
Abstract
BACKGROUND AND PURPOSE: A report directly comparing platinum coils, Matrix coils, and HydroCoils in a single animal model does not currently exist. We evaluated and compared the performance of these three products in the embolization of experimental aneurysms.
METHODS: Thirty-three elastase-induced saccular aneurysms were created in rabbits. Aneurysms were embolized with Matrix coils (n = 15), HydroCoils (n = 9), or platinum coils (n = 9). The groups were compared with respect to the following parameters: aneurysm size, procedure duration, number and total length of devices deposited, angiographic occlusion score, and volumetric occlusion percentage. Follow-up angiographic and histologic features at 2, 6, and 10 weeks after embolization were analyzed. Groups were compared by using analysis of variance and χ2 tests.
RESULTS: No significant differences were found among groups regarding aneurysm size, total device length, initial angiographic occlusion score, or procedure time. The mean number of devices for Matrix subjects was less than that for platinum coils (P = .02) and HydroCoil (P = .03). Volumetric occlusion for HydroCoil (76%) was significantly greater (P < .0001) than both platinum coils (31%) and Matrix (23%). Angiographic durability was significantly increased in the HydroCoil group compared with Matrix (P = .03). Coil compaction was found more frequently in the Matrix group (five cases, 33%) than the HydroCoil (no cases, 0%), or platinum coil groups (two cases, 22%). The Matrix group showed greater tissue reaction compared with platinum coils (P < .05).
CONCLUSION: In the rabbit model, the use of HydroCoils results in improved long-term occlusion rates compared with Matrix and platinum coils. The Matrix group showed an increase in inflammation and coil compaction compared with HydroCoils and platinum coils.
Endovascular treatment of intracranial aneurysms with detachable coils has been widely used as an important alternative to surgical clipping (1, 2); however, coil compaction and aneurysm recanalization remains problematic, especially for giant and wide-necked aneurysms (3–6). Histopathologic results in human specimens show that aneurysms embolized with detachable coils were mainly occupied by unorganized thrombus and lack of neointima across the aneurysm neck in most cases (7). Thus, much attention has been paid to increasing the filling volume of microcoils and accelerating the process of thrombus organization and fibrosis (8–17).
HydroCoil embolization system (MicroVention, Aliso Viejo, CA) and Matrix coils (Boston Scientific, Natick, MA) represent two next-generation microcoils that might lower recurrence rates as compared with platinum coils. The HydroCoil carries an expandable polymer that allows improved aneurysm filling as compared with standard microcoils. The Matrix coil carries a biodegradable polymer that was designed to amplify tissue response to the coil, with a resultant increase in healing.
Separate preclinical animal studies regarding HydroCoil and Matrix have been reported (15, 16), but a report comparing the angiographic and histologic effects in the same aneurysm model does not exist. In this study, we compare angiographic and histologic outcomes among HydroCoils, platinum coils, and Matrix coils in elastase-induced aneurysms in a single study in rabbits.
Methods
Elastase-induced, saccular aneurysms were created in 33 New Zealand white rabbits. The institutional animal care and use committee at our institution approved all procedures. Following aneurysm creation, at least 21 days elapsed before embolization, as previous studies have recommended (19). Embolization was performed with HydroCoil (n = 9), Matrix (n = 15), or platinum coil (n = 9) devices. After embolization, subjects were followed for 2 weeks (n = 11), 6 weeks (n = 11), and 10 weeks (n = 11).
Aneurysm Creation
Detailed procedures for aneurysm creation have been described elsewhere (18). In brief, anesthesia was induced with an intramuscular injection of ketamine, xylazine, and acepromazine (75 mg/kg, 5 mg/kg, and 1 mg/kg, respectively). By using a sterile technique, the right common carotid artery (RCCA) was exposed and ligated distally. A 1–2-mm beveled arteriotomy was made and a 5F vascular sheath (Cordis Endovascular, Miami Lakes, FL) was advanced retrograde in the RCCA to a point approximately 3 cm cephalad to the origin of RCCA. A roadmap image was obtained by injection of contrast through the sheath retrograde in the RCCA, to identify the junction between the RCCA and the subclavian and brachiocephalic arteries (Advantx; General Electric Company; Milwaukee, WI). A 3F Fogarty balloon (Baxter Healthcare, Irvine, CA) was advanced through the sheath to the level of the origin of the RCCA with fluoroscopic guidance and was inflated with iodinated contrast material. Porcine elastase (5.23 μ/mgP, 40.1 mgP/mL, approximately 200 U/mL; Worthington Biochemical, Lakewood, NJ) was incubated within the lumen of the common carotid above the inflated balloon for 20 minutes, after which the catheter, balloon, and sheath were removed, the RCCA was ligated below the sheath entry site.
