
Abstract
Summary: The imaging findings of cryptococcosis affecting the brain in immunocompetent patients can be different from the more commonly described findings in immunocompromised patients. We report a case of an extremely unusual MR appearance of central nervous system cryptococcosis in a 49-year-old immunocompetent man.
Cryptococcus neoformans is an opportunistic fungal infection that affects the central nervous system in HIV patients and patients in other immunocompromised states. It can infrequently be seen in immunocompetent patients as well (1). Imaging findings of central nervous system infection by Cryptococcus species have been well described in literature. We present a case of an extremely unusual presentation of cryptococcal infection in the brain of an immunocompetent patient.
Case Report
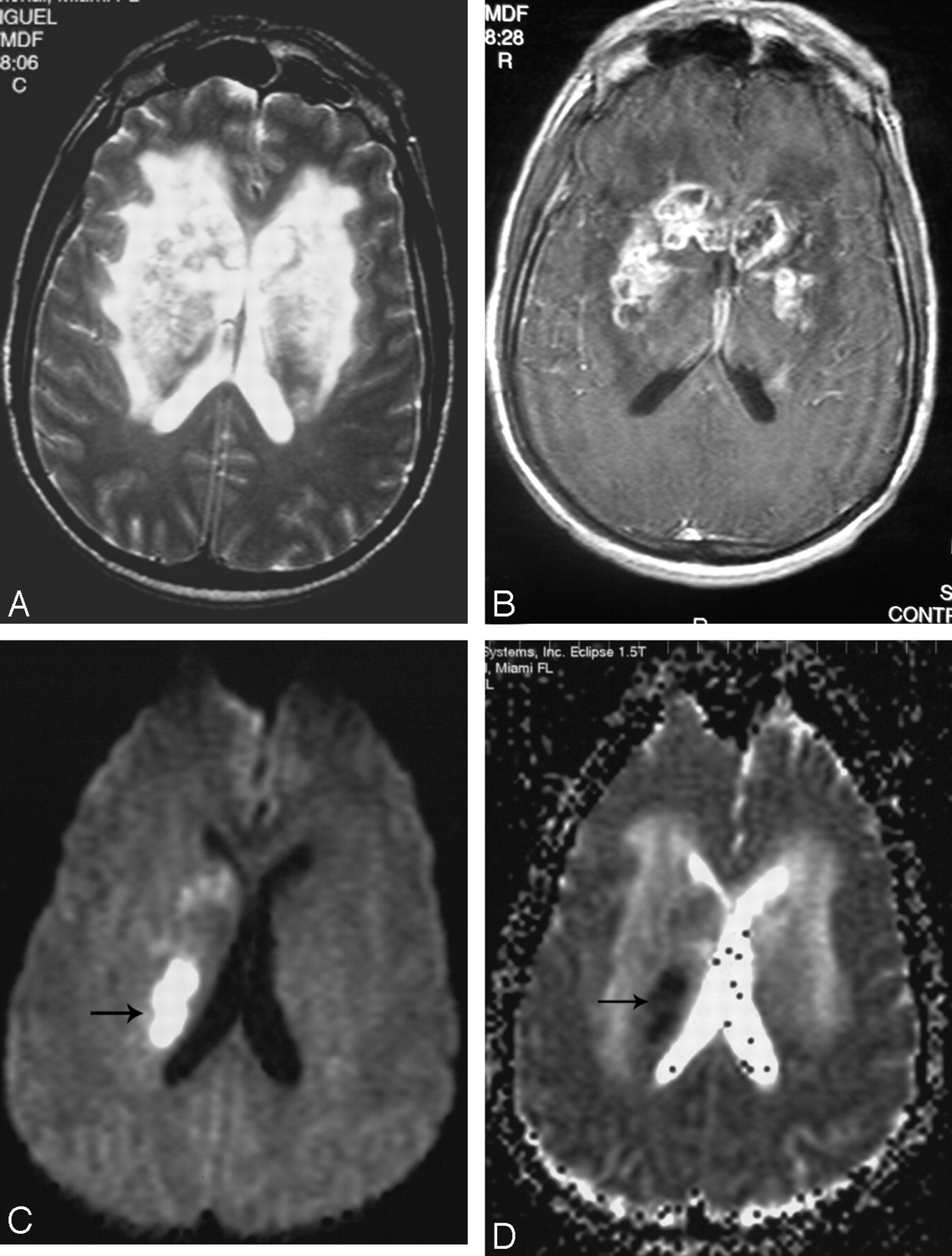
A 49-year-old man presented acutely with a change in mental status, frontal headache, and an episode of syncope. He had been in good health until 1 month earlier, when his wife noticed some “unusual” behavior. The patient was becoming progressively confused, was sleeping most of the time, and was complaining of severe frontal headaches. He had no history of any medical illness and had not undergone surgery. He had been involved in cleaning pigeon droppings form a pigeon coop 1 month before the presentation. The initial MR image (8/6/02) showed small cystlike clusters in the basal ganglia bilaterally (Fig 1). These were hypointense on T1-weighted and hyperintense on FLAIR/T2-weighted images and showed subtle postcontrast enhancement. Some of the cysts demonstrated restricted diffusion, and an initial diagnosis of ischemia was suggested. No other lesions were seen in the brain. MR angiography did not show any abnormality in the vasculature. No meningeal enhancement was noted.

