
Abstract
SUMMARY: Remote cerebellar hemorrhage (RCH) is a rare but benign, self-limited complication of supratentorial craniotomies that, to the best of our knowledge, has not been described in the imaging literature. RCH can be an unexpected finding on routine postoperative imaging studies and should not be mistaken for more ominous causes of bleeding such as coagulopathy, hemorrhagic infarction, or cortical vein occlusion. Cerebellar hemorrhage in the typical setting can be identified as RCH and does not require more extensive or invasive evaluation.
Hemorrhage in and around the operative site is common following neurosurgical procedures. Hemorrhage at remote sites such as epi- or subdural and subarachnoid spaces is not uncommon. Cerebellar hemorrhage after supratentorial craniotomy is a rare, self-limiting phenomenon that should not be mistaken for more ominous pathologic findings such as hemorrhagic infarction. About 100 cases of remote cerebellar hemorrhage (RCH) have been reported in the neurosurgical literature,1–16 but none has been reported in the radiologic literature to date.
In this report, we introduce the concept of RCH to the neuroradiologic community by reporting 7 patients who developed RCH after supratentorial craniotomy and one following penetrating head trauma. We review the literature and discuss the risk factors, as well as possible theories to explain the cause, of this rare but generally benign phenomenon.
Seven patients who developed RCH following craniotomy for supratentorial pathologies and one after penetrating head trauma were identified, and their charts were reviewed (Table). Age, sex, presentation, location and type of underlying pathology, coagulation parameters, and clinical course including preoperative usage of anticoagulation agents, history and perioperative hypertension, and postoperative epidural drainage were assessed. CT and MR imaging scans were reviewed, and the imaging findings were categorized.
Summary of patients’ age, primary pathology, site of craniotomy, symptoms, location of bleed site, and complications
Case Reports
Case 1
A 67-year-old woman had an unruptured right internal carotid artery paraclinoid aneurysm identified during work-up for Ménière disease. She underwent a right craniotomy for clipping of the aneurysm with intraoperative angiography and a temporary occlusion balloon placed in the right carotid artery for proximal control. The surgery was tolerated well; however, she was slow to awaken postoperatively. A noncontrast CT of the head demonstrated postoperative changes of uncomplicated craniotomy as well as a small remote left cerebellar hemorrhage. She was observed closely by intracranial pressure monitoring and good blood pressure control. Initially, the patient had mild gait imbalance, though she returned to her baseline 4 months later.
Case 2
A 65-year-old woman presented with visual loss. MR imaging was suggestive of an aneurysm, and cerebral angiography confirmed an anterior communicating artery and middle cerebral artery aneurysm. The patient was observed for a few months and subsequently underwent right pterional craniotomy for clipping of both aneurysms. She tolerated the procedure well, but a left cerebellar hemorrhage was noted on her follow-up CT scan on postoperative day 1. Initially, she had some minor confusion and left-sided ataxia associated with the hemorrhage, but she continued to make a steady recovery. At her 3-month follow-up, no residual neurologic deficits were identified.
Case 3
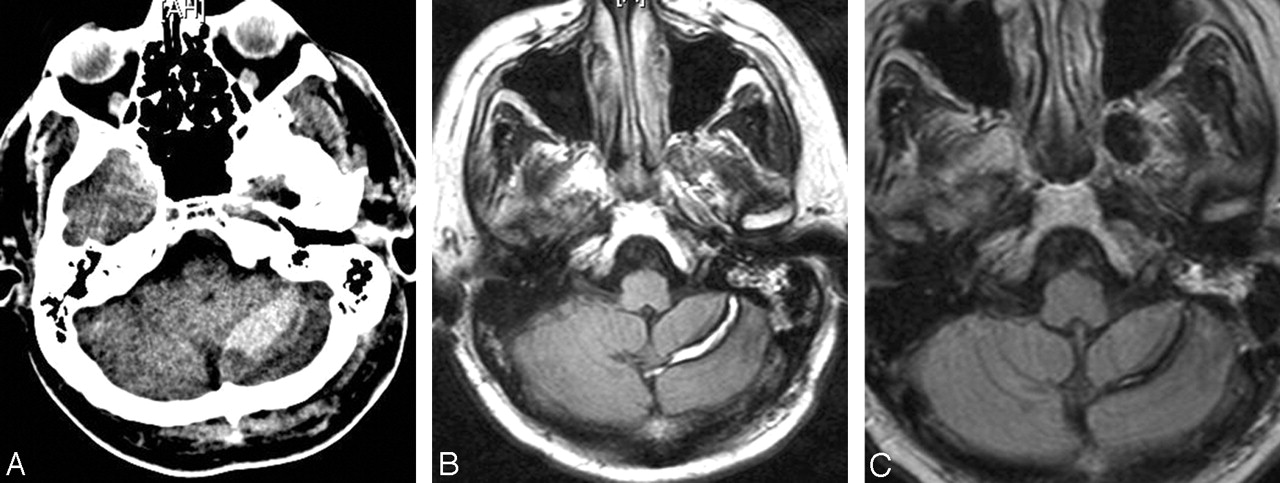
A 36-year-old woman presented with a history of nocturnal seizures. MR imaging showed a nonenhancing lesion in the right frontal lobe. The patient underwent resection of the mass, which revealed an oligodendroglioma (WHO grade II). She tolerated the procedure well; however, a postoperative CT scan revealed a left cerebellar hemisphere hemorrhage, which was confirmed on MR imaging (Fig 1). No underlying lesion was identified. The patient was transferred to the intensive care unit for closer observation, where she was found to have developed dysmetria as well as some mild ataxia and dizziness. A follow-up CT scan showed no further progression of her cerebellar hemorrhage. On 6-month follow-up, she was doing very well, without any neurologic deficits.