Description of Embolic Devices
Platinum coil devices.
A variety of sizes (2–8 mm) and lengths (4–19 cm) of the commercially available MicroPlex coiling system (MCS, MicroVention) 0.010-inch and 0.018-inch complex and filler coils were used in this study.
HydroCoil devices.
A variety of sizes (2–4 mm) and lengths (3–10 cm) of commercially available HydroCoil 14 embolic system devices were used in this study. An MCS complex coil (MicroVention) was deployed first to provide framing of the aneurysm sac.
Matrix devices.
A variety of sizes (2–9 mm) and lengths (2–30 cm) of commercially available two-dimensional (2D) Matrix coils were used in this study. The aneurysm sac in Matrix-treated aneurysms was not framed with a complex or 3D platinum coil.
Embolization Procedures
Five aneurysms were used at each time point (2, 6, and 10 weeks) for the Matrix group, whereas three aneurysms were used at each time point for the HydroCoil and platinum coil groups. Previous work in the rabbit elastase model demonstrated consistent angiographic and histologic results of HydroCoil and platinum coil–treated aneurysms (7, 16). Thus, a lower number of replicates was selected for the HydroCoil and platinum coil groups. In the same work, thrombus organization was shown to be incomplete at 2 weeks, mostly complete at 6 weeks, and complete at 13 weeks. In this study, the 2-week time point was selected to evaluate incomplete organization, whereas the 6- and 10-week time points were selected to evaluate complete organization and the stability of the response.
Details about the embolization procedure have been described elsewhere (11, 16). In brief, anesthesia was induced and maintained as during aneurysm creation. Using a sterile technique, surgical exposure of the right common femoral artery (CFA) was performed and a 5F vascular sheath was placed. Heparin (100 U/kg) was administered intravenously. A 5F catheter (Envoy; Cordis Endovascular) was advanced into the descending aorta. Placement of the guiding catheter in this position results in the microcatheter being relatively poorly supported. We chose this guiding catheter position to simulate the clinical scenario, because modified coil devices may suffer from inferior handling characteristics compared with platinum coils. By using a coaxial technique, a microcatheter (Excelsior 10–18, Boston Scientific) was advanced into the aneurysm. The size of the aneurysm was assessed by direct comparison with radiopaque sizing devices.
Theoretical volumetric occlusion was estimated based on volume of the aneurysm and volume of implanted devices. For these calculations, the aneurysm dome and length, as well as a radiopaque calibration marker, were measured by using a ruler. The volumes of the aneurysms were determined from the dome and length measurements of the aneurysms before embolization. The aneurysms were assumed to be cylindrical and the volume was determined from the equation 
The volumes of the devices were determined by ex vivo measurement. Theoretical volumetric occlusion was determined by taking the sum of the volume of all the devices implanted divided by aneurysm volume.
Embolization was performed in aneurysms by use of either the HydroCoil, platinum coils, or Matrix, as done clinically and according to a randomized schedule. For the platinum coil group, the aneurysm was framed with a single complex coil, embolized by complex and helical coils as densely as possible. Aneurysms in the HydroCoil group were framed with a single platinum complex coil, followed by packing with HydroCoil devices as densely as possible. The Matrix group aneurysms were packed with 2D Matrix coils. The framing and packing strategy was selected to mimic the clinical use of the embolic devices. Efforts were made to avoid protrusion into parent artery in all groups. The total length of devices, number of devices, and procedure time were recorded for each embolization. After embolization, the catheters were removed. The vascular sheath was removed, and the proximal aspect of the femoral artery was ligated with a 4-0 silk suture.
