
Abstract
OBJECTIVE: Endoscopic third ventriculostomy (ETV) is increasingly used as alternative treatment for obstructive hydrocephalus. The aim of this study was to determine the utility of quantitative and qualitative examinations with cine phase-contrast MR imaging to determine the efficacy of ventriculostomy across time and whether CSF pulsation is restored after ETV.
METHODS: Thirty-eight patients treated with ETV were evaluated with cine phase-contrast MR within 1 month after surgery. Follow-up studies were performed after 1 year in 25 patients and after 2 years in 12. We evaluated flow void changes in the floor of the third ventricle and quantified the stroke volume at the site of the ventriculostomy. We also recorded changes in ventricular size and clinical outcome. To determine the restoration of CSF pulsation, we compared the CSF waveform at the ventriculostomy with the CSF waveform at the aqueduct in a healthy control group.
RESULTS: After ventriculostomy, restoration of pulsate motion characteristics of CSF circulation was observed. The stroke volume registered at ventriculostomy was maintained with time. There was a statistically significant relationship between clinical outcome and stroke volume. Overall flow magnitude was the most effective variable to determine which patients would improve after surgery. Values >75 mm3 showed a sensitivity of 76.7% and a specificity of 87.5% There was no relationship between ventricular size changes and clinical outcome. Patients with primary aqueduct stenosis had the best response to surgery, whereas patients with Arnold Chiari malformation or communicating hydrocephalus had the worst response.
CONCLUSION: Quantitative analysis with phase-contrast MR imaging indicates that ETV is an efficient technique for restoring CSF pulsation, with efficacy being maintained during the follow-up controls. Quantification of stroke volume at ventriculostomy is a good indicator of the functional status of ETV, and a high stroke volume in the ventriculostomy appears to be a positive predictor of favorable clinical outcome.
Neuroendoscopic third ventriculostomy has become a first-line treatment for obstructive hydrocephalus in several centers. The morbidity associated with this technique is low, and the success rates are high. It is essential, however, to ensure that this new internal shunt is effective. The outcome of the patients is obviously a key factor. Some reviews of the current literature have identified parameters that can be used to determine malfunction of the ventriculostomy. In addition to clinical outcome, particular attention has been paid to ventricular size reduction and the presence of a flow void in cine phase-contrast MR imaging (1–10). The aim of this study was to assess the usefulness of a cine phase-contrast MR measurement—stroke volume—as a parameter for predicting the functional evolution and state of ventriculostomy. We correlated quantitative volume data with clinical follow-up, ventricular size, and flow void signal intensity in cine phase-contrast MR. We were also interested in whether CSF circulation is restored after endoscopic third ventriculostomy (ETV) and whether the CSF flow pattern in the ventriculostomy is similar to that in the aqueduct.
Materials and Methods
All patients treated with neuroendoscopic ventriculostomy in the neurosurgery department between 1997 and 2000 were included in the study. The decision to perform this technique rather than ventriculoperitoneal shunt was made by the neurosurgeons.
Thirty-eight patients (25 men and 13 women; mean age, 39.5 years; age range, 11–74 years) with hydrocephalus were treated by neuroendoscopic ventriculostomy at the floor of the third ventricle anterior to the mammillary bodies during this period of time. The study was approved by our institutional review board, but patient informed consent was not provided because phase-contrast MR imaging was included during the standard follow-up MR studies after ventriculostomy.
Occlusive hydrocephalus was diagnosed in all but 3 patients. In 11 patients, the cause was primary aqueduct stenosis; in 18 patients, the cause was secondary stenosis due to intraventricular or extraventricular cystic or tumor lesions compromising CSF circulation at the third ventricle or aqueduct—9 tectum tumors, 6 pineal tumors, and 3 cystic lesions, including colloid cyst (Fig 1); and in 6 patients the cause was choroid plexus papilloma and neuroepithelial cysts) and Arnold Chiari malformation. We also included 3 patients with communicating hydrocephalus (2 with previous history of meningitis and the other with previous history of subarachnoid hemorrhage). No other diseases were associated.

A, Sagittal T1-weighted image located in the midsagittal plane shows a cystic lesion inside the aqueduct. B, Sagittal cine phase-contrast image after ventriculostomy shows flow signal intensity between third ventricle and pontine cistern.
