
Article Figures & Data
Figures
- Fig 1.
FLAIR (A) and isotropic (B) DWI MR images. Normal FLAIR imaging in the context of a 1-day history of right-sided weakness. DWI reveals restriction within the putamen and external capsule (white arrow).
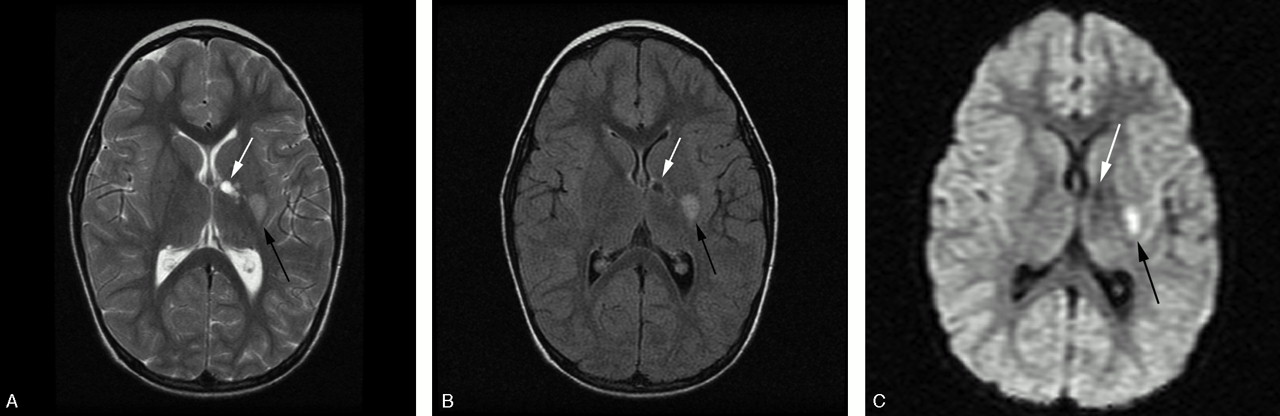
- Fig 2.
T2-weighted (A), FLAIR (B), and isotropic DWI (C) of a unilateral lesion in a patient with an acute or chronic presentation of worsening right-sided weakness. There are 2 T2-weighted hyperintense lesions involving the genu and posterior limb of the internal capsule (white arrow) and posterolateral