Follow-Up Procedures
Follow-up imaging evaluation and tissue harvest were performed. Subjects euthanized at 2, 6, and 10 weeks underwent intra-arterial digital subtraction angiography (IADSA) at the time of sacrifice. On the day of sacrifice, surgical access of the left CFA was achieved, in similar fashion to that used for access of the right CFA described above. A 5F catheter was placed in the aortic arch, and DSA was performed. Immediately following angiography, the subjects were euthanized by a lethal injection of pentobarbital. The mediastinum was dissected, and the aortic arch and proximal great vessels, including the coil-embolized segment of artery, were exposed and dissected free from surrounding tissues. The tissue was immediately placed in 10% neutral buffered formalin.
Histologic Processing
Three aneurysms from the HydroCoil and Matrix groups at each time point were embedded in methyl methacrylate, sectioned with a diamond saw, and surface-stained with hematoxylin and eosin. The aneurysms from the platinum coil group, as well as two aneurysms from the Matrix group, at each time point were embedded in paraffin. Sections, approximately 1 mm thick, were prepared with a saw. The coils were removed from the sections by hand. The section was re-embedded in paraffin wax, sectioned at 5–10 μ, and stained with hematoxylin and eosin.
Evaluation Criteria
Angiography.
Aneurysm occlusion posttreatment and at follow-up was estimated by a single experienced observer for all time points by using the following categories: complete, near complete, or incomplete. Follow-up angiograms were compared directly to the immediate posttreatment angiogram to assess for treatment durability. Durability was estimated by a single experienced observer for all time points by using the following categories: progressive, stable, or recurrence. Recurrence was defined as any interval increase in contrast opacification of the aneurysm cavity or neck between the immediate postembolization angiogram and the follow-up angiogram. Progressive occlusion was defined as any decrease in contrast opacification of the aneurysm cavity or neck between the immediate postembolization angiogram and the pre-euthanasia angiogram.
Histology.
The methyl methacrylate and paraffin sections were scored according to a semiquantitative scale, with particular attention to the appearance of extracellular matrix within and around the coil mass and the tissue traversing the neck of the aneurysm sac. A qualitative, categorical assessment of histology was performed by two of the authors (D.D. and D.F.K.). The results presented are the concurrence of opinion by both reviewers. In brief, we defined histologic features and noted the “presence” or “absence” in each case. The following features were used: (1) tissue across neck, either fibrinous or cellular; (2) microcompaction at the aneurysm neck, defined as a concave interface with the parent artery; (3) tissue reaction around coil winds; and (4) inflammation. Degree of inflammation was defined as (1) mild, scant, scattered inflammatory cells infiltration; (2) moderate, attenuated, patchy inflammatory cells infiltration; or (3) marked, attenuated, diffuse inflammatory cells infiltration.
Statistical Analysis
All statistical analyses were performed by using JMP software (SAS Institute, Cary, NC). Statistically significant differences in normally distributed data were determined by using an ANOVA test. Statistically significant differences in discrete data were determined by using a χ2 test. In all cases, statistical significance was accepted at α ≤ 0.05.
Results
Procedural Results
Aneurysms were successfully embolized in all 33 cases without acute or chronic morbidity or mortality. Results are summarized in Tables 1 and 2. Statistically significant differences among groups regarding aneurysm size (neck, width, and height), total device length, and procedure time were not present. There were, however, significant differences among the number of devices utilized between three groups. The number of devices implanted in the Matrix group was significantly less than platinum coil (P = .02) and HydroCoil groups (P = .03). Premature detachment occurred in one Matrix coil when we tried to advance it into an aneurysm. Premature detachment did not occur with other devices.
Pooled aneurysm data
Pooled embolization results
Statistically significant differences in the volumetric filling of the aneurysms were present. The volumetric filling of HydroCoil-treated aneurysms (76% ± 32%) was significantly greater than those treated with platinum coils (31% ± 9%; P < .0001) or Matrix coils (23% ± 7%; P < .0001)
Angiography.
Angiographic occlusion scores (complete occlusion/near-complete occlusion/incomplete occlusion) immediately following embolization were 4/5/0, 6/6/3, and 5/3/1 for platinum coils, Matrix coils, and HydroCoil, respectively. At follow-up, angiographic occlusion scores were 4/5/0, 8/2/5, and 8/1/0 for platinum coils, Matrix coils, and HydroCoil, respectively. Follow-up angiographic durability scores (progressive occlusion/stable occlusion/recurrence) were 1/6/2, 2/8/5, and 4/5/0 for platinum coils, Matrix coils, and HydroCoil, respectively (Figs 1–3). There were no cases of delayed, progressive compromise of the parent artery.