Previous clinical symptoms in all patients (headaches, nausea and vomiting, vertigo, and, in some cases, absence seizures) were associated with increased intracranial pressure.
After the ETV, CSF flow MR studies were performed in all patients within the first postoperative month. Follow-up CSF flow MR studies were undertaken 1 year after the procedure in 25 patients and 2 years after the procedure in 12.
MR Imaging Techniques.
All initial CSF flow MR studies were performed with a 1.5T Siemens Magnetom 63SP system. Two series of cine phase-contrast MR imaging techniques were applied after performing spin-echo coronal T1-weighted images to locate the third ventriculostomy and evaluating ventricular size after surgery: one in the axial plane, with through-plane velocity encoding in the craniocaudal direction for flow quantification, and one in the sagittal plane, with in-plane velocity encoding in the craniocaudal direction for qualitative assessment.
Axial Technique.
CSF flow dynamics were quantitatively studied with the use of a prospective cardiac-gated high-resolution axial phase-contrast protocol with an imaging plane perpendicular to the ventriculostomy. The direction of flow encoding was craniocaudal. The imaging parameters were as follows: TR, 100 msec; TE, 16 msec; flip angle, 15°; number of acquisitions, 2; field of view, 160 mm; matrix, 512 × 512; scan thickness, 4 mm. Velocity encoding at 20 cm/s was initially selected and increased to 30 cm/s if aliasing was encountered. Depending on the patient’s heart rate, the measurement time lasted from 10 to 15 minutes, and 19 phase images were calculated.
Once the imaging data had been acquired, we transferred the images to a workstation and processed the images by using software provided by Siemens (Numaris version 2.5). A spherical region of interest was placed in the ventriculostomy shown on a magnified image and a CSF flow waveform was generated.
During CSF diastole, CSF moves in the caudocranial direction (positive velocity), whereas, during CSF systole, the flow is craniocaudal (negative velocity). The CSF velocity data finally used to calculate the third ventriculostomy CSF stroke volume (net CSF volume inflow and net CSF volume outflow during the cardiac cycle) were obtained from these images. We also calculated the overall flow amplitude (OFA = systolic stroke volume [SSV] plus net diastolic stroke volume [DSV]) and the ratio of the absolute value of these 2 measurements (ratio = DSV/SSV).
To evaluate the reproducibility of the quantification values, some regions of interest were performed twice by the same radiologist, on different occasions, and we determined that no significant differences were observed between the 2 measurements.
Sagittal Technique.
For qualitative assessment of CSF flow, midsagittal contrast images were displayed in closed-loop cine format (Fig 2). The direction of flow encoding was craniocaudal and velocity encoding 10 cm/s. The imaging parameters were as follows: TR, 70 msec; TE, 13 msec; flip angle, 15°; field of view, 250 mm; matrix, 192 × 256; scan thickness, 4 mm. Measurement time was approximately 7 minutes. We evaluated the presence of signal intensity void in the ventriculostomy (at the level of mammillary bodies.)