Patient 3. Axial T2-weighted (A), FLAIR (B), and gradient–refocused (C) images show a left cerebellar hemisphere hemorrhage with mild mass effect and minimal adjacent edema. No enhancement is seen on the postcontrast T1-weighted MR image (D). Diffusion-weighted MR image (E).
Case 4
A 28-year-old man presented with severe headaches and vertigo. MR imaging and CT scans revealed a ruptured left anterior temporal arachnoid cyst with associated hemorrhage into a subdural hygroma. A craniotomy was performed for fenestration of the arachnoid cyst and drainage of both subacute subdural hygroma and hematoma. The procedure was well tolerated, but the patient continued to experience residual nausea. Routine postoperative CT revealed a right RCH. The nausea gradually resolved, and he was discharged on postoperative day 6. At 1-month follow-up, he had no symptoms or neurologic deficits.
Case 5
A 53-year-old man with a history of glioblastoma multiforme and previous surgical resection, radiation, and chemotherapy presented with tumor progression. The patient underwent a conscious craniotomy for resection of the recurrent tumor. The patient tolerated the procedure well. Postoperative CT showed an asymptomatic RCH (Fig 2A). On postoperative day 2, he was found to have hyponatremia and was treated with 3% sodium. The patient continued to do well, and a follow-up MR imaging 2 months later showed expected evolution of the hematoma without recurrence (Figs 2B, -C).

Patient 5. A, Immediate postoperative CT showing left RCH. Three-month follow-up MR T2-weighted (B) and FLAIR (C) images show a hemosiderin ring surrounding the resolving hematoma.
Case 6
A 33-year-old man was admitted after a self-inflicted gunshot wound to the head. At the scene, he was found to have a Glasgow Coma Score of 3 and was intubated. On arrival, his pupils were fixed and dilated bilaterally. He had no corneal, oculocephalic, or gag reflexes. An entrance wound was identified on his right temple without any clear exit wound. He was actively bleeding from his ears and mouth. A CT scan showed a projectile that passed from the right frontal bone across the midline and both lateral ventricles to impact the left parietal bone, where the bullet was retained. Bilateral intraventricular hemorrhage, bilateral convexity subarachnoid hemorrhage, left-sided subdural hematoma, and transtentorial herniation were identified. In addition, a focus of remote intraparenchymal cerebellar hemorrhage was identified. He was taken to the surgical intensive care unit, where he was pronounced dead after a formal brain death examination.
Case 7
A 29-year-old man presented with a history of petit mal and grand mal seizures. MR imaging of the brain revealed a 1-cm vascular lesion in the left mesiotemporal region consistent with a cavernous malformation. The patient underwent left pterional craniotomy for resection of the cavernous malformation. He tolerated the procedure well; however, on routine postoperative MR imaging he was found to have a right RCH. The patient’s postoperative course was unremarkable, and he was discharged to home on postoperative day 3.
Case 8
A 53-year-old man presented with acute onset of severe headache, nausea, and vomiting. His CT scan showed diffuse subarachnoid hemorrhage. Cerebral angiography revealed a ruptured right middle cerebral aneurysm. The patient underwent a right pterional craniotomy for clipping of the aneurysm and tolerated the procedure well. Postoperatively, the patient remained neurologically intact without any deficits, but a routine follow-up CT of the head showed bilateral RCH (Fig 3). The patient continued to do well, without any neurologic deficits.

Patient 8. Postoperative noncontrast-enhanced CT shows bilateral RCH (arrowheads). Arrow indicates a surgical clip placed on the right middle cerebral artery aneurysm.
Discussion
RCH is an alarming but seldom reported complication of supratentorial craniotomies. Approximately 100 cases have been described in neurosurgical journals, but, to the best of our knowledge, this phenomenon is unknown in the imaging literature.
RCH has been reported after a variety of neurosurgical procedures. Although RCH has occurred most often after frontotemporal or frontal craniotomies, it does not seem to be related to any specific type of surgery. RCH occurs after a variety of supratentorial procedures, including aneurysm clipping, temporal lobectomy, tumor resection, and hematoma evacuation. RCH is most common between the ages of 30 and 60 years, though it has been reported in patients as young as 10 and as old as 83 years.
The most common presenting symptom of RCH is decreased level of consciousness. Other common symptoms include motor deficits, gait ataxia, and prolonged awakening from anesthesia. Some cases are asymptomatic and found incidentally on postoperative CT or MR imaging. RCH can occur contralateral (cases 1–4, 7) or ipsilateral (case 5) to the site of craniotomy or may occasionally be bilateral (case 8).
Identifying the cause and true risk factors of RCH is difficult. Friedman et al2 reported 43 cases of RCH, concluding that RCH usually follows supratentorial procedures that involve opening of cisterns or ventricular systems with patients in a supine position. They proposed that opening of cisterns and the ventricular system causes CSF hypovolemia resulting in cerebellar sagging. This causes transient occlusion of the superior bridging veins of the posterior fossa, leading to subsequent hemorrhagic infarction. Yoshida et al16 and Konig et al7 proposed that RCH relates to the amount of CSF drained postoperatively. Postoperative overdrainage by negative suctioning may lead to downward displacement of the cerebellum, causing tearing of the superior cerebellar vein and tributaries. This phenomenon could mimic “sinking brain syndrome,” as described by Kelley and Johnson17; however, RCH has not been reported with the “sagging brain” found in many cases of intracranial hypotension.
Friedman et al2 also found that preoperative acetylsalicylic acid (ASA) usage and elevated intraoperative systolic blood pressure are possible modifiable risk factors associated with RCH. On the other hand, Marquardt et al9 reported that only one of their 9 patients had a history of well-controlled hypertension. They concluded that there was no relationship between history of hypertension or preoperative hypertension and RCH. Similarly, no incidences of perioperative hypertension were observed in our patients, which indicates that perioperative hypertension is probably not the most important factor causing RCH.
Even though Marquardt et al9 were not able to find any correlation between coagulation parameters and RCH, they proposed that abnormal blood coagulation could be a contributor of RCH. Friedman et al2 found that use of ASA within 7 days of surgery did increase the risk of RCH, yet they reported that there were no differences between control and RCH patients’ coagulation parameters. Preoperative ASA should increase not only the risk of infratentorial bleeding but also the risk of supratentorial bleeding. Coagulation parameters may have an indirect effect on cerebellar hemorrhage; these certainly does not seem to be a major contributor.
The underlying lesion for which the supratentorial craniotomy is performed seems unrelated to spontaneous cerebellar hemorrhage. Lesions have included a variety of pathologies, such as aneurysms, tumors, hematomas, temporal sclerosis, or atrophy.
RCH seems to be a self-limiting and identifiable complication of supratentorial craniotomies that should not be mistaken for more ominous pathologies such as hemorrhagic infarction. None of our patients required further work-up or intervention. Location and size of the bleed may have an important prognostic value. If the bleed is large enough to cause mass effect leading to obstructive hydrocephalus, surgical intervention may be indicated. Smaller bleeds with little or no mass effect, however, seem to be self-limiting and do not require further work-up. Follow-up CT is helpful in assessing the natural evolution of the bleed.
Conclusions
The precise mechanism by which cerebellar hemorrhage occurs following supratentorial craniotomy is unknown; however, male sex, perioperative hypertension, and preoperative usage of anticoagulation are possible risk factors for RCH. RCH seems to be a self-limiting phenomenon, and further surgical and diagnostic evaluation is not required in most cases.
Acknowledgments
We thank Kristin Kraus for her editorial assistance in preparing this report.
References
- Received January 24, 2005.
- Accepted after revision April 5, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}