putamen (black arrow). Both T2-weighted (A) and FLAIR (B) images reveal lesions of differing age with an anteromedial well-defined encephalomalacic cavity and a posterolateral lesion. The isotropic image (C) confirms a new focal area of infarction within the lateral lenticulostriate artery territory (black arrow) as an area of reduced diffusion.
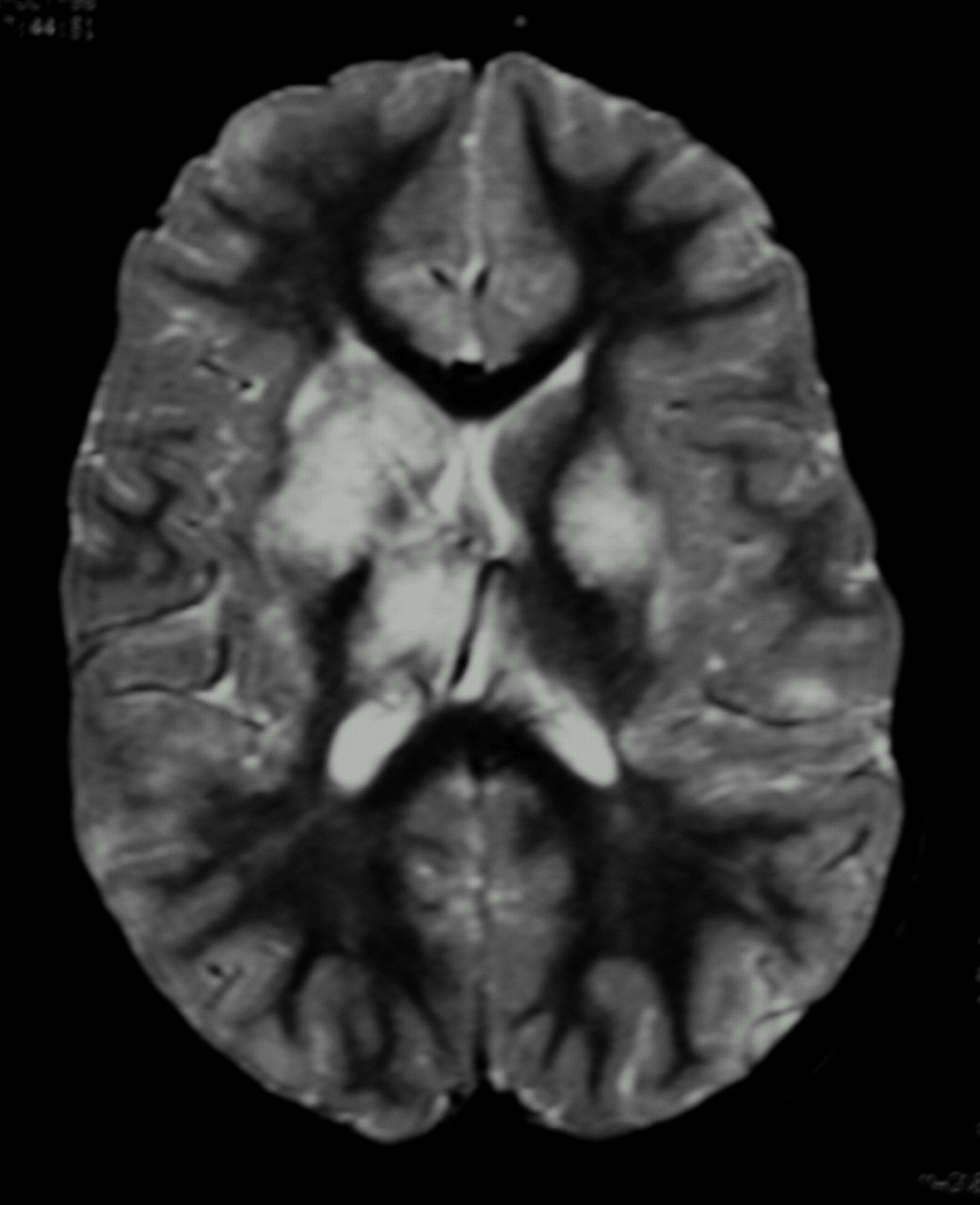
- Fig 3.
Fat-saturated T2-weighted MR imaging of bilateral lesions. There is T2-weighted signal intensity abnormality involving bilateral basal ganglia nuclei, thalami, subcortical, and deep white