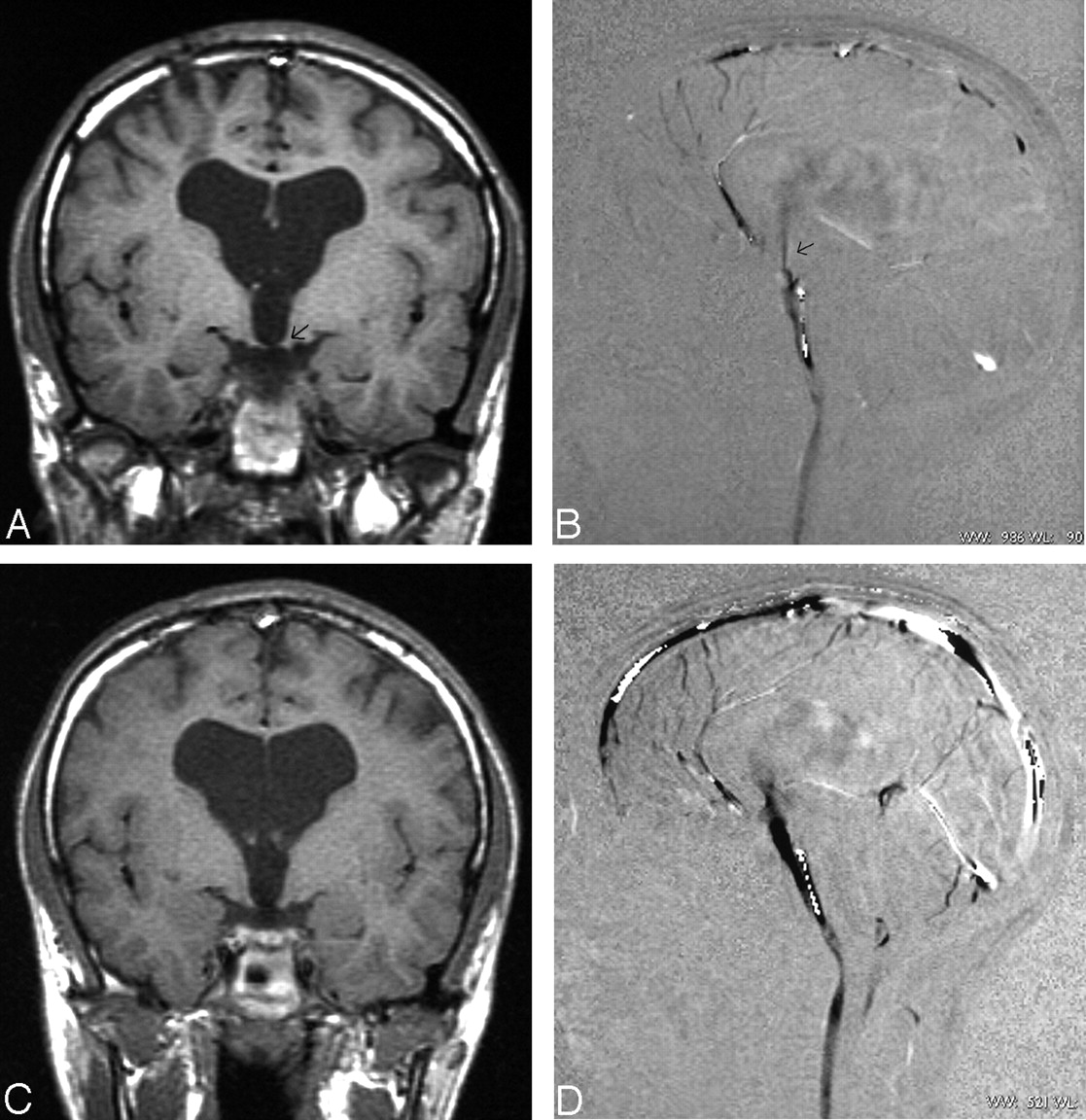
An 11-year-old boy with aqueduct stenosis and previous ventriculostomy who had clinical deterioration. A, Coronal T1-weighted image centering in mammillary bodies shows a small defect in the floor of third ventricle (arrow). B, Sagittal cine phase contrast in the ventriculostomy site demonstrates a filiform flow signal intensity (arrow). C and D, Coronal T1-weighted image and sagittal cine phase contrast after new ventriculostomy demonstrate a big defect in the floor of third ventricle and excellent flow passing through the ventriculostomy.
Some of the follow-up studies were performed in other 1.5T MR scanning equipment (Signa GE, Milwaukee, WI) by using similar parameters and the same velocity encoding. Previous validation between the 2 scans was performed.
Ventricular size was measured in millimeters from MR studies conducted preoperatively and compared with the last postoperative MR studies. The third ventricle diameter was measured at the widest coronal section, and the lateral ventricle was measured at the maximum bifrontal distance obtained, also in the coronal plane.
Clinical data after treatment were collected from chart review and discussion with the neurosurgeons. The patients were evaluated at least 3 months after surgery. Outcome was graded as I (complete resolution of hydrocephalus symptoms), II (partial resolution of the symptoms), III (no improvement), or and IV (worsening of the symptoms).
To evaluate the pattern of CSF circulation a healthy control group, 22 individuals were studied (12 men and 10 women; mean age, 49.36 years) with cine phase-contrast MR imaging. To evaluate aqueductal CSF flow, the MR protocol was the same as described above, but the section thickness of 4 mm was positioned perpendicular to the aqueduct. DSVs and SSVs in the aqueduct were quantified.
