
Through the past decades, many attempts have been made to standardize lumbar disk herniation–related terminology (1, 2). Two different, and not necessarily parallel, sets of characteristics of a herniated disk (HD) are taken into account in the reporting of cross-sectional images of the lumbar spine. First, is the absolute attributes of the HD (ie, morphology, location, volume, etc), and second is the relationship of the HD to its neighboring neural structures. The absolute attributes of a HD are only one set of factors that determine the pattern and degree of compromise of the neighboring neural structures. The morphology and cross-sectional areas of the involved lumbar vertebral and neural foraminae, along with the degree of the epidural fat, are the other determining factors.
Although standardized nomenclature has been proposed for the absolute attributes of a HD, descriptive terminology is used for the elaboration of the relationship of a HD to its neighboring neural structures. Terms such as “abuts,” “impinges,” “flattens,” “indents,” “compresses,” “displaces,” and “distorts” are useful in the description of the effects of a HD on the adjacent thecal sac (TS) and intracanalicular dural nerve root sleeves (DNRSs). The effects of a HD on specific intracanalicular nerve roots may at times also be ascertained by using high-resolution axial T2-weighted sequences of the lumbar spine. In particular, compromise (or maximal degree of compromise) of a lumbar nerve root (LNR) at a level just proximal to its respective neural foraminal exit could be pinpointed to a specific segment of the nerve.
In this context, a 3-tiered descriptive division of the preneural foraminal portion of a LNR, into the lateral thecal sac, junctional, and dural root sleeve segments (Figs 1 and 2) may be of value. This partitioning is particularly suitable at the lower lumbar levels that demonstrate a distinguishable lateral recess and parallels the compartmentalization of the preneural foraminal portion of dural coverings of the LNRs.
The intracanalicular portions of the LNRs demonstrate an intradural topography (the LNRs pierce the dura at the level of their respective neural foraminae) (3), either within the TS (Fig 1A) or in a DNRS (Fig 1C). These sleeves are pinched off from the ventrolateral angles of the TS. This TS-DNRS transition may be evident as “waisting” (Fig 2A) of the ventrolateral angles of the TS. More distally, the passage of the DNRS within the epidural fat (Fig 1C) is reminiscent of the intraorbital course of the optic nerve within the orbital fat.
These proposed segments do not necessarily comply with the localization system proposed by Wiltse et al (4) and later endorsed by the 2001 multidisciplinary task force (1). A particular “zone” may harbor different segments of a LNR (Fig 1), whereas a specific “level” may accommodate different segments of the opposing LNRs (Fig 3).
Awareness of the varying appearances of a LNR within the vertebral foramen may be of value in localizing the level—or maximal level—of neural structural compromise and correlating the imaging findings with the patient’s symptoms. This is especially valuable in herniated disks that demonstrate a volume-neural structural compromise discordance (eg, a small-volume posteriorly HD may cause significant impingement of a neighboring ventrally located preneural foraminal LNR) (Fig 4), and may have a potential role in patient management.

Contiguous axial T2-weighted (3800/97.8) MR images through the L5–S1 level show the 3 segments of the preneural foraminal portion of the S1 nerve root. In this patient, individualization of all of the 3 segments is possible within a single zone.
A, Cranial-most image demonstrates the lateral thecal sac segment of the right S1 nerve root (arrow) in the right central zone.
B, Image shows the junctional zone segment of the right S1 nerve root (long arrow) in the right central zone. This segment, which is situated in the proximal portion of the dural root sleeve, is separated from the contents of the neighboring thecal sac by 2 adjacent layers of dura mater (arrowhead). The thickness of a single layer of dura mater is demarcated (short arrow) in the posterior portion of the thecal sac for comparison.
C, More caudally, image demonstrates the dural root sleeve of the right S1 nerve root (arrow) in the right central zone. Individualization of the contained dural root sleeve segment of the S1 nerve root is not possible in this patient.

Contiguous axial T2-weighted (3700/106.7) MR images through the L5–S1 level show the varying appearances (also refer to Fig 1B) of the proposed “junctional segment” of a lumbar nerve root.
A, Image demonstrates the junctional segment of the left S1 nerve root (long arrow) within the “pinched” portion (arrowheads) of the left ventrolateral angle of the thecal sac. The unrestricted contour of the right ventrolateral aspect of the thecal sac harbors the lateral thecal sac segment of the ipsilateral S1 nerve root (short arrow).
B, Image at a slightly more caudal level shows the proximal-most portion of the left S1 dural nerve root sleeve (arrowheads), the medial wall of which is in close apposition to the ventrolateral wall of the neighboring thecal sac. This portion of the dural root sleeve is also regarded as housing the junctional segment of the S1 nerve root (arrow).

