
Abstract
SUMMARY: This case report demonstrates delayed rupture of a cavernous carotid fistula and aneurysm into the temporal lobe 12 years after treating a direct cavernous carotid artery fistula using detachable silicon balloons. The ultimate treatment was performed using arterial endovascular sacrifice. Successful treatment of cavernous carotid fistulas may ultimately lead to formation of cavernous aneurysms. Although these lesions rarely cause intraparenchymal hemorrhage, the risk for such an event must be taken into consideration when patients are treated for the initial lesion.
Direct carotid cavernous sinus fistulas (CCF) (Barrow type A) are usually secondary to either traumatic injury to the cavernous segment of the internal carotid artery (ICA) or spontaneous rupture of a cavernous ICA aneurysm.1 These lesions generally lead to visual and ocular changes secondary to venous hypertension and elevated intraocular pressure, ophthalmoplegia, and audible bruit. Intracranial hemorrhage (subarachnoid or intraparenchymal) is a rare complication due to the carotid artery being encased by the cavernous sinus walls, which are extradural relative to the intracranial compartment. We report a case of a traumatic direct CCF that was successfully treated by using detachable balloons, yet 12 years later, the patient presented with cavernous carotid origin aneurysm rupture into his adjacent temporal lobe.
Case Report
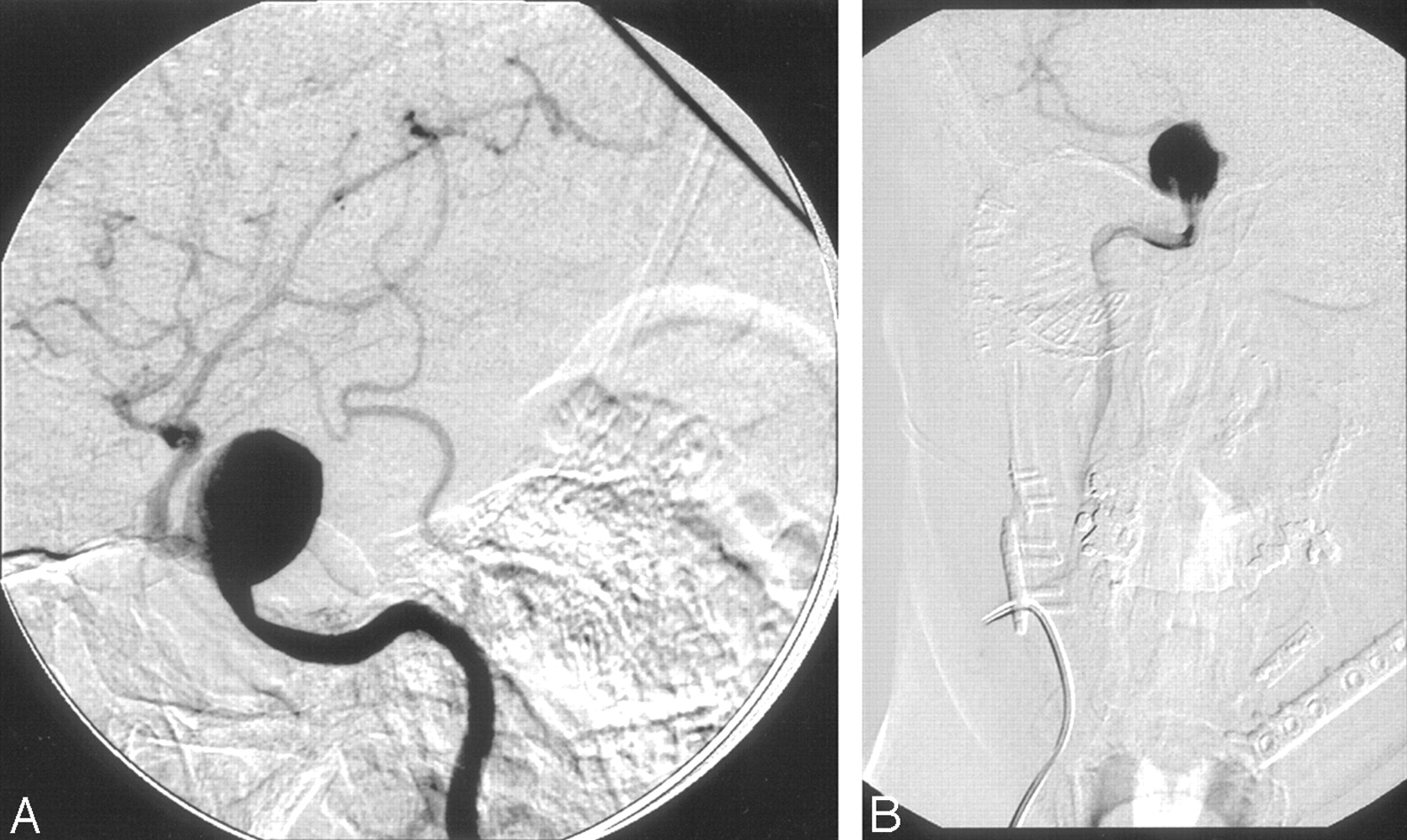
A 32-year-old right-handed man initially presented 12 years earlier with traumatic right ocular blindness and a Barrow type A CCF (Fig 1). The lesion was treated successfully at the time by using detachable silicon balloons placed across the arterial tear and into the cavernous sinus (Fig 2). The patient remained clinically stable for 2 years and then presented with headaches. At that time, arteriography demonstrated a right cavernous carotid aneurysm with no fistulous drainage, the lesion was not treated,, and the patient’s headaches resolved.

Anteroposterior ICA arteriogram showing CCF with rapid venous drainage.

Anteroposterior right common carotid artery arteriogram obtained after placement of 3 detachable silicon balloons (arrow) into the cavernous sinus. The direct CCF is absent.
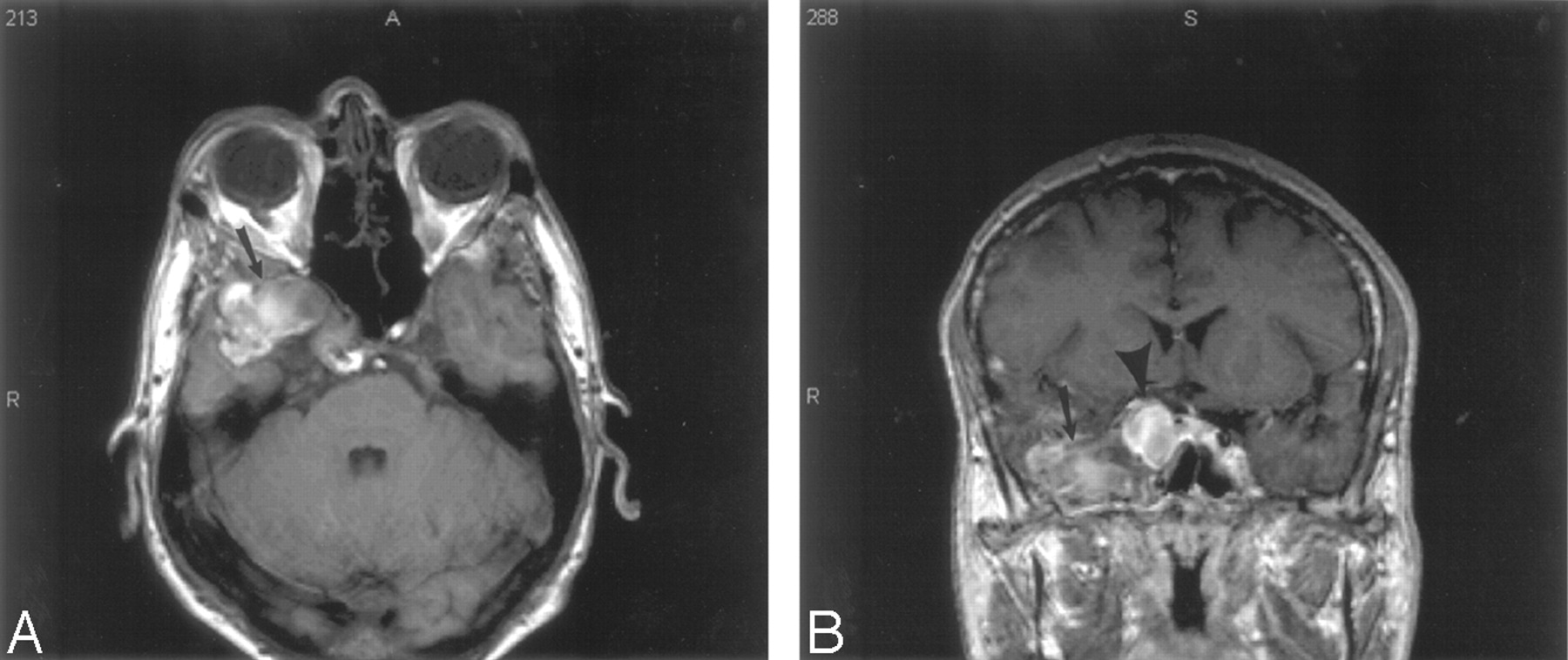
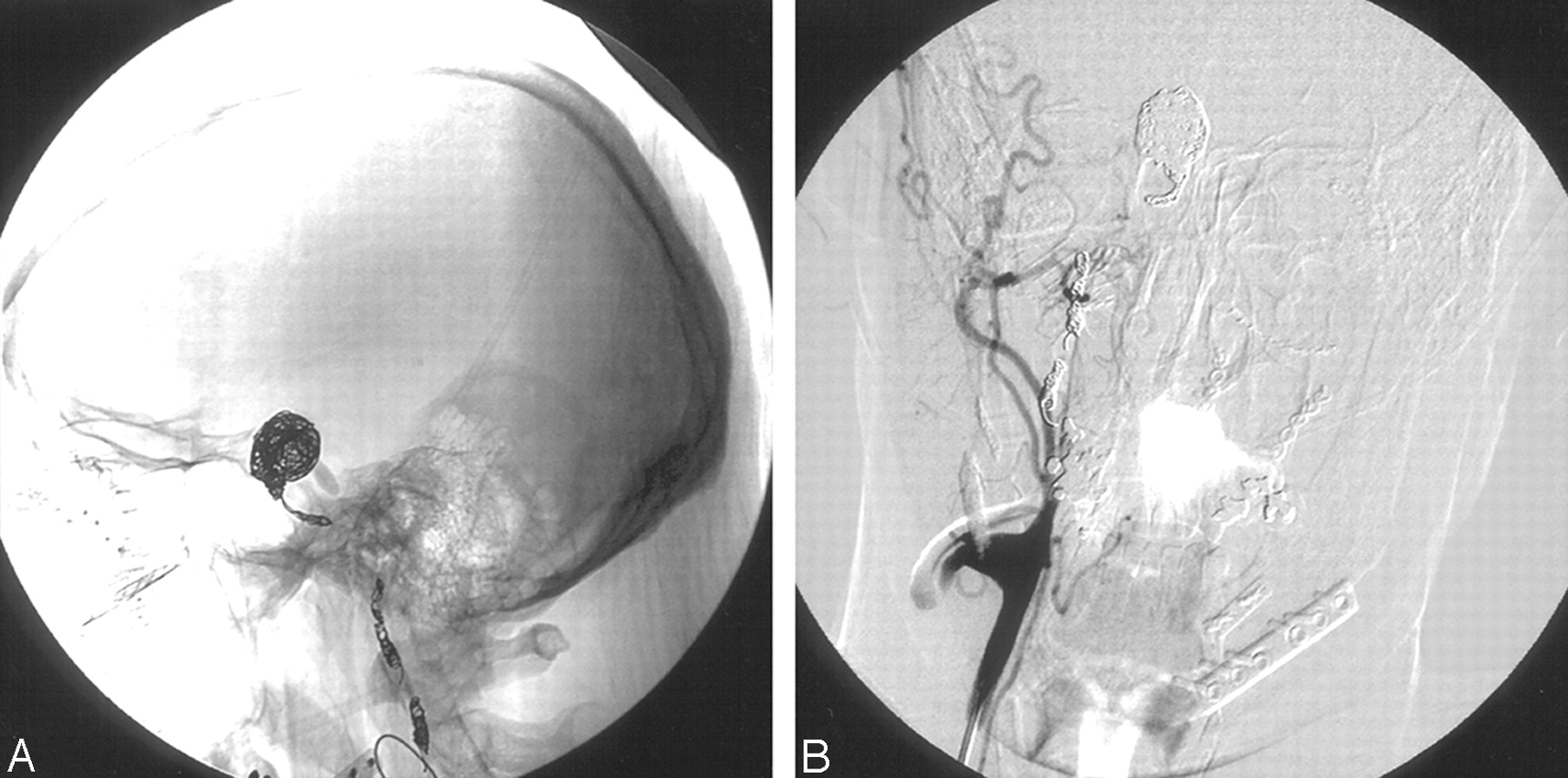
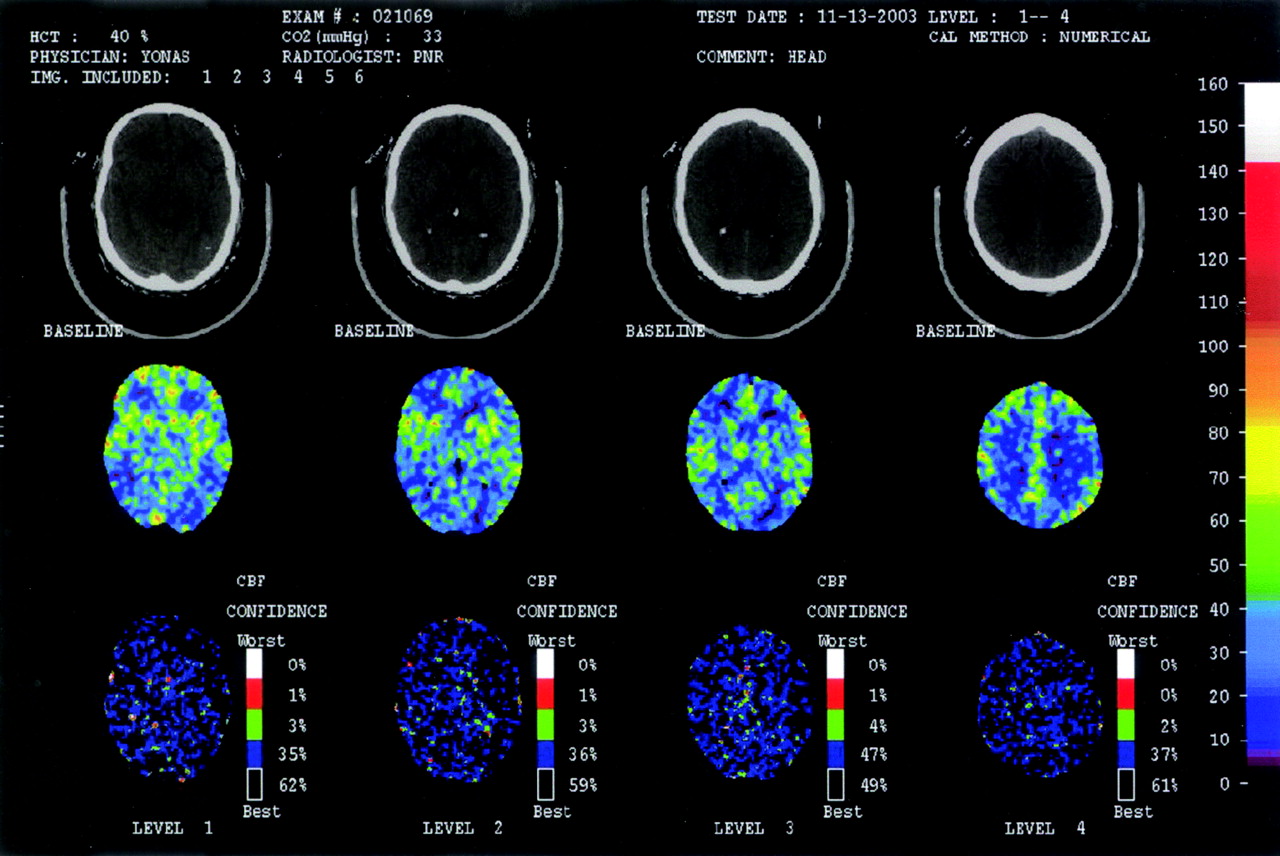
The patient presented 12 years after his initial injury with severe headache. A head CT scan and MR image demonstrated a right temporal lobe hematoma contiguous with the cavernous aneurysm (Fig 3A, -B). A cerebral arteriogram revealed the 19-mm lesion, which appeared to originate from the cavernous sinus segment of the right ICA (Fig 4A, -B). To avoid the risk