Statistical Analysis.
Descriptive statistical analysis was made for qualitative variables (clinical outcome, etiology of hydrocephalus, and ventricular size changes). The quantitative variables obtained in each MR study were DSV, SSV, OFA, and the ratio between diastolic and systolic stroke volume. The Pearson correlation coefficient was used to evaluate the correlation between stroke volume values obtained in the ventriculostomy in patients and those obtained in the aqueduct in the control group. The Spearman correlation coefficient was used to evaluate the stroke volume values obtained in the ventriculostomy with clinical outcome and ventricular changes. The χ2 test was used to evaluate the relation between clinical outcome and ventricular size. To determine a baseline stroke volume value useful to predict the clinical outcome, the receiver operating characteristic analysis (ROC) curve was performed.
Results
Thirty patients showed improvement after third ventriculostomy, 17 patients presented partial improvement, and 13 had complete resolution of the symptoms. Two patients presented initial improvement but progressive worsening of the symptoms, and 6 patients did not improve at all.
By using cine phase-contrast MR imaging of the sagittal plane, in the initial follow-up studies in 36 patients we detected flow void in the ventriculostomy hole (from the floor of the third ventricle body toward basal cisterns). Two patients with communicating hydrocephalus never showed flow void in the follow-up studies, and neither of them improved after surgery. Two patients who initially had flow void in the follow-up studies and clinical improvement in later follow-up studies manifested lack of flow void in the ventriculostomy. One of these patients was an 11-year-old boy with primary aqueduct stenosis who had clinical deterioration, and the ventriculostomy was re-examined, which demonstrated arachnoid septa (Fig 2). The other patient who did not present flow in the ventriculostomy in the later follow-up studies had a pineal tumor compromising the aqueduct. After treatment, the tumor size decreased, the aqueduct became permeable again, and the ventriculostomy flow disappeared (Fig 3).

Patients with secondary aqueduct stenosis induced by pineal lesion. A, Sagittal T1-weighted image demonstrated a cystic lesion in the pineal region blocking the aqueduct and producing hydrocephalus. B, Sagittal cine phase-contrast in the ventriculostomy site performed shortly after surgery and treatment of pineal lesion demonstrates a filiform flow signal intensity in the ventriculostomy and subtle flow signal intensity in the aqueduct (arrows). C, Sagittal T1-weighted image obtained long after treatment demonstrates reduction of pineal lesion and aqueduct decompression. D, Sagittal cine phase-contrast performed in the same examination shows absence of flow in the ventriculostomy and aqueduct permeability.
In 6 patients, we observed reversed flow circulation at the ventriculostomy in the first follow-up study, but in subsequent controls the flow returned to being caudocranial in diastole and craniocaudal in systole.
Fifteen patients (39.5%) of all groups presented a reduction in ventricular size. The relation between clinical outcome and ventricular size changes is described in Table 1.
Clinical outcome related to ventricular size changes
Five of the 13 patients whose symptoms resolved completely (38.5%) and 9 patients of the 17 (52.9%) who had partial improvement showed ventricular size reduction. Patients with secondary aqueduct stenosis showed more ventricular size reduction than the other groups; 66.7% of these patients presented reduction in ventricular size, whereas only 26.7% of patients with primary aqueduct stenosis had ventricular size reduction.
The relation between clinical outcome and hydrocephalus etiology is represented in Table 2. Patients with aqueduct stenosis demonstrated better clinical outcome than patients with Arnold Chiari malformation or communicating hydrocephalus. In fact, 2 of the 6 patients with Arnold Chiari malformation and 2 of the 3 patients with communicating hydrocephalus partially improved after surgery, whereas 10 of the 11 patients with primary aqueduct stenosis (90.9%) showed resolution of symptoms after ventriculostomy.
Relationship between hydrocephalus etiology and clinical outcome
Stroke volume values obtained in the ventriculostomy in the patient group were significantly higher than the stroke volume values registered in the aqueduct in the control group (P > .01). In the control group the median of OFA was 80 mm3, whereas in the patient group the median obtained in the ventriculostomy was 137 mm3.