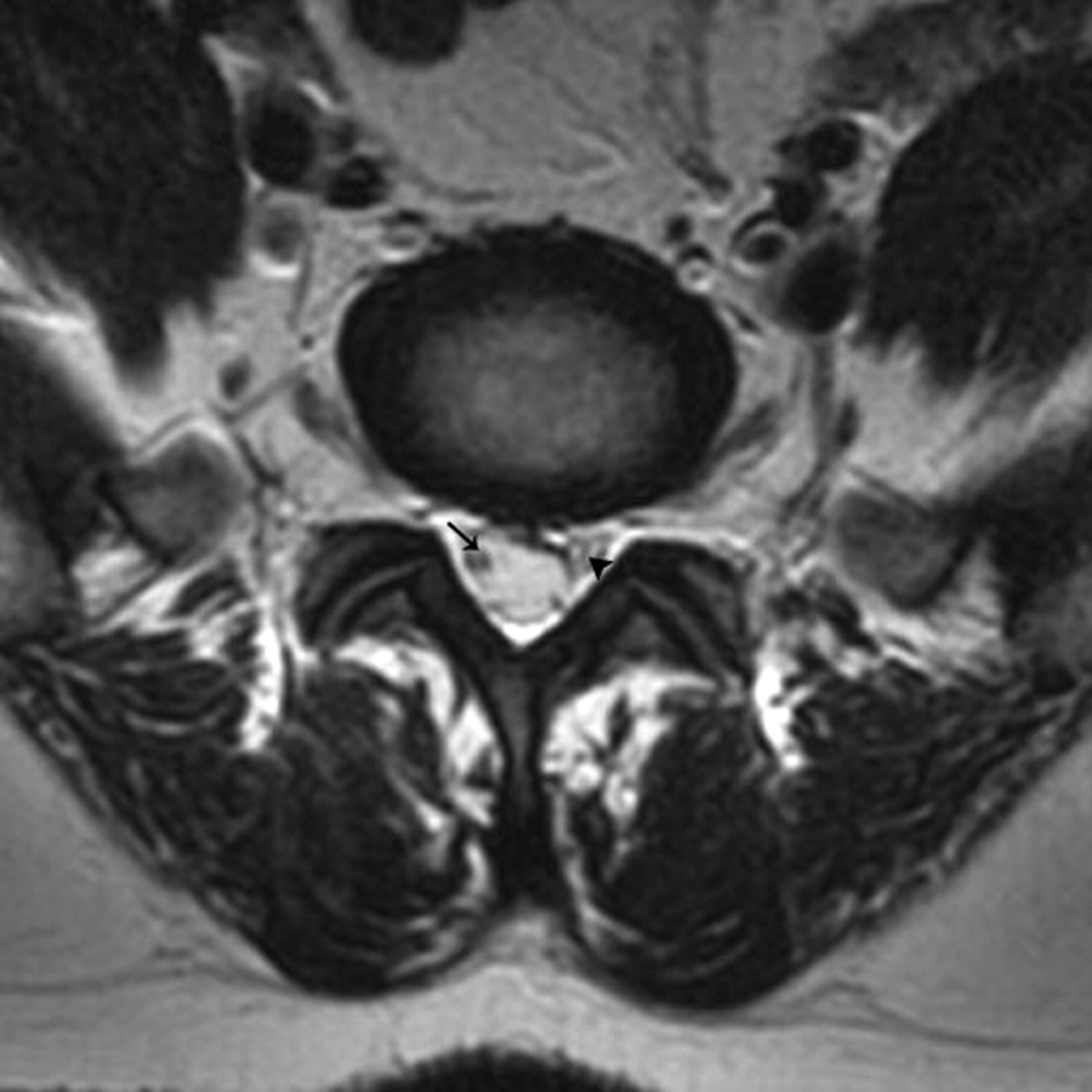
Axial T2-weighted (4000/98) MR image at the diskal-suprapedicular level of L5–S1 demonstrates the nonparallel segmentation of the S1 nerve roots. On the right, the lateral thecal sac segment (arrow), and on the left, the junctional segment (arrowhead), of the S1 nerve roots are visualized.

Contiguous axial T2-weighted (3800/97.8) MR images through the L5–S1 level with the S1 dural nerve root sleeves (individualization of the dural root sleeve segments of the S1 nerve roots within their respective dural sleeves is not possible in this particular patient).
A, Cranial-most image demonstrates the right (long arrow) and left (short arrow) S1 dural nerve root sleeves within the subarticular zones.
B, Image at a slightly more caudal level shows a mild central-subarticular zone disk protrusion that causes a relatively severe compression of the right S1 dural nerve root sleeve (long arrow). The left-sided intact complex is demarcated (short arrow) for comparison.
C, The S1 dural nerve root sleeves (long and short arrows) assume a symmetric appearance at a slightly more caudal level.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.