of additional hemorrhage, we opted to treat the lesion endovascularly. Numerous attempts were made to cross the lesion with a microcatheter and wire so that stent arterial reconstruction/coiling could be performed. Because we were unable to cross the lesion, we opted to coil the aneurysm by using Gugliemi detachable coils (GDC [Target Therapeutics-Boston Scientific, Fremont, Calif]) and to occlude the proximal ICA by using fibered 0.018 Tornado coils (Cook, Bloomington, Ind) and 0.038 coils (Cook) (Fig 5A, -B). The patient had already demonstrated excellent left-to-right cross-filling, and though balloon test occlusion was considered, we believed the combination of cross rapid filling along with the emergent nature of the patient’s problem warranted immediate lesion obliteration. Postembolization left ICA angiography demonstrated excellent cross-filling of the right hemisphere from the left ICA contrast injection (Fig 6). Xenon blood flow after the procedure showed normal and symmetric cerebral blood flow (CBF) (Fig 7).

A, Axial T1-weighted MR image showing cavernous aneurysm with adjacent temporal lobe intraparenchymal hematoma (arrow).
B, Coronal T1-weighted MR image showing cavernous aneurysm (arrowhead) with adjacent intraparenchymal temporal lobe hematoma (arrow).

Right lateral (A) and anteroposterior (B) ICA angiograms showing 19-mm cavernous origin aneurysm.