Axial T2-weighted (A) and contrast-enhanced T1-weighted (B) MR images demonstrate a cluster of small hyperintense T2-weighted lesions in the basal ganglia (arrows), showing subtle peripheral enhancement. Diffusion-weighted image (C) demonstrates high signal intensity in some of the lesions (arrow).
Findings of a lumbar puncture procedure showed an opening pressure of >35 cm of H2O. CSF was clear. Laboratory studies disclosed the following values: RBC, 12; WBC, 87 with 95% lymphocytes; CSF glucose, 22; total protein, 85; CSF IgG, 9.32 mg/dL; albumin, 42.10 g/dL, with an increased CSF index of 1.45 and positive oligoclonal bands. The results of the Gram stain and acid fast bacilli stain were normal. India ink showed encapsulated yeast, and the findings of a culture showed a light growth of C neoformans (Fig. 2). Cryptococcal antigen titer was 1:256. Findings of serum HIV and human T-cell lymphoma/leukemia virus tests were negative with normal T-cell subsets. Thyroid functions were normal. Antinuclear antibody levels, complement levels, and B12, and folate levels were normal.

India ink preparation of CSF (A) demonstrates encapsulated yeast. CSF mycology culture (B) shows a light growth of Cryptococcus neoformans.
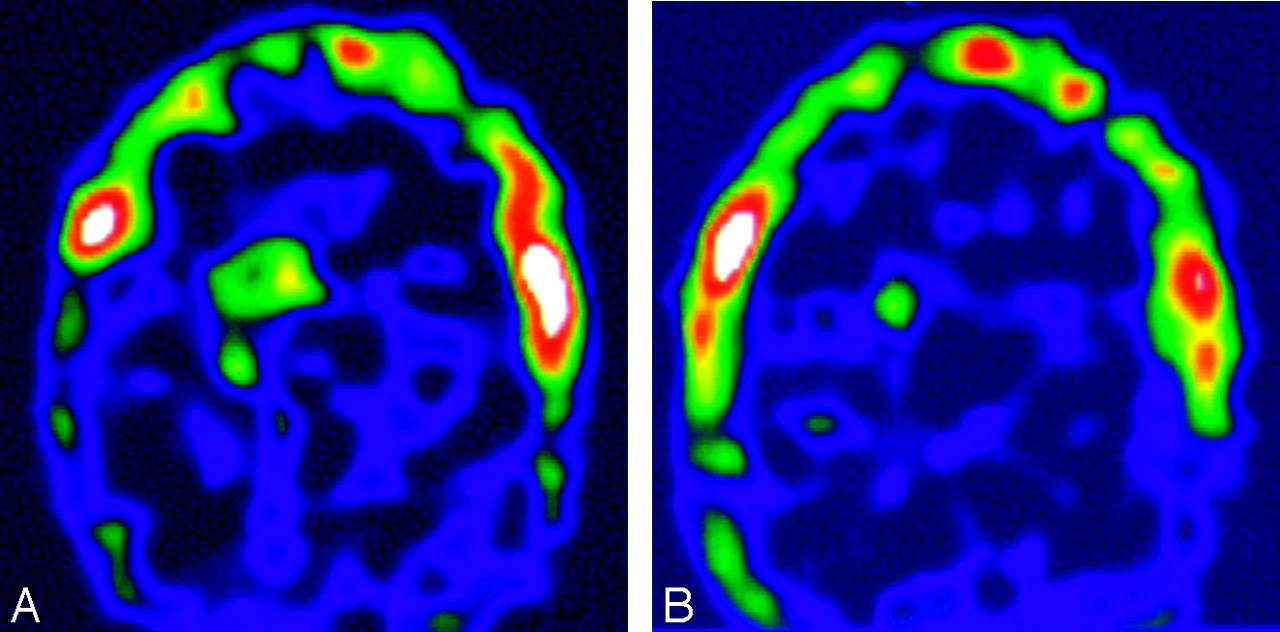
Following the lumbar puncture result, the diagnosis of cryptococcal meningitis with early gelatinous pseudocyst formation in the perivascular spaces was established, and the patient was started on IV amphotericin therapy for 2 months, following which the patient was discharged on oral amphotericin. The cryptococcal antigen titer was normal at the time of discharge. The patient returned a few days later with a worsening of mental status, and repeat MR imaging was performed (10/31/02), which revealed marked enlargement of the gelatinous pseudocysts in the basal ganglia, showing peripheral postcontrast enhancement and marked surrounding edema (Fig 3). The restricted diffusion seen in the previous lesions had resolved, and new areas of restricted diffusion were noted. The cryptococcal antigen titer was elevated at 1:64. A thallium–single-photon emission tomography study was also performed (11/18/02), which showed marked increased uptake in the basal ganglia (Fig 4A).