matter, greater on the right. The distribution of abnormality is consistent with both anterior and posterior circulation involvement.
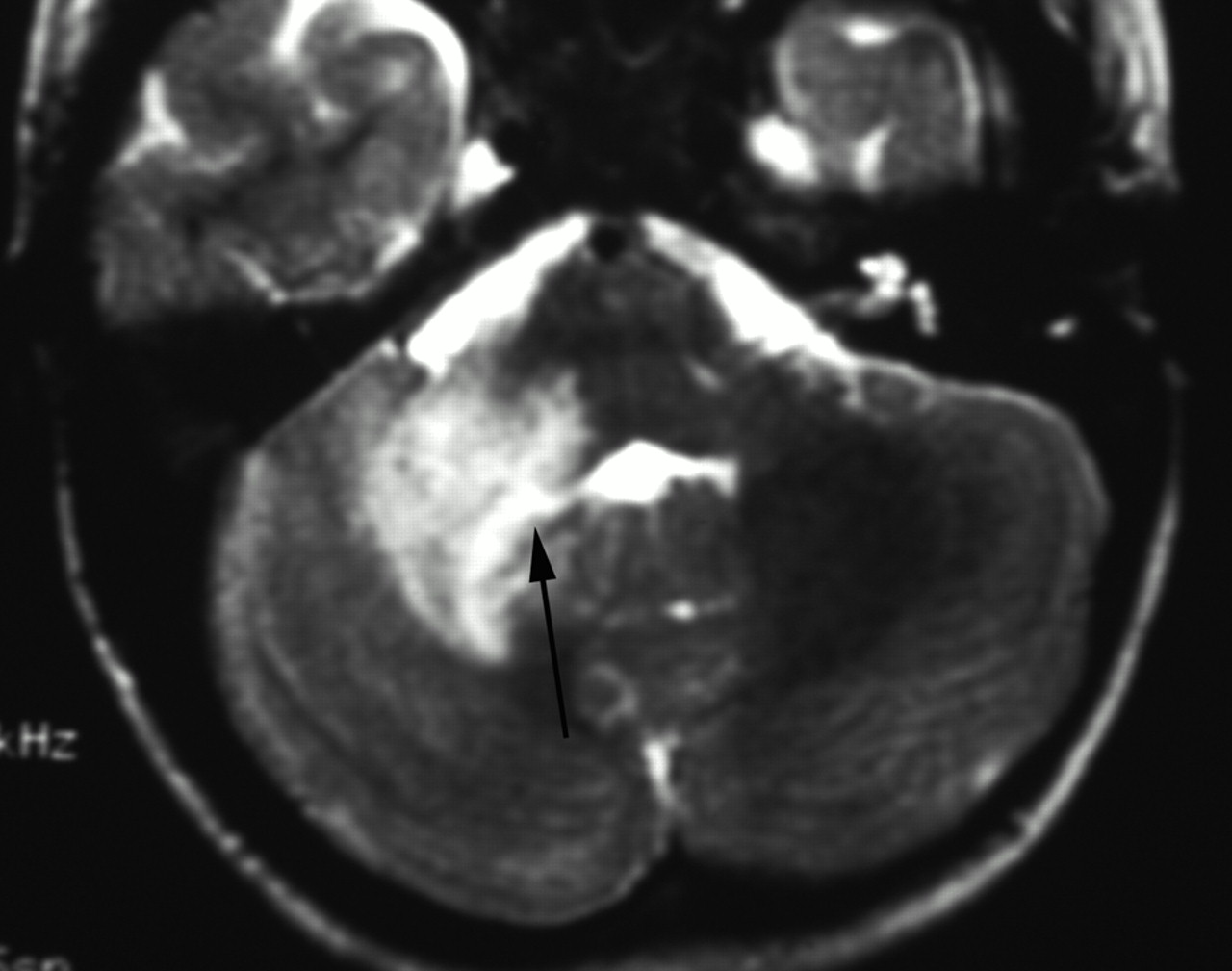
- Fig 4.
T2-weighted MR imaging. There is expansion and irregular hyperintensity within the right middle cerebellar peduncle extending into the right cerebellar deep white matter and dentate nuclei. Mild fourth ventricular effacement is evident (black arrow). The appearances are consistent with anterior inferior cerebellar artery (AICA) and perforator infarcts.
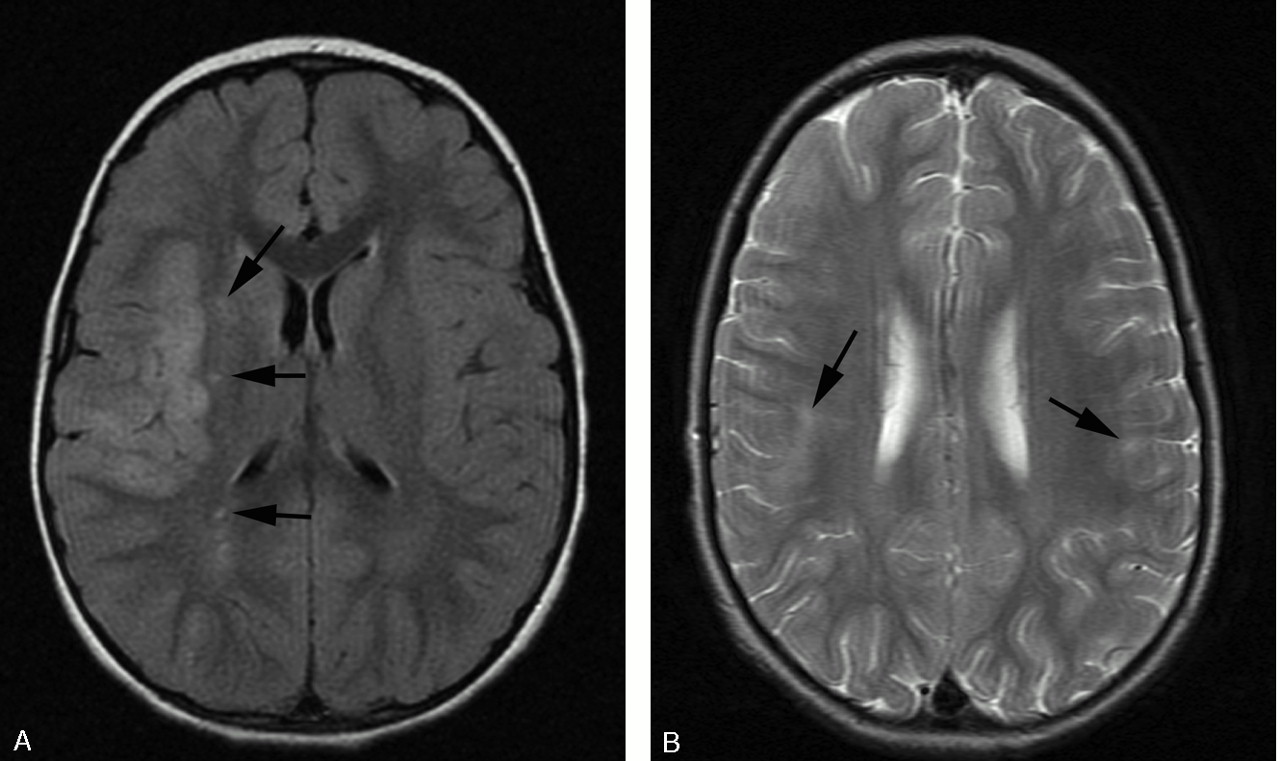
- Fig 5.