These results confirm the higher flow of CSF during the cardiac cycle passing through the ventriculostomy than passing through the aqueduct. This result was to be expected, because the diameter of the ventriculostomy was greater than the aqueduct size. We also observed that the stroke volume values were maintained in the follow-up studies.
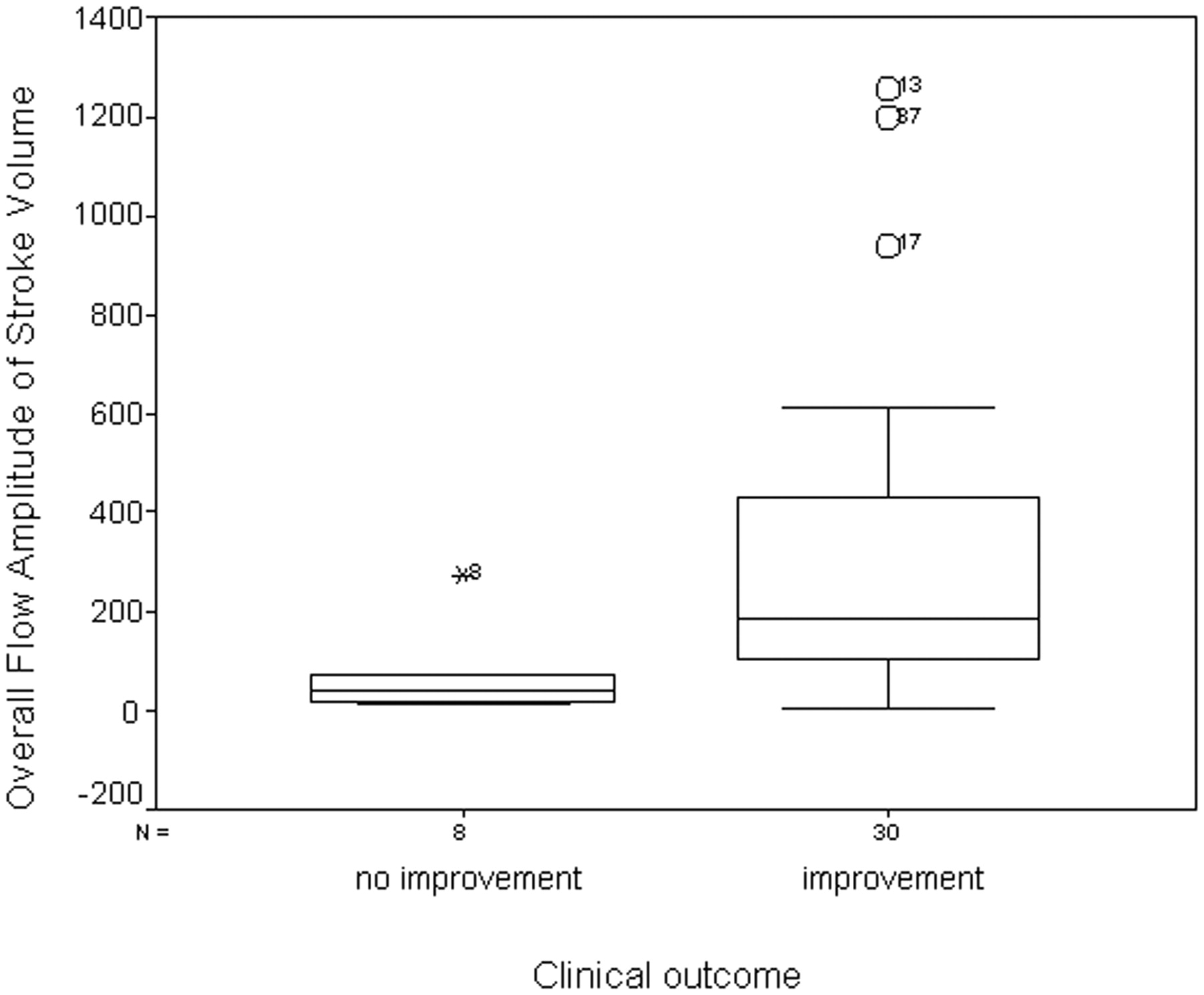
When we compared the stroke volume values between patients with clinical improvement and patients without any clinical changes or worsening of the symptoms, we found that the patients with bad outcome had lower stroke volume values (Fig 4). This finding is statistically significant if we use SSV and DSV and OFA (P > .01). We did not, however, find any differences between patients with total or partial improvement.