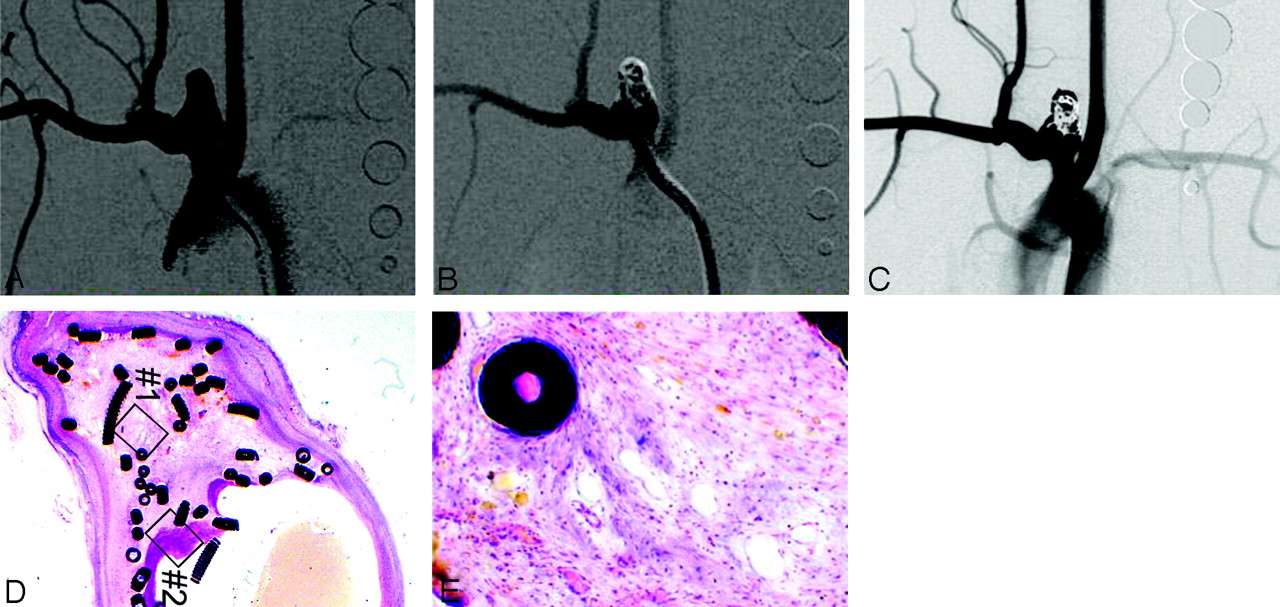
Number 3 aneurysm in Matrix group, 2-week implant.
A, Anteroposterior DSA of the brachiocephalic artery shows a moderately wide-necked aneurysm.
B, Anteroposterior DSA obtained immediately after embolization with Matrix coils shows near-complete occlusion of the aneurysm.
C, Anteroposterior DSA obtained 2 weeks after embolization shows marked coil compaction.
D, Hematoxylin and eosin stain; original magnification, ×1.5. Coronal section obtained through the aneurysm cavity. Microcompaction and inflammation along neck are shown.
E, Hematoxylin and eosin stain; original magnification, ×25. Magnification of the area shown in panel D; substantial inflammation is shown along neck.

Number 9 aneurysm in Matrix group, 10-week implant.
A, Anteroposterior DSA of the brachiocephalic artery shows a wide-necked aneurysm.
B, Anteroposterior DSA obtained immediately after embolization with Matrix coils shows the aneurysm is nearly completely occluded.
C, Anteroposterior DSA obtained 2 weeks after embolization shows slight coil compaction.
D, Hematoxylin and eosin stain; original magnification, ×1.3. Coronal section obtained through the aneurysm cavity. Marked microcompaction and unorganized thrombus are shown. There is no tissue across the aneurysm neck.
E, Hematoxylin and eosin stain; original magnification, ×25. Magnification of the area shown in panel D. Dense cellular infiltration near coils in the dome is seen.