A, FLAIR demonstrating acute infarct within a superficial distribution. There is cortical swelling and hyperintensity and adjacent patchy subcortical involvement within the right MCA territory. Additional punctate signal intensity abnormalities are present within the right external capsule and parietal deep white matter (black arrows). B, T2-weighted axial MR imaging demonstrating bilateral peripheral infarcts with hyperintensity within deep and subcortical white matter best appreciated within the right frontal lobe. Bilateral cortical involvement and left deep white matter involvement are appreciated more easily on FLAIR (not shown).
- Fig 6.
Time-of-flight MRA maximum intensity projection (MIP) viewed from posteriorly. The posterior circulation has been removed. There is smooth, regular, concentric, distal left internal carotid and proximal prebifurcation M1 segment flow attenuation (white arrowhead) resulting in reduction in flow signal intensity from remaining MCA branches (white arrow). The A1 segment of the ACA is unaffected. The pattern of proximal involvement was seen in >80% and the “benign” morphology was seen in half of patients studied.
- Fig 7.
Time-of flight MIP oblique view demonstrating distal involvement of the postbifurcation M1 and proximal M2 segments. There is eccentric, irregular narrowing with alternating stenosis and dilation consistent with beading (white arrowheads). “Aggressive” features are said to be the hallmark of vasculitis but were seen in only 11% of our patients. Multiple additional stenoses are present within the left M2 and P2.
- Fig 8.
T2-weighted (A) and FLAIR (B) MR imaging demonstrating focal hyperintensity within the cortex of the postcentral gyrus (white arrow). There is widening of the adjacent sulci providing further clues to previous infarction here but the signal intensity abnormality may be overlooked owing to the adjacent CSF hyperintensity. A small subtle lesion is present within the ipsilateral posterior frontal lobe cortex (black arrowhead). Both the lesions are readily visualized on FLAIR imaging (B).








Tables
Location No. Patients Sublocation No. Patients Supratentorial Cortex 13 (29%) Any deep gray matter 41 (91%) Caudate 25 (56%) Putamen 30 (67%) Globus pallidus 19 (42%) Lentiform 15 (33%) Corpus striatum 7 (16%) Thalamus 10 (22%) Any white matter 39 (87%) Deep 25 (56%) Periventicular 11 (24%) Internal capsule 28 (62%) Subcortical 12 (27%) Infratentorial Gray matter Dentate 0 White matter Brain stem 2 (4%) Cerebellar peduncle 1 (2%) Arterial Territory MR Imaging* ICA NA ACA 0 MCA 169 (89%) PCA 14 (7%) Vertebrobasilar 3 (2%) Anterior horoidal 4 (2%) Note:—ICA indicates internal carotid artery; ACA, anterior cerebral artery; MCA, middle cerebral artery; PCA, posterior cerebral artery; NA, not applicable.
* MR imaging detected 190 lesions.
Arterial Territory Lesions* ICA 14 (18%) ACA 15 (20%) MCA 39 (51%) PCA 6 (10.5%) Vertebrobasilar 0 Anterior choroidal 0 Note:—ICA indicates internal carotid artery; ACA, anterior cerebral artery; MCA, middle cerebral artery; PCA, posterior cerebral artery.
* MR angiography detected 76 lesions, including 2 aneurysms.
Morphology Stenoses* Smooth 56 (78%) Irregular 14 (19%) Concentric 68 (94%) Eccentric 2 (3%) Graduated 12 (17%) Single 65 (90%) Beading 8 (11%) * MRA demonstrated a total of 72 stenoses.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Primary Angiitis of the Central Nervous System: Magnetic Resonance Imaging Spectrum of Parenchymal, Meningeal, and Vascular Lesions at Baseline
- The growing spectrum of antibody-associated inflammatory brain diseases in children
- Clinical Reasoning: An 8-year-old girl with multifocal brain lesions and cerebral edema
- Multiple brainstem infarctions in a boy caused by angiitis of the basilar artery
- Reply:
- MRI features of pediatric multiple sclerosis
- Mode of Onset Predicts Etiological Diagnosis of Arterial Ischemic Stroke in Children