Box plot of the OFA of stroke volume related to clinical outcome. Patients with clinical improvement after surgery showed higher stoke volume than patients without clinical improvement.
Comparative ROC curves by using the stroke volume values demonstrated that OFA is a better test than the other variables to predict the response to surgery in the postoperative studies. When OFA value is >75 mm3, the sensitivity and specificity of this technique to determine which patient will improve were 76.7% and 87.5%, respectively, with a positive likelihood ratio of 6.13 and a negative likelihood ratio of 0.27.
Discussion
The indications for ETV are still a matter of controversy. Although the technique has proved to be highly successful in treating occlusive hydrocephalus caused by primary or secondary aqueductal stenosis and space-occupying lesions of the midbrain, the pineal region or the posterior fossa (11–15), it is thought to be less effective in patients with hydrocephalus caused by intraventricular or subarachnoid hemorrhage, in patients with meningitis, in pediatric patients with associated spinal dysraphism and in normal pressure hydrocephalus (1, 2, 5, 12, 16–18). In Chiari type I malformations, the results with ETV reported in the literature vary widely. Although hydrocephalus associated with Chiari type I malformations may be considered obstructive, the reason for the disparity in the results is unknown (5, 18). In our series the only 2 cases with Chiari type I malformation presenting clinical improvement were patients in whom the main cause of hydrocephalus was aqueductal stenosis.
A range of image parameters have been assessed to evaluate the permeability of the ETV, including ventricular size changes, flow void signal intensity, and MR patency, by using cine phase-contrast MR (2–5, 7, 12, 19, 20). MR imaging velocity measurements in the third ventriculostomy have also been evaluated by Lev et al (13).
Ventricular size is not always reduced after third ventriculostomy. The proportion of subjects who did not present ventricular size reduction ranges between 11% and 38% in the series reported to date. In our series, we found a reduction in only 39.5% of the patients, and, on correlating the ventricular size changes with clinical improvement and hydrocephalus etiology, we found that even among patients in whom the symptoms improved completely only 38% had ventricular size reduction. We also found that the patients with secondary aqueductal stenosis caused by tumor compression had the greatest ventricular size reduction. This finding suggests that ventricular size reduction is easier to identify in patients with acute hydrocephalus, whereas in chronic hydrocephalus the ventricular size changes are subtler and in some cases are only perceived when detailed measurements or volumetric studies are performed (2, 20–22). Currently, the consensus is that ventricular size reduction does not seem to correlate with clinical outcome, and, thus, anatomic neuroimaging during follow-up is only useful for ruling out increasing ventricular size.
Numerous investigators have studied flow void as an indicator of ETV patency. Flow void signal intensity in the floor of the third ventricle assessed by MR flow studies is observed in most patients with clinical improvement and indicates evidence of flow through the ETV (3, 16, 23). Some patency of the ETV site, however, has been demonstrated, even in cases deemed clinical failures with an incidence of as high as 50% in some series (24). In our series, 4 patients did not show flow void signal intensity in the floor of the third ventricle in the follow-up sagittal cine phase-contrast MR imaging studies, but the quantitative studies still indicated low values in mean velocity and stroke volume. In one of these patients with primary aqueduct stenosis, the ventriculostomy was examined and arachnoid septa were observed. The other 3 patients were also reevaluated—2 who had communicating hydrocephalus were treated with ventriculoperitoneal shunt, and in the other patient who presented reduction of secondary aqueductal stenosis after radiation therapy we considered that the ventriculostomy was not functioning but the CSF flow in the aqueduct had been restored.
Phase-contrast flow-sensitive MR imaging techniques offer more physiologic data than structural MR images and qualitative assessment of the patency of ventriculostomy. The sagittal acquisition tends to underestimate CSF flow because of intravoxel phase dispersion from in-plane flow, but, by contrast, it produces an easy-to-read cine display. The angle-axial acquisitions perpendicular to the ventriculostomy takes advantage of through-plane flow and is more accurate for quantitative analysis, because the partial volume effects are minimized. Velocity encoding has to be similar or a little higher than 20 cm/s to avoid aliasing artifacts. Although in this study the MR acquisitions were frankly larger, new MR images provide faster hardware that allows performing these studies in <15 minutes. Only patients with severe bradycardia and cardiac arrhythmia have to be excluded, because cardiac cycle registration will be difficult.
Lev et al (13) reported the utility of cine phase-contrast MR velocity measurements in determining the functional status of third ventriculostomy. They examined 6 patients with third ventriculostomy and 12 normal subjects by phase-contrast MR and correlated the quantitative velocity data with clinical follow-up. They concluded that phase-contrast MR velocity measurements, specifically the velocity ratio between the high pontine cistern and the space anterior to the spinal cord, may help to determine the functional status of third ventriculostomy.
In our study, we compared stroke volume measurement in the third ventriculostomy and the aqueduct in a healthy control group and observed that the pattern of the stroke volume was similar, indicating that the cardiac cycle-related pulsated bidirectional CSF motion through the aqueduct in the healthy volunteers is also present in the ventriculostomy orifice. The low resistance provided by the ventriculostomy allows increased CSF pulsation during the cardiac cycle. Stroke volume measurements in the ventriculostomy are expected to be higher than in the aqueduct because the diameter of the ventriculostomy is greater than the aqueduct size. Our results demonstrated these differences between stroke volume in the ventriculostomy and the aqueduct and also the permanency of these high stroke volume values across time in the follow-up studies. We also observed that in some patients the caudocranial flow was higher than the craniocaudal in the first postoperative control but this pattern was reversed in the follow-up studies. After surgery there may be a turbulent flow in the ventriculostomy that progressively returns to normal and this inverted flow pattern in the first postoperative control does not necessarily indicate failure of the ventriculostomy. None of the patients in our series showed worsening or lack of improvement of symptoms.
Of the 6 patients who did not improve after ventriculostomy, 4 had Arnold Chiari malformation and another had communicating hydrocephalus. The lack of success of ventriculostomy in these conditions may not have been due to inefficient surgery technique but rather to erroneous indication. In each case, the stoke volume was low, and, thus, ventriculostomy function was poor because of an insufficient pressure gradient between the third ventricle floor and the basal cisterns. An obstructive intraventricular condition leads to the appearance of a pressure gradient between the ventricular system and the subarachnoid space and the opening between these compartments. This pressure gradient allows the CSF to move forward into the subarachnoid space. Quantitative analysis of the CSF flow in the ventriculostomy in these cases with lack of success indicated that the amount of CSF flow across the fenestration was insufficient to resolve the CSF circulation problem, possibly because of inappropriate treatment in most patients with nonintraventricular obstruction (Fig 5).

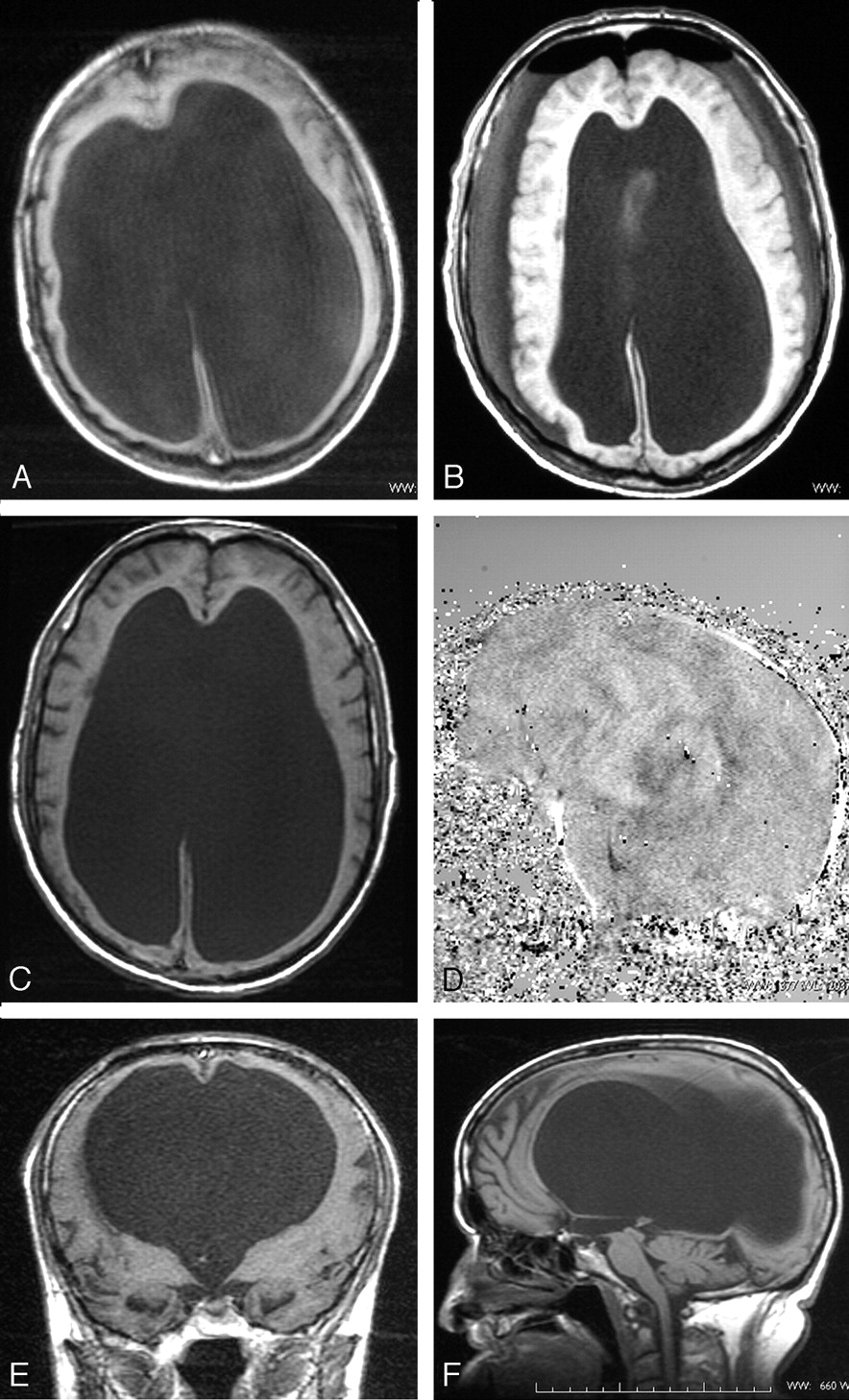
Patient with congenital triventricular hydrocephalus. A, Presurgery axial T1-weighted image at the level of ventricular bodies demonstrated an enlarged ventricular size. B, Immediately postsurgery, axial T1-weighted image at the same level shows reduction of ventricular size and 2 subdural collections. Pneumoencephalus was also present. C and D, Axial T1-weighted image, 6 months after surgery, shows that the ventricular bodies regressed to initial size, and sagittal phase-contrast image demonstrates absence of flow in the ventriculostomy. E and F, Coronal and sagittal T1-weighted image, 6 months after surgery, at the level of mammillary bodies demonstrates the persistence of third floor defect.
An important finding in this study is that, if the OFA of the stroke volume in the initial follow-up study is high (>75 mm3), ventriculostomy is effective and the patient improves. If the value of stroke volume is <75 mm3, further radiologic follow-up is necessary to determine the usefulness of ventriculostomy. We also found that a decrease in stroke volume during the follow-up control was associated with ventriculostomy failure and clinical deterioration.
Conclusion
Endoscopic third ventriculostomy restores the pulsatile bidirectional CSF motion. In addition, the measurement of stroke volume in ventriculostomy by using cine phase-contrast MR imaging provides functional information about the third ventriculostomy. Our results show a good correlation between clinical improvement and stroke volume. When the stroke volume obtained in the ventriculostomy is high, the clinical outcome is usually good and further quantification radiologic study is only needed in the appearance of clinical deterioration. Ventricular size is not a good indicator of ventriculostomy patency. Similar to other authors, we consider ETV to be the best technique for primary and secondary aqueductal stenosis, but not for communicating hydrocephalus.
References
- Received October 29, 2004.
- Accepted after revision February 11, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}