
Article Figures & Data
Figures
- Fig 1.
High-resolution CT angiography (HCRTA) of a ruptured anterior communicating artery (AcomA) aneurysm with Fisher IV subarachnoid hemorrhage. The aneurysm is wide-necked, arising from the junction of the A1-A2 segments of the anterior cerebral artery on both sides and from the AcomA. It projects anteriorly, from left to right, and slightly inferiorly (A). This aneurysm developed unbalanced contact constraints with the adjacent right gyrus rectus (B) and the planum sphenoidale (C–E). The aneurysm was irregular with a bleb on its left lateral surface (B). Note how the bleb arises from the surface of the aneurysm that faces the free subarachnoid space. The surface of the aneurysm, which is in contact with the planum sphenoidale, shows a flattened contour in relation to the imprint from the adjacent bone (C and D). In this case, the shape of the aneurysm was directly modified by a contact constraint with the perianeurysmal environment.
A, 3D reconstruction, posteroanterior view. Asterisk, anterior clinoid processes.
B, Axial HCRTA. Single arrow, bleb; double arrow, unbalanced contact constraint with gyrus rectus.
C and D, Coronal and sagittal plane multiplanar reconstructions. White arrow, contour deformation of the surface of the aneurysm in contact with the planum sphenoidale.
E, 3D reconstruction, anteroposterior, slightly oblique view. Small arrow, bleb; large arrow, contact constraint with planum sphenoidale.
- Fig 2.
A 47-year-old man with chronic headache. A left, unruptured middle cerebral artery (MCA) aneurysm was suspected during routine CT, which motivated high-resolution CT angiography (HCRTA). HRCTA revealed a 6-mm MCA aneurysm, which pointed inferiorly and was embedded in the temporal lobe (A–D). The whole circumference of the aneurysm was surrounded by brain tissue, resulting in a balanced contact constraint (A–C). This aneurysm had regular contours.
A–C, Sequential, coronal plane, multiplanar reconstructions of HRCTA. arrows, balanced contact constraint with surrounding temporal lobe parenchyma.
D, Three-dimensional reconstruction of HRCTA, left superior view. A, MCA aneurysm; asterisk, posterior clinoid process.
- Fig 3.
Ruptured, right-sided giant middle cerebral artery (MCA) bifurcation aneurysm with right, intraparenchymal temporal lobe hematoma. On noncontrast CT, the aneurysm was seen as a round structure that was hypoattenuated compared with the temporal lobe hematoma (A). Postcontrast high-resolution CT angiography (HCRTA) showed an unbalanced contact constraint with the frontal and temporal lobes (B) and with the greater sphenoid wing (C–E). The aneurysm had a regular shape with no blebs. This case showed how the trajectory and growth of the aneurysm could have been influenced by the contact constraints it developed with the perianeurysmal environment. As it grew, this aneurysm was probably canalized laterally and outward by the adjacent frontal and temporal lobes that delimitate the sylvian fissure, and then, when it developed a contact constraint with the sphenoid greater wing, it grew caudally toward the middle cranial fossa.
A, Axial, noncontrast enhanced, HRCT. A, aneurysm; H, hemorrhage.
B and C, Axial, postcontrast HRCTA. H, hemorrhage.
D, 3D reconstruction of HRCTA, superior view.
E, 3D reconstruction of HRCTA, posteroanterior view.
- Fig 4.
Axial noncontrast CT. Ruptured anterior communicating artery (AcomA) aneurysm with Fisher IV subarachnoid hemorrhage (SAH). The SAH delineates the cisternal portion of both occulomotor nerves (white arrows), which appear as a “negative print” within the blood clot. In such cases, contact constraints between an aneurysm with the occulomotor nerve could readily be identified.
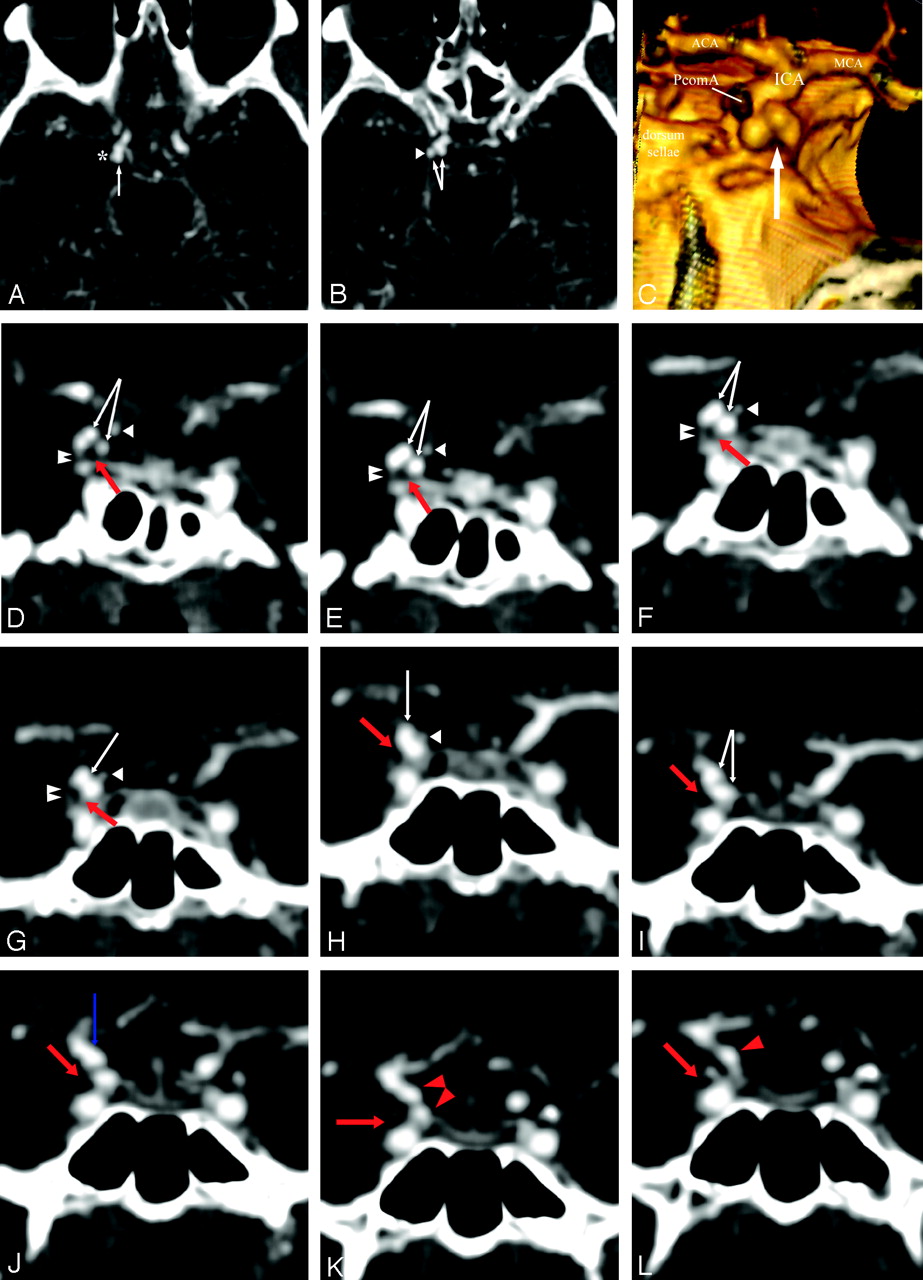
- Fig 5.
High-resolution CT angiography (HCRTA) of a ruptured right posterior communicating artery (PcomA) aneurysm with Fisher IV SAH. This aneurysm is highly irregular with multiple blebs (A–C). Axial HRCTA images show unbalanced contact constraints with the mediotemporal lobe (A) and the free border of the tentorium cerebelli (B). Coronal plane reconstructions show the occulomotor nerve as a round nonenhancing structure and the free edge of the tentorium as an enhancing, linear, slitlike structure (D–L). The contours of the aneurysms are clearly deformed by the imprint of these 2 structures on its inferior surface. The PcomA is visualized medially to the aneurysm.
A and B, Axial HRCTA images. White arrow, PcomA aneurysm; asterisk, contact with the mesiotemporal lobe; arrowhead, contact with the free border of the tentorium cerebelli.
C, 3D reconstruction of HRCTA, posteroanterior view. Arrow, imprint from free border of tentorium cerebelli and right occulomotor nerve.
D–L, Coronal plane, sequential, back to front, thin section multiplanar reconstruction of the PcomA aneurysm. Double arrowhead, free border of the tentorium cerebelli; white arrowhead, PcomA; red arrow, right occulomotor nerve; white arrow, PcomA aneurysm; red arrowhead, cisternal internal carotid artery (ICA); blue arrow, ICA-PcomA aneurysm junction.
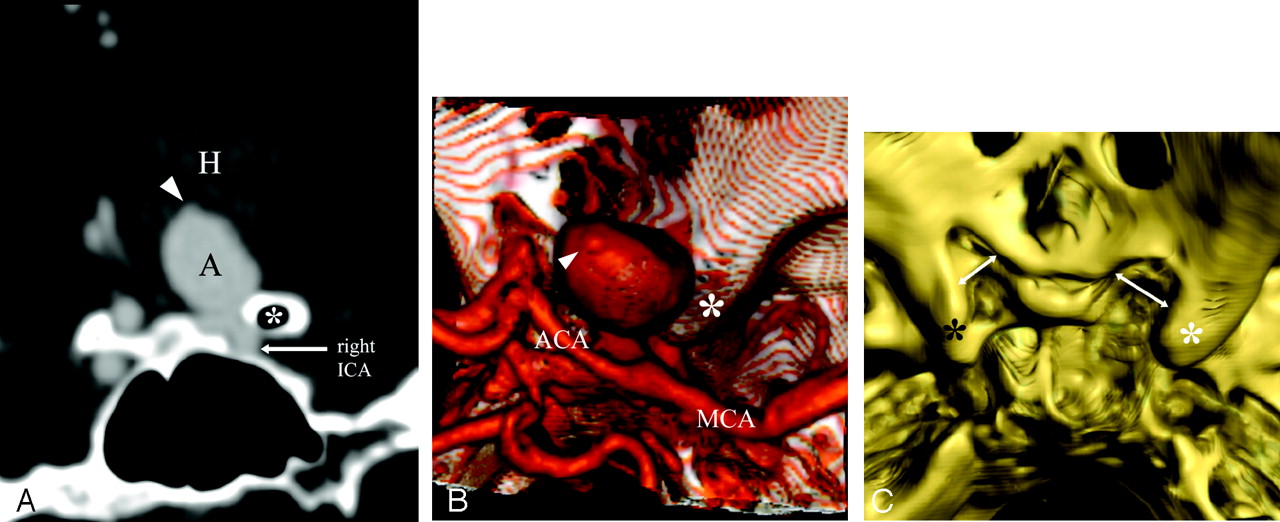
- Fig 6.
Ruptured, right-sided, 18-mm carotido-ophthalmic aneurysm with intraparenchymal hemorrhage into the right basal frontal lobe and basal ganglia (A and B). The aneurysm expanded superiorly and became embedded into the basal frontal lobe. It developed unbalanced contact constraints with a pneumatized, right anterior clinoid process (A). A contact constraint with the right optic nerve and chiasma was suspected from the location of the aneurysm, and was confirmed surgically. The aneurysm presented with a bleb at the dome (A and B). Bone 3D reconstructions revealed bony erosions of the right optic gutter and right anterior clinoid process in relation to the mass effect from the aneurysm (C).
A, Coronal plane, multiplanar reconstruction of the high-resolution CT angiography (HCRTA), posteroanterior view. Asterisk, right anterior clinoid process; A, aneurysm; H, intraparenchymal hemorrhage in the right basal ganglia; arrowhead, bleb.
B, 3D reconstruction of HRCTA, superior view. Asterisk, right anterior clinoid process; arrowhead, bleb.
C, 3D bone reconstruction of the base of the skull from HRCTA images. White asterisk, right anterior clinoid process; black asterisk, left anterior clinoid process; arrows, bony erosion of right optic gutter and right anterior clinoid process compared with the left side.







Tables
Site Group 1 (%) Group 2 (%) ACA 3 1.5 AchoA <1 4.5 AcomA 37 15 AICA 2 0 PCA 2.5 3 BA tip 4 7.5 ICA 5.5 14 MCA 22 44 PcomA 20 9 PICA 3 1.5 Note:—ACA indicates anterior cerebral artery (all segments included); AchoA, anterior choroidal artery; AcomA, anterior communicating artery; AICA, anterior inferior cerebellar artery; PCA, posterior cerebral artery (all segments included); BA, basilar artery; ICA, internal carotid artery (supraclinoid portion only; PcomA and AchoA aneurysms are considered separately); MCA, middle cerebral artery (all segments included); PcomA, posterior communicating artery-ICA junction; PICA, posterior inferior cerebellar artery. Bold- face type within each group indicates the first 3 more frequent locations.
Group 1 Group 2 No. of aneurysms with contact with bone or dura 32 4 Contour deformation of the aneurysm 20 (62.5%) 2 (50%) Deformation of the PAE by aneurysm (bone erosion) 5 (15.6%) 2 (50%) Location PcomA 9 (45%) — AcomA 5 (25%) — ICA/ophthalmic 1 (5%) 2 (100%) ICA C1/C2 1 (5%) — MCA 3 (15%) — PCA P1/P2 1 (5%) — Note:—PAE indicates perianeurysmal environment; PcomA, posterior communicating artery; AcomA, anterior communicating artery; ICA, internal carotid artery; MCA, middle cerebral artery; PCA, posterior cerebral artery.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Hemodynamic Characteristics in Ruptured and Unruptured Intracranial Aneurysms: A Prospective Cohort Study Utilizing the AneurysmFlow Tool
- Intracranial Aneurysmal Pulsatility as a New Individual Criterion for Rupture Risk Evaluation: Biomechanical and Numeric Approach (IRRAs Project)
- Difference in Aneurysm Characteristics Between Ruptured and Unruptured Aneurysms in Patients With Multiple Intracranial Aneurysms
- Quantitative Hemodynamic Analysis of Brain Aneurysms at Different Locations
- Hemodynamic Patterns of Anterior Communicating Artery Aneurysms: A Possible Association with Rupture