On axial T2-weighted (A) and contrast-enhanced (B) MR images, repeat MR imaging shows marked enlargement of the previously noted cystic lesions in the basal ganglia and florid peripheral postcontrast enhancement of the lesions. New areas of restricted diffusion are seen on the diffusion-weighted (C) and the apparent diffusion coefficient map (D) images, which are different in location from those seen before.

A, Initial thallium–single-photon emission tomography image demonstrates marked uptake in the basal ganglia bilaterally. B, Posttreatment, note near complete reduction of uptake.
At this time, on the basis of the thallium–single-photon emission tomography findings, the possibility of a neoplastic process such as a lymphoma was also entertained. Because no clinical improvement had been seen up to this stage, double drug therapy with flucytosine and fluconazole was instituted. After discussion with the neurology service, steroids were also added to the therapy regimen because of the intense inflammatory response. Repeat MR imaging (11/26/02) demonstrated a significant decrease in the T2/FLAIR signal intensity abnormality in the basal ganglia bilaterally, suggestive of resolving edema. The number of cysts and postcontrast enhancement also showed interval reduction. Repeat thallium–single-photon emission tomography (12/04/02) demonstrated marked reduction in uptake in the basal ganglia with near complete resolution (Fig 4B). Cryptococcal antigen titers were normal at this time (12/30/02). Steroid therapy was tapered and a repeat thallium–single-photon emission tomography study (01/07/03) showed no uptake of radiotracer in the basal ganglia, suggesting resolution.
Multiple repeat MR imaging studies during the next 2 years showed eventual resolution of the edema, the development of calcification, and gliosis and marked reduction in the size of the small residual peripherally enhancing lesions (Fig. 5). The patient was doing well clinically at the time of the last MR imaging 2 years after the initial presentation. Findings of his CSF cryptococcal antigen test remained negative.

Axial T1-weighted (A) and postcontrast T1-weighted (B) images demonstrate T1 hyperintensity in the basal ganglia, suggestive of calcification. Some residual enhancement persists on the postcontrast images.
Discussion
C neoformans is a ubiquitous organism found in mammal and bird feces, particularly in pigeon droppings (2). Cryptococcosis is an opportunistic fungal infection that affects the central nervous system in HIV and other immunocompromised patients. It can rarely be seen in immunocompetent patients as well (1). Headache is the most common symptom, but patients may also present with meningeal signs, confusion, seizures, blurred vision, and, rarely, focal deficits. Fever and nuchal rigidity may be mild or absent (3). Lumbar puncture is a useful initial diagnostic test that shows increased CSF pressure and may show mild-to-moderate leukocytosis, decreased glucose levels, and elevated protein levels. The India ink test is more specific and helps in demonstrating the fungus. The level of antigen titer corresponds to the severity of disease (4).
Besides the immune status of the patient, the size of the inoculum is considered to be an important factor in determining the pathogenesis of this disease (2). We postulate that our patient inhaled a huge bolus of cryptococcal organisms while cleaning the pigeon coop, which could explain the cause of the infection in this immunocompetent patient via the respiratory route, which is the major route of dissemination of this organism. Central nervous system infection can be either meningeal or parenchymal. Infection usually starts as meningitis. Parenchymal involvement is seen as cryptococcomas (also known as toruloma), dilated Virchow-Robin spaces, or enhancing cortical nodules (5). It is believed that the meningeal infection along the base of the skull may involve the adjacent brain parenchyma, giving rise to cryptococcomas (6) or may extend along the Virchow-Robin spaces. Virchow-Robin spaces are perivascular spaces seen accompanying the lenticulostriate, perforating branches of the middle cerebral arteries in the basal ganglia. Perivascular spaces are also seen in the thalamus, periventricular white matter, midbrain, and the cerebellum (7). As the infection spreads along the Virchow-Robin spaces, the perivascular spaces may dilate with mucoid gelatinous material produced by the capsule of the organism (4, 5, 8). These cysts have, therefore, also been called “gelatinous pseudocysts” (5).