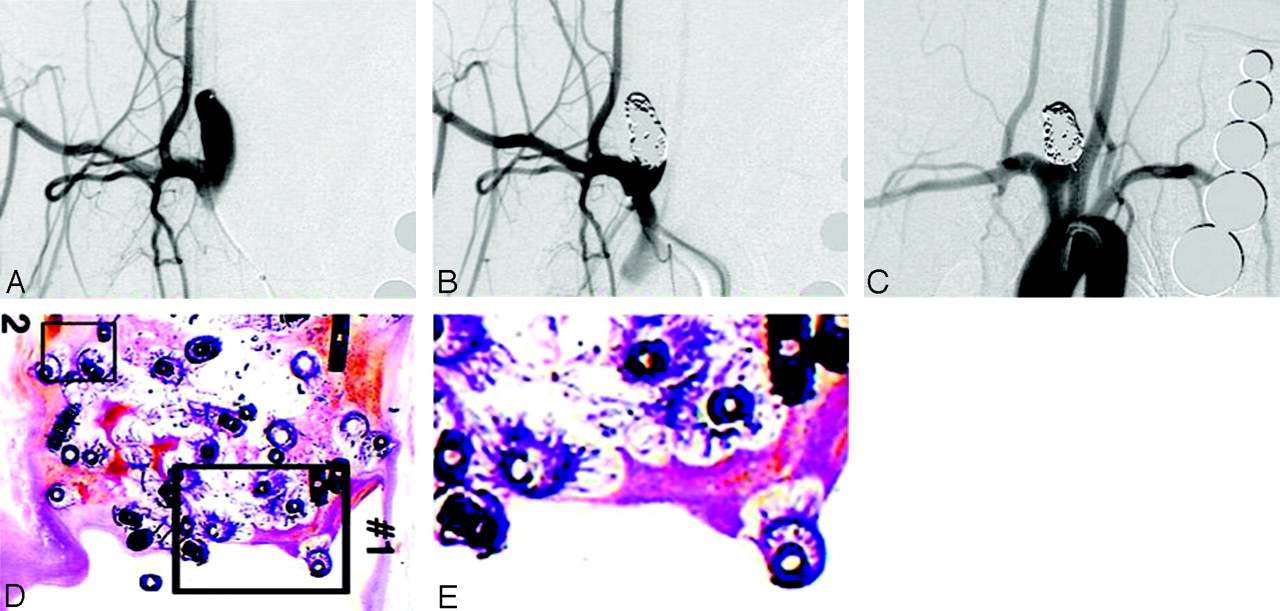
Number 15 aneurysm in HydroCoil group, 6-week implant.
A, Anteroposterior DSA of the brachiocephalic artery shows a wide-necked aneurysm.
B, Anteroposterior DSA obtained immediately after embolization with HydroCoils shows the aneurysm is nearly completely occluded.
C, Anteroposterior DSA obtained 2 weeks after embolization shows the aneurysm remaining stable.
D, Hematoxylin and eosin stain; original magnification, ×1.1. Coronal section obtained through the aneurysm cavity. No substantial inflammatory response is present. Microcompaction is absent. A small part of persistent unorganized thrombus is shown in the aneurysm dome.
E, Hematoxylin and eosin stain; original magnification, ×10. Magnification of the area shown in panel D. Cellular fibrous tissue is shown across the neck.
Histologic Outcomes
Tissue deposition across the aneurysm neck was seen in 1 (11%) of 9 platinum coil samples, 14 (93%) of 15 Matrix samples, and 8 (89%) of 9 HydroCoil samples (Fig 3D–E), indicating significantly increased tissue deposition with the modified coils as compared with platinum (P < .05). Tissue deposition was present in all Matrix samples at 2 and 6 weeks and in four of five samples at 10 weeks. Tissue deposition was present in all HydroCoil samples at 6 and 10 weeks and in two of three samples at 2 weeks.
Inflammation.
Strong tissue reaction around coil surfaces was found more commonly in the Matrix group than that in the HydroCoil and platinum coil groups (P < .05) (Fig 1D–E). Marked levels of tissue reaction, as evidenced by attenuated cellular infiltration around coil surface, was found in nine (60%) aneurysms in the Matrix group (five at 6 weeks, four at 10 weeks; Fig 2D–E) but was not seen in other groups. Mild inflammation was found in seven of the aneurysms in the HydroCoil group (three in 2-weeks group, one in 6-weeks group, three in 10-weeks group). Moderate inflammation was found in two of the aneurysms in the platinum coil group at 10 weeks. Unorganized thrombus and loose connective tissue was consistently found 10 weeks after embolization in the platinum coil group. In the HydroCoil group, much of the aneurysm dome was filled with polymer.
Discussion
In this study, we carried out a direct comparison among platinum coils, Matrix coils, and HydroCoils in the rabbit, elastase-induced aneurysm model, to gain improved understanding of the healing mechanisms of these three devices. We demonstrated that enhanced tissue response, as compared with platinum coils, is reliably achieved with the Matrix coil in this animal model. Even with this enhanced tissue response, however, angiographic outcome was not improved by the Matrix device compared with platinum coils. Indeed, even in cases of marked inflammatory response with Matrix, substantial coil compaction was observed. Conversely, the HydroCoil allowed significant increases in filling volume as compared with other coils and also achieved improved coil stability, on both angiographic and histologic analysis.
We believe that these results offer insights into important mechanisms behind the failure of coils in saccular aneurysms. Our findings indicate that biologic modification alone, without mechanical stability, may fail to improve coil performance. Structural modification, aimed at improving the mechanical stability of the device at the aneurysm neck, may offer a more promising approach to coil design than biologic modifiers. Indeed, from a clinical standpoint, angiographic recanalization is considered a failure, regardless of improved tissue reaction around coils.
Expandible HydroCoils have been shown to fill significantly more volume than nonexpandible platinum coils in both clinical and preclinical studies (32). Histologic study at all time points after embolization showed only small amounts of unorganized thrombus or tissue within aneurysm cavities, with most of the aneurysm cavity filled with expanded hydrogel. Long-term aneurysm occlusion with the HydroCoil device is not dependent on stimulation of host reaction to the implant. Instead, occlusion is achieved by filling of the aneurysm with the biomaterial itself (16). Further, the expanded hydrogel excludes thrombus from the aneurysm cavity, eradicating the tendency for aneurysm regrowth from thrombus resorption or recanalization.
Previous results from the swine aneurysm model showed Matrix accelerates clot organization (13, 15). More organized thrombus, thicker neointima, and neoendothelial coverage of the neck of experimental aneurysms embolized by Matrix in swine were noted within 14 days, as compared with platinum coil (15). In our study using elastase-induced model in rabbits, the occurrence of strong tissue reaction in the Matrix group was higher than that of the HydroCoil and platinum coil groups. Unlike the swine sidewall model, however, coil compaction was commonly seen with Matrix coils in the model used in this study. The rabbit elastase aneurysm is subjected to considerably more hemodynamic stress than the swine sidewall aneurysm, which possibly explains the presence of compaction seen in the rabbit elastase aneurysm and the lack thereof in the swine sidewall aneurysm. Additional clinical data are necessary to assess which of these two models better predicts clinical outcome.
Two variations between groups were present in this study—namely, in the method of embolization and method of histologic processing. The HydroCoil and platinum coil groups were embolized first with a platinum coil. The Matrix group was embolized first with a Matrix coil. This variation was selected to represent the usual clinical practice of the device. We believe that this variation did not affect the outcome of the results. Second, we chose methyl methacrylate embedding for the HydroCoil and Matrix groups and paraffin embedding for the platinum coil group. The choice of methyl methacrylate embedding for HydroCoil and Matrix groups was made on the basis of prior experience of the industry sponsor of this project. Paraffin embedding, a technique still in development, was used for the platinum coils not only to further the development of the technique, but also to achieve efficiency of animal use. It is possible that some difference in histologic outcome may result from differences in processing, but we are not aware of any systematic difference that would have affected the results.
This study, though offering notable findings that may predict the clinical response, had limitations. The number of subjects in each group was small. This limitation is somewhat offset by the finding of relative concordance within each group, which suggests that even more subjects may not have changed outcome. Also, the sizes and neck breadth were variable, and this may have affected outcome in selected cases. Further, there remains no robust histologic grading system that has been shown to predict clinical outcome for any animal model of aneurysms.
We chose to use both angiographic evidence of compaction as well as histologic evidence of compaction in this study. Marked compaction that is evident on histologic sections may be unapparent on angiography (33). This occurs in the setting of a concave, central compaction occurs that may be masked on angiography by the coils remaining in the periphery of the neck.
