
Abstract
BACKGROUND AND PURPOSE: The purpose of this study was to assess the incidence of early rebleeding after coiling of a ruptured cerebral aneurysm, assess the clinical outcome, and identify risk factors for this event.
METHODS: Early rebleedings occurred in 6/431 (1.4%) consecutive patients after coiling of a ruptured aneurysm. Clinical condition at the time of treatment, aneurysm location and size, initial aneurysm occlusion, timing of coiling, and the presence of an adjacent intracerebral hematoma in the six patients with early rebleedings were compared with the remaining 425 patients.
RESULTS: Incidence of early rebleeding after coiling of a ruptured aneurysm was 1.4%, and mortality was 100%. Independent risk factors are the presence of an adjacent intracerebral hematoma and small aneurysm size. Dependant risk factors are location on the anterior communicating artery, initial incomplete aneurysm occlusion, and poor clinical condition at the time of treatment.
CONCLUSION: Early rebleeding after coiling of ruptured aneurysms is a major concern, in particular because the mortality is very high. A more restricted postembolization anticoagulation strategy in high-risk aneurysms may possibly prevent the occurrence of this devastating event.
Surgical or endovascular treatment of ruptured cerebral aneurysms is aimed at the prevention of rebleedings with the lowest possible risk of procedural complications. Because the risk of rebleeding is highest in the first hours and days after subarachnoid hemorrhage (SAH), early treatment is advocated. It is generally assumed that both surgery and coiling are effective in preventing early rebleedings (1–4). We reviewed our data base of 431 consecutive patients who, over an 8-year period, were treated with coils for ruptured aneurysms. We assessed the incidences of early rebleeding after coiling of a ruptured cerebral aneurysm, evaluated the clinical outcomes, and tried to identify risk factors for this event.
Clinical Material and Methods
Between November 1994 and April 2003, 431 consecutive patients with ruptured aneurysms were treated with Guglielmi detachable coils (Boston Scientific, Fremont, CA) or Detach coils (Cook, Copenhagen, Denmark). The patient group included 301 women and 130 men, with a mean age of 52.2 years (median, 52 years; range, 25–81 years). At the time of treatment, the clinical condition of the patients was graded according to the Hunt and Hess (HH) scale (5) as follows: HH I–II, 273; HH III, 86; HH IV–V, 72. The mean delay between SAH and treatment with coils was 9.1 days (median, 5 days; range, 0–80 days). Treated aneurysms were located in the following areas: anterior communicating artery, 138; basilar bifurcation, 91; posterior communicating artery, 75; middle cerebral artery, 28; pericallosal artery, 18; superior cerebellar artery, 15; posterior inferior cerebellar artery, 15; carotid bifurcation, 13; anterior choroidal artery, 8; basilar trunk, 8; ophthalmic artery, 8; vertebral artery, 6; posterior cerebral artery, 6; and supraclinoid carotid artery, 2. CT scanning on admission revealed an adjacent intracerebral hematoma in 63 patients.
Coiling of aneurysms was performed with the patient under general anesthesia and systemic heparinization. The aim of the coiling was to obtain a packing of the aneurysm as attenuated as possible. Heparin was continued intravenously or subcutaneously for 48 hours after the procedure, followed by oral administration of low-dose aspirin for 3 months.
Early rebleeding was separately defined for patients in good clinical condition and for patients in poor clinical condition. Patients in good clinical condition were considered to have had an early rebleeding when a sudden clinical detoriation occurred within 30 days after coiling, together with a rebleeding on CT scan compared with a pre-embolization CT scan. For patients in poor clinical condition after coiling, early rebleeding was diagnosed only if CT scanning revealed more blood than was seen in a previous postembolization CT scan. This last criterion was used to exclude rebleeding between the pre-embolization CT and coiling or unrecognized rebleeding during coiling. On the basis of these criteria, we identified six of 431 patients with early rebleeding from the coiled aneurysm. Three poor-grade patients with more blood on CT scan after coiling compared with the pre-embolization CT were not included, because comparable postembolization CT scans were not available. Early rebleeding after coiling was uncertain in these three patients. Clinical and imaging records were reviewed to identify causative factors that could have contributed to the occurrence of the rebleeding.
Odds ratios (ORs) of early rebleeding with corresponding 95% confidence intervals (CIs) were calculated for the following clinical and aneurysm characteristics: timing of treatment after SAH < median 5 days, aneurysm size <6 mm, presence of an adjacent hematoma on initial CT scanning, aneurysm location on anterior or posterior communicating artery, clinical condition graded as HH III–V at the time of treatment, and initial incomplete occlusion of the aneurysm on the postembolization angiogram.
Statistical analysis was performed by using univariate and multivariate logistic regression (MedCalc Statistical Software, Mariakerke, Belgium). P values <.05 were considered statistically significant.
Our institutional review board did not require its approval or patient informed consent for this study.
Results
The incidence of early rebleeding of ruptured aneurysms was 1.4% (6/431; 95% CI, 0.57–3.09).
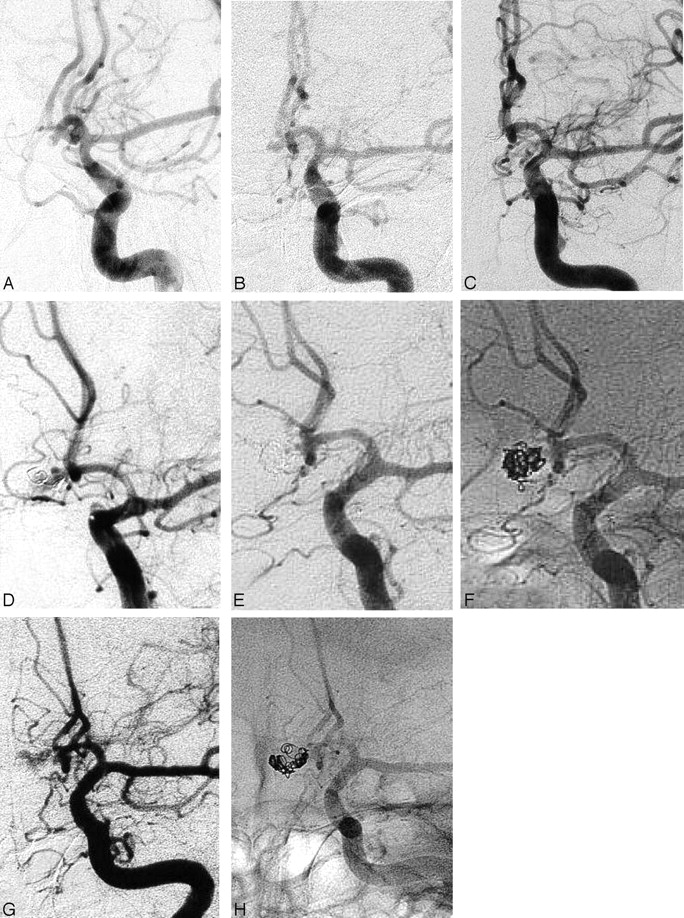
Relevant clinical and imaging data of the six patients with early rebleeding from the coiled aneurysm are summarized in Table 1. In two patients (3 and 5), angiography was performed after the rebleeding. Patient 3, a 34-year-old woman, had a 4-mm ruptured posterior communicating artery aneurysm with an adjacent intracerebral hematoma in the temporal lobe. The aneurysm was initially completely occluded, but she suffered a rebleeding 4 days later. Angiography showed an enlargement of the aneurysm from 4 mm to 5 mm with partial reopening of the aneurysm lumen, possibly as a result of resolution of intraluminal thrombus. Patient 5, a 53-year-old man in poor clinical condition after rupture of a 3-mm anterior communicating artery aneurysm with a large intracerebral hematoma, suffered two rebleedings, one after initial coiling and the other after second coiling (Fig. 1). It is not clear whether the recurrent enlargement of the aneurysm lumen in this patient was caused by resolution of thrombus within a pre-existent larger aneurysm or by resolution of thrombus in an adjacent pseudoaneurysm in the hematoma. All six patients with early rebleeding eventually died.

Serial angiograms of patient 5, a 53-year-old man in poor clinical condition after SAH.
A, Diagnostic angiogram 1 day after SAH, showing a very small aneurysm on the anterior communicating artery with a filling defect (thrombus) in the fundus. The aneurysm was judged to be too small for coil treatment.
B, Angiogram 11 days later, showing disappearance of the fundal thrombus and enlargement of the aneurysm lumen.
C, Complete occlusion after coiling.
D, Angiogram after rebleeding 10 days after coiling, showing further enlargement of the aneurysm lumen with migration of the coils resulting in incomplete aneurysm occlusion.
E and F, Subtracted (E) and unsubtracted (F) angiogram after second coiling, showing near-total occlusion.
G and H, Subtracted (G) and unsubtracted (H) angiogram after second rebleeding 25 days after second coiling, again showing further enlargement of the aneurysm with migration of the coils.
Relevant patient and aneurysm characteristics of the six patients who suffered an early rebleeding after coiling of a ruptured aneurysm
Multiple univariate logistic regression analysis identified aneurysm size <6 mm, aneurysm location on anterior communicating artery, adjacent hematoma on admission CT scan, initial incomplete aneurysm occlusion, and poor clinical condition (HH III–V) as risk factors for early rebleeding (Table 2).
Results of possible risk factors for early rebleeding after coiling of a ruptured aneurysm by multiple univariate logistic regression analysis
Multivariate logistic regression analysis identified aneurysm size <6 mm (OR, 13.7; 95% CI, 1.2–152.3), and adjacent hematoma (OR, 21.3; 95% CI, 1.9–240.2) as independent risk factors for early rebleeding.
Discussion
We found an incidence of 1.4% of early rebleeding after coiling of ruptured aneurysms. Risk factors for this event were aneurysm size <6 mm, the presence of an adjacent intracerebral hematoma on initial CT scanning, location on anterior communicating artery, initial incomplete aneurysm occlusion, and poor clinical condition at the time of treatment. Aneurysm size <6 mm and the presence of an adjacent intracerebral hematoma on initial CT scanning were independent risk factors.
The 1.4% incidence of early rebleeding after coiling is in concordance with reported incidence rates in two prospective studies. Vanninen et al found one fatal early rebleeding in 52 coiled patients (4). In the International Subarachnoid Aneurysm Trial (ISAT; 2), 10 of 1005 coiled aneurysms rebled within 30 days after coiling. Seven of these 10 aneurysms were incompletely occluded, and three were judged to be completely occluded.
Although an early rebleeding rate after coiling of a ruptured aneurysm of 1%–2% may seem low, the high mortality makes this event a major concern. Although rebleeding has an a priori high mortality, clinical consequences may be aggravated by the use of anticoagulant drugs that are usually administered to patients after coiling to prevent thromboembolic complications. Mortality as a consequence of early rebleeding in coiled aneurysms is probably clinically more important than mortality of late rebleeding, which has been reported to be <0.2% annually (3, 6).
Intuitively, incomplete aneurysm occlusion after coiling would be a logical reason for early rebleeding. Although this was a risk factor in our study, it is remarkable that the presence of an adjacent intracerebral hematoma on CT scan was the strongest risk factor for the occurrence of early rebleeding. Even location on anterior communicating artery and aneurysm size <6 mm were stronger risk factors than incomplete aneurysm occlusion.
Why would the presence of an adjacent hematoma be such a strong and independent risk factor for the occurrence of early rebleeding? It is likely that ruptured aneurysms with an adjacent intracerebral hematoma more often harbor a pseudoaneurysm than do aneurysms that have bled solely into the subarachnoid space. Pseudoaneurysms may go undetected on initial angiography, because of thrombosis of the lumen (7–9). Resolution of thrombus over time results in an apparent enlargement of the aneurysm on angiography (Fig 2B and C). At the time of coiling a pseudoaneurysm may or may not be visible on angiography. If a pseudoaneurysm is apparent on angiography, coiling of the true aneurysm plus the pseudoaneurysm can be considered; however, the fragile wall of the pseudoaneurysm is prone to perforation, and this has led some authors to advise against catheterizing the false lumen (7). In our patient 2, we decided to occlude only the true aneurysm and not the pseudoaneurysm, but apparently this did not protect the aneurysm from rebleeding (Fig 2). If the pseudoaneurysm is thrombosed and not visible on angiography at the time of coiling, the false lumen will not be occluded with coils. When reopening occurs in the days following coiling, the coil mesh may migrate into the pseudoaneurysm, resulting in reopening of the aneurysm and possible subsequent rebleeding. This limited angiographic visibility also applies to aneurysms with a lumen that is partially thrombosed shortly after rupture. If only the angiographically visible part of the lumen is filled with coils, subsequent thrombus resolution can lead to reopening of the true aneurysm lumen. This phenomenon of transient partial thrombosis of the aneurysmal lumen after rupture leads to undersizing of the aneurysm and may explain the fact that small aneurysm size is an independent risk factor for the occurrence of early rebleeding.