Imaging tests may provide useful diagnostic information (although the findings are not pathognomonic and other infectious processes may simulate cryptococcal infection in the brain). A communicating hydrocephalus may occur because of the acute meningeal exudate and also may occur late in the course of the infection because of meningeal adhesions. Gelatinous pseudocysts are seen as multiple CSF-equivalent round or oval cysts in the basal ganglia, thalami, midbrain, cerebellum, and the periventricular regions. On MR imaging, these are seen as multiple hypointense T1 and hyperintense T2 lesions (Fig 1). Demonstration of clusters of these cysts in the basal ganglia and thalami is fairly specific and strongly suggestive of this infection (5, 8). Enhancement of these lesions usually does not occur for 2 reasons. Firstly, these lesions are perivascular and therefore do not usually penetrate the blood-brain barrier for contrast enhancement to occur. Secondly, as mentioned earlier, these lesions are most commonly seen in immunocompromised patients who are unable to mount an immune response to the infection. In rare instances when the infection affects an immunocompetent patient, enhancement of these lesions might occur as a result of an immunologic reaction by the host (1). We speculate a similar pathogenesis wherein the intact immune status of our patient resulted in an intense inflammatory response, leading to marked enhancement and the surrounding edema of the lesions.
Concerning uptake on thallium–single-photon emission tomography imaging, we note that there have been reports of false-positive thallium–single-photon emission tomography uptake in patients with bacterial brain abscess and fungal (Candida and Aspergillus organisms) brain abscess (9). Tonami et al (10) postulated that an intense inflammatory response with marked endothelial proliferation and increased permeability of the blood-brain barrier led to the increased uptake of thallium, similar to the increased blood-brain barrier permeability, increased vascularity, and increased metabolic cellular activity that have been proposed as a possible mechanism for increased thallium uptake in tumors.
We postulate in our case of an overwhelming acute cryptococcal infection in an immunocompetent host that the patient was able (because of his intact immune system) to mount an intense inflammatory response that resulted in marked endothelial proliferation and increased permeability of the blood-brain barrier, with resultant intense contrast enhancement and edema due to leakage of contrast material and water out of an altered blood-brain barrier. This inflammatory response then accounted for the increased uptake of thallium on the earlier thallium scans and a subsequent decrease and eventual resolution of this thallium uptake with the addition of multidrug antifungal therapy. The addition of steroid therapy also helped to improve the patient’s course, providing the medication to ameliorate this intense inflammatory response during the early stages of the infection. We postulate that by decreasing the junction between the endothelial cells, the steroids (which were tapered and then discontinued) prevented less permeability of the blood-brain barrier, decreasing passage of contrast material and the interstitial edema. As for the restricted diffusion found on our patient’s MR images, fluid restriction can be explained by reviewing the literature. Restricted diffusion in bacterial abscesses is a well-known phenomenon and is thought to be due to the high cellularity and viscosity of its pus content (11). Similarly, the high viscosity of the thick gelatinous content of the cryptococcal pseudocysts likely explains the restricted diffusion seen in our case and its eventual resolution.
It has been recommended that longer duration of treatment and combination therapy with multiple antifungal agents might be needed not only in HIV-infected and resistant cases but also in infected immunocompetent patients (2). The relatively long duration and the use of multiple antifungal agents such as amphotericin B, flucytosine, and fluconazole required to treat the infection in our patient support this recommendation.
In conclusion, the appearance of a Cryptococcus central nervous system infection in an immunocompetent patient may be different from that commonly encountered in the immunocompromised. Cryptococcosis should be considered in the differential when multiple cystic lesions are noted in the basal ganglia, even in an immunocompetent patient. Marked ring enhancement of the basal ganglia lesions may be seen; this enhancement probably represents the patient’s ability to mount an immune response, which would be uncommon in an immunocompromised patient. Marked surrounding edema may also be a feature of this infection. An interesting finding seen in this patient was the changing patterns of restricted diffusion in the lesions (findings somewhat similar to those seen in other infections with different stages of evolution) and the increased uptake on the thallium–single-photon emission tomography imaging.
References
- Received November 6, 2004.
- Accepted after revision January 19, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- CNS-Immune Reconstitution Inflammatory Syndrome in the Setting of HIV Infection, Part 1: Overview and Discussion of Progressive Multifocal Leukoencephalopathy-Immune Reconstitution Inflammatory Syndrome and Cryptococcal-Immune Reconstitution Inflammatory Syndrome
- Uncommon Presentation of Intracranial Cryptococcoma in an Immunocompetent Patient
- Reply: