nuclei); Ki-67/MIB-1; 2% B-cell, not specified (perivascular, small, mature lymphocytes with round nuclei); Ki-67/MIB-1: 4% Therapy Total resection, HDMTX, local RT HDMTX, WBI HDMTX HDMTX BMPD, MTX i.th. none BMPD, MTX i.th., CHOP, WBI HDMTX HDMTX HDMTX, WBI PFS/OAS (months) 3/5.5 27+/27+ 44.5+/44.5+ 22.5/22.5 2/3 14.5+/14.5+ 54+/54+ 58+/58+ 33.5+/33.5+ 10+/10+ Last status Died due to sepsis CR CR Died due to acute renal failure Died due to lymphoma CR CR CR NC CR Note.—KPS indicates Karnofsky performance score; Ki-67/MIB-1, growth fraction of neoplastic cells as evidenced by staining with Ki-67 or MIB-1 antibody; hpf, high-power field of 0.159 mm2; (HD)MTX, (high-dose) methotrexate; RT, radiotherapy; WBI, whole-brain irradiation; i.th., intrathecally; BMPD, BCNU, methotrexaste, procarbazine, dexamethasone; CHOP, cyclophosphamide, doxorubicin, vincristine, prednisolone; PFS, progression-free survival; OAS, overall survival; CR, complete response; NC, no change.
Patient No. No. of Lesions Location of Lesions Enhancement T2-Weighted Image 1 (Fig 4) 2 Spinal cord (cervico-thoracal) Strong, homogeneous Hyperintense, marked edema Spinal cord (Th 4–5 level) Moderate, homogeneous 2 (Fig 5) Multiple Right parietal (periventricular), cerebellar Strong, homogeneous Hyperintense, moderate edema 3 (Fig 2) Multiple Basal ganglia bilaterally Moderate, heterogeneous Hyperintense, marked edema 4 2 Basal ganglia (superior to sella) Strong, homogeneous Hyperintense, moderate edema Left parietal Isointense, edema absent 5 1 Right thalamus (periventricular) Strong, heterogeneous Hyperintense, moderate edema 6 Multiple Left temporal, left basal ganglia Moderate, heterogeneous Hyperintense, marked edema 7 1 Right frontal (periventricular) Strong, homogeneous Hyperintense, moderate edema 8 1 Left occipital Moderate, heterogeneous Hyperintense, moderate edema 9 (Fig 3) Multiple Right temporal/occipital (periventricular) Moderate, heterogeneous Hyperintense, marked edema 10 (Fig 6) 1 Bifrontal (periventricular) + caput corporis callosi None Hyperintense, moderate edema Characteristics Number of Patients Number of lesions 1 4 2 2 >2 4 Localization Supratentorial/supra- and infratentorial 8/1 Spinal 1 Deep/superficial/both 2/3/4 Necrosis 1 T2-weighted signal* Hyperintense/isointense 10/1 Contrast enhancement* Strong/moderate/none 5/5/1 Homogeneous/heterogeneous 5/5 Edema* Marked/moderate/absent 4/6/1 Ventricular ependymal involvement 5 * Some patients had multiple sites and appearances of involvement.
- TABLE 4.
Comparison of radiologic and clinical characteristics between low-grade and high-grade PCNSL in immunocompetent patients
Low-Grade PCNSL High-Grade PCNSL Radiological morphology Moderate and inhomogeneous or absent contrast enhancement frequent Usually strong and homogemeous contrast enhancement Localization of lesions often without contact to subarachnoid space Lesions typically in contact with the subarachnoid space Hyperintensity of T2-weighted images often present Hyperintensity on T2-weighted images possible Location in deep brain structures and spine common Location in deep brain structures and spine possible but infrequent Clinical characteristics Indolent clinical course possible Aggressive clinical course almost invariably seen Delays in diagnosis establishment possible due to paucity of symptoms and variable radiologic appearance Diagnosis establishment usually rapid due to severe symptoms and typical radiological appearance Long survival with absence of complete tumor remission possible Survival without complete remission usually short Long survival after local treatment (surgery, local radiotherapy) possible Survival with local treatment short, whole brain treatment required Note.—PCNSL indicates primary central nervous system lymphoma.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging of Lymphomas Involving the CNS: An Update-Review of the Full Spectrum of Disease with an Emphasis on the World Health Organization Classifications of CNS Tumors 2021 and Hematolymphoid Tumors 2022
- Primary low-grade diffuse small lymphocytic lymphoma of the central nervous system
- Utility of Proton MR Spectroscopy for Differentiating Typical and Atypical Primary Central Nervous System Lymphomas from Tumefactive Demyelinating Lesions
- Primary hypothalamic third ventriclular Burkitt's lymphoma: a case report with emphasis on differential diagnosis