Patient 2, a 68-year-old man with HH III SAH.
A, CT scan on admission shows small interhemispheric hematoma.
B, Angiogram on the day of admission shows small anterior communicating artery aneurysm pointing upward.
C, Pre-embolization angiogram 6 days later shows enlargement of the aneurysm thought to be caused by pseudoaneurysm formation. Note vasospasm in anterior and middle cerebral artery.
D—F, Lateral views before (D) and after (E and F) coiling, demonstrating a small neck remnant. There are no coils in the pseudoaneurysm. Note stasis of contrast agent in the pseudoaneurysm (F).
G and H, CT scan 16 days later, showing rebleeding and hydocephalus.
Dependent risk factors for early rebleeding are location on the anterior communicating artery and poor clinical condition of the patient at the time of treatment. A possible explanation is that rupture of an anterior communicating artery aneurysm more often is associated with the occurrence of an intracerebral hematoma and that patients with an intracerebral hematoma more often are in poor clinical condition. Also middle cerebral artery aneurysms are associated with intracerebral hematomas, but the proportion of coiled aneurysm on this location is usually small, in our series 6.5% (28 of 431).
How can early rebleedings after coiling of ruptured aneurysms be prevented? Patients with a small ruptured aneurysm and an adjacent hematoma could be offered surgical clipping instead of endovascular treatment. On the other hand, many of these patients are poor surgical candidates because of poor clinical condition. Another possibility of preventing early rebleeding is very early imaging follow-up after coiling for timely detection reopening of the true (pseudo) aneurysm lumen, but this would imply daily angiograms. Theoretically, it may be beneficial to refrain from postprocedural anticoagulation after coiling of a ruptured small aneurysm with an adjacent hematoma: formation of thrombus in the (pseudo) aneurysm is not inhibited and sequelae of a rebleeding could be less devastating.
Conclusion
Early rebleeding after coiling of ruptured aneurysms is a major concern, in particular because the mortality is very high. Risk factors for early rebleeding are adjacent hematoma on initial CT scan and small aneurysm size. It is possible that a more restricted postembolization anticoagulation strategy in high-risk aneurysms may prevent the occurrence of this devastating event.
References
- Received November 11, 2004.
- Accepted after revision January 10, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Safety and efficacy of management for intraprocedural rupture during endovascular treatment for intracranial aneurysms
- Republished:Delayed aneurysm rupture following treatment with the WEB embolization device
- Delayed aneurysm rupture following treatment with the WEB embolization device
- Rebleeding and bleeding in the year following intracranial aneurysm coiling: analysis of a large prospective multicenter cohort of 1140 patients--Analysis of Recanalization after Endovascular Treatment of Intracranial Aneurysm (ARETA) Study
- Stent-assisted coil embolization of anterior communicating artery aneurysms: safety, effectiveness, and risk factors for procedural complications or recanalization
- 'Plug and pipe strategy for treatment of ruptured intracranial aneurysms
- Validity of the Meyer Scale for Assessment of Coiled Aneurysms and Aneurysm Recurrence
- Rupture of aneurysms in the immediate post-coiling period
- Complex shaped detachable platinum coil system for the treatment of cerebral aneurysms: The Codman Trufill DCS and Trufill DCS Orbit Detachable Coil System COMPLEX Registry final results
- Computerized Occlusion Rating: A Superior Predictor of Aneurysm Rebleeding for Ruptured Embolized Aneurysms
- Single-Center Experience of Surgical and Endovascular Treatment of Ruptured Intracranial Aneurysms
- Reporting standards for endovascular repair of saccular intracranial cerebral aneurysms
- Late Adverse Events in Coiled Ruptured Aneurysms with Incomplete Occlusion at 6-Month Angiographic Follow-Up
- Reporting Standards for Endovascular Repair of Saccular Intracranial Cerebral Aneurysms
- Reporting Standards for Endovascular Repair of Saccular Intracranial Cerebral Aneurysms
- Long-Term Recurrent Subarachnoid Hemorrhage After Adequate Coiling Versus Clipping of Ruptured Intracranial Aneurysms
- Clinical and Angiographic Follow-up of Ruptured Intracranial Aneurysms Treated with Endovascular Embolization
- Clinical and Angiographic Results of Coiling of 196 Very Small (<= 3 mm) Intracranial Aneurysms
- Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage: A Statement for Healthcare Professionals From a Special Writing Group of the Stroke Council, American Heart Association