Lateral (A) and anteroposterior (B) images showing coiled aneurysm and occluded right ICA.

Postaneurysm/right ICA occlusion left ICA angiogram showing excellent cross-filling of the right cerebral anterior circulation and no retrograde aneurysm opacification.

Xenon-CT CBF image, after right ICA sacrifice and aneurysm embolization, showing normal symmetric right and left hemispheric CBF.
Discussion
A fistula is a direct connection between an artery and vein. CCFs form secondary to abnormal communications between the carotid artery and the cavernous sinus and may present with pulsatile exophthalmos, bruit, diplopia, chemosis, pain, increased intraocular pressure, and/or erythema.1 Barrow et al2 classified CCFs as direct (type A) or dural (indirect; types B–D). Direct CCFs are high-flow lesions caused by traumatic or aneurysmal rupture of the cavernous carotid artery into the cavernous sinus. These lesions are generally treated by using proximal vessel sacrifice, proximal and distal vessel occlusion (trapping), vessel reconstruction, and aneurysm obliteration with stents and coils or primary embolization with coils to seal the fistulous connection. In the past, detachable silicon balloons were flow-directed across the carotid tear and into the cavernous sinus, where they were inflated and released to seal the fistula. These devices, however, are no longer available, having been removed voluntarily from the market by their manufacturer, Target Therapeutics-Boston Scientific in 2003.
Intracavernous carotid artery aneurysms comprise 5% of intracranial aneurysms.3 These lesions are notable for their benign natural history and low rates of subarachnoid hemorrhage.4 Subarachnoid extension of a cavernous aneurysm can be difficult to elucidate even with MR imaging, CT, and angiography. Fundal indentation, however, has been shown to represent erosion of the aneurysm through the dural rings and into the subarachnoid space. This indentation or dural waisting has been shown at surgery to reliably identify lesions that present with a risk for intracranial hemorrhage.3,4
The case described here is interesting in that it represents an instance of intraparenchymal temporal lobe hemorrhage from a cavernous carotid origin aneurysm without associated subarachnoid hemorrhage identifiable on CT. The fact that the hemorrhage occurred 12 years after successful obliteration of a Barrow type A traumatic CCF is also notable. We do not believe the aneurysm was present at the time of the patient’s initial injury because the angiogram from 1993 failed to demonstrate an aneurysm at the time of the balloon embolization.
- Received April 7, 2005.
- Accepted after revision May 18, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.