Conclusions
The use of HydroCoil results in improved long-term occlusion rates compared with Matrix and platinum coils. The Matrix group showed an increase in inflammation and coil compaction compared with HydroCoil and platinum coils.
Footnotes
This study was funded, in part, by MicroVention, Inc., Aliso Viejo, CA, and, in part, by NIH grant NS42646.
Dr. Kallmes is a stockholder in MicroVention.
Presented at the 42nd annual meeting of the American Society of Neuroradiology, Seattle, WA, June 7–11, 2004.
References
- Received October 18, 2004.
- Accepted after revision January 10, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Rabbit Elastase Aneurysm Model Mimics the Recurrence Rate of Human Intracranial Aneurysms following Platinum Coil Embolization
- Assessment of endothelialization of aneurysm wall over time in a rabbit model through CD31 scoring
- Rabbit aneurysm models mimic histologic wall types identified in human intracranial aneurysms
- GEL THE NEC: a prospective registry evaluating the safety, ease of use, and efficacy of the HydroSoft coil as a finishing device
- Testing Stenting and Flow Diversion Using a Surgical Elastase-Induced Complex Fusiform Aneurysm Model
- From bench to bedside: utility of the rabbit elastase aneurysm model in preclinical studies of intracranial aneurysm treatment
- HydroCoils Are Associated with Lower Angiographic Recurrence Rates Than Are Bare Platinum Coils in Treatment of "Difficult-to-Treat" Aneurysms: A Post Hoc Subgroup Analysis of the HELPS Trial
- RNA-Sequencing Analysis of Messenger RNA/MicroRNA in a Rabbit Aneurysm Model Identifies Pathways and Genes of Interest
- Mechanisms of Healing in Coiled Intracranial Aneurysms: A Review of the Literature
- HydroCoils Reduce Recurrence Rates in Recently Ruptured Medium-Sized Intracranial Aneurysms: A Subgroup Analysis of the HELPS Trial
- Correlation of thrombus formation on 7 T MRI with histology in a rat carotid artery side wall aneurysm model
- Reactive tissue proliferation and damage of elastic lamina caused by hydrogel coated coils in experimental rat aneurysms
- Creation of sidewall aneurysm in rabbits: aneurysm patency and growth follow-up
- The next generation HydroCoil: initial clinical experience with the HydroFill embolic coil
- Creation of Bifurcation-Type Elastase-Induced Aneurysms in Rabbits
- Review of 2 Decades of Aneurysm-Recurrence Literature, Part 1: Reducing Recurrence after Endovascular Coiling
- 1-Hexyl n-cyanoacrylate compound (Neucrylate™ AN), a new berry aneurysm treatment. II. Rabbit implant studies: technique and histology
- Embolization of intracranial aneurysms with second-generation Matrix-2 detachable coils: mid-term and long-term results
- The Woven EndoBridge: A New Aneurysm Occlusion Device
- Improved Microsurgical Creation of Venous Pouch Arterial Bifurcation Aneurysms in Rabbits
- Creation of Large Elastase-Induced Aneurysms: Presurgical Arterial Remodeling Using Arteriovenous Fistulas
- Angiographic and Clinical Outcomes in 200 Consecutive Patients with Cerebral Aneurysm Treated with Hydrogel-Coated Coils
- Angiographic and Histologic Comparison of Experimental Aneurysms Embolized with Hydrogel Filaments
- Endovascular Histologic Effects of Ultrathin Gold- or Vitronectin-Coated Platinum Aneurysm Coils in a Rodent Arterial Occlusion Model: A Preliminary Investigation
- A New Endoluminal, Flow-Disrupting Device for Treatment of Saccular Aneurysms
- Endovascular Treatment of Aneurysms: Healing Mechanisms in a Swine Model Are Associated with Increased Expression of Matrix Metalloproteinases, Vascular Cell Adhesion Molecule-1, and Vascular Endothelial Growth Factor, and Decreased Expression of Tissue Inhibitors of Matrix Metalloproteinases
- Control of Aneurysm Volume by Adjusting the Position of Ligation During Creation of Elastase-Induced Aneurysms: A Prospective Study
- Endosaccular Treatment of Intracranial Aneurysms Using Matrix Coils: Early Experience and Midterm Follow-Up