
Abstract
Summary: There are various techniques available for percutaneous biopsy of suspected diskitis/osteomyelitis. Our technique has evolved as our experience with percutaneous vertebroplasty has grown. By using a transpedicular approach, we angle a bone biopsy needle in an exaggerated caudocranial trajectory to allow eventual access across the disk space above. This approach permits sampling of the disk space, as well as both adjacent vertebral endplates. We describe our percutaneous modified vertebroplasty approach for biopsy of suspected diskitis/osteomyelitis.
Percutaneous techniques for diagnosis of spine infections include fine-needle aspiration or large-caliber core biopsy. These procedures can be performed under fluoroscopic or CT guidance. Access to the involved disk space can be obtained from a lateral diskogram approach or an exaggerated oblique transpedicular approach similar to that employed for vertebroplasty procedures. The lateral diskogram approach often limits sampling of the adjacent vertebrae if involved. Furthermore, such an approach requires avoidance of the exiting nerves, which can be injured if larger caliber biopsy needles are used. We describe a technique using an exaggerated oblique vertebroplasty approach that allows sampling of the intervertebral disk space, as well as both vertebral endplates adjacent to the involved disk.
Technique
Representative Case.
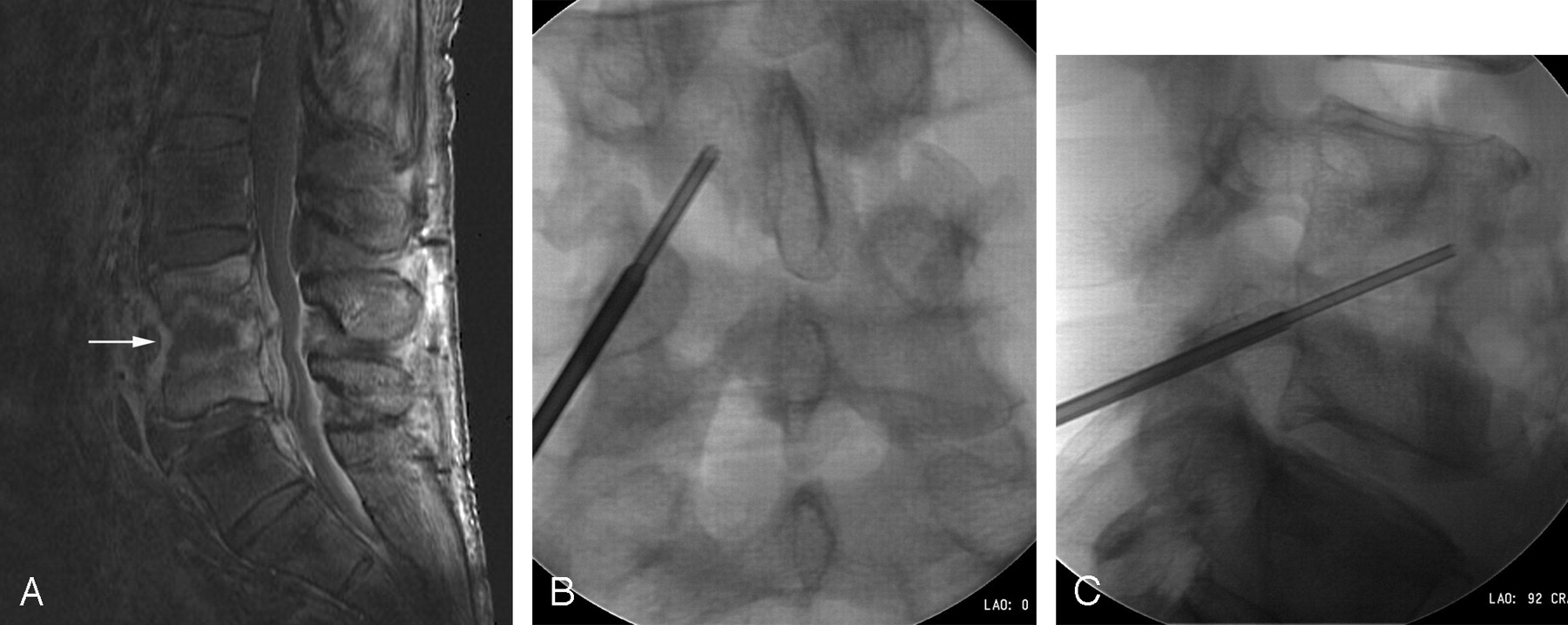
A 72-year-old woman with diabetes mellitus was evaluated for percutaneous biopsy of a suspected L4–5 disk space infection. Eight months before presentation, the patient had undergone an L4–5 diskectomy for a disk herniation. She had been doing well but developed recurrent back pain and lower extremity radiculopathy 3 days before admission. A contrast-enhanced MR imaging of the lumbar spine demonstrated an epidural abscess and evidence for diskitis/osteomyelitis at the L4–5 level (Fig 1A). Of note, the patient was afebrile at the time of diagnosis.

A, Sagittal contrast-enhanced T1-weighted MR imaging with fat-saturation demonstrates an epidural abscess and diskitis/osteomyelitis at the L4–5 level.
B, Anteroposterior image demonstrates the 11- and 14-gauge needles traversing the left L5 pedicle, L4–5 disk space, and inferior L4 endplate.
C, Lateral image shows the transdiskal placement of the 14-gauge needle by using a modified vertebroplasty approach.
Procedure.
After the patient granted informed consent, she was brought to the neuroradiology department for a fluoroscopic guided biopsy of the L4–5 disk space. Before biopsy, the patient was not taking antibiotics. She was placed prone on the fluoroscopy table, and the lower back was prepared and draped in the usual sterile fashion. The procedure was performed under conscious sedation and local anesthetic was administered to the subcutaneous tissues and periosteum overlying the left L5 pedicle. By using biplane fluoroscopic guidance, an 11-gauge bone biopsy needle was placed into the left L5 pedicle with the tip positioned at the posterior margin of the vertebral body. The needle was placed with more caudal to cranial angulation than a traditional vertebroplasty approach in an attempt to provide subsequent access to the intervertebral disk and the L4 inferior endplate. A 14-gauge trephinated biopsy needle was then advanced coaxially through the 11-gauge needle. Multiple samples were obtained with the 14-gauge needle through the superior L5 and inferior L4 vertebral endplates (Figs 1B, -C). In addition, 7.5 mL of serosanguineous fluid were readily aspirated from the disk space. The needles were removed, and the patient experienced no subsequent complications. The aspirate and biopsy samples were positive for S aureus infection, and she was placed on an appropriate intravenous antibiotic regimen.
Discussion
Fine-needle aspiration of the disk space has been utilized as a diagnostic tool in cases of suspected diskitis; however, the small-caliber needles used for fine-needle aspiration generally do not allow for sampling of the adjacent vertebrae.1 Furthermore, viscous infected fluid can be difficult to aspirate, and larger needles are difficult to maneuver without injuring the exiting nerves. As a consequence, fine-needle aspiration of disk space infections frequently fails to provide an adequate sample for analysis.
As practitioners have become more facile with percutaneous vertebroplasty, the transpedicular approach used for vertebroplasty has become more common for disk space biopsies. This technique allows for larger 11-gauge bone biopsy needles to be placed into the vertebral body and coaxial aspiration can be performed. The traditional transpedicular vertebroplasty approach, however, generally places the needle in a horizontal plane, making access to the disk space and adjacent vertebral bodies impossible. To obtain improved access to the disk space and adjacent endplates, we use the modified vertebroplasty approach described above for most cases of suspected diskitis/osteomyelitis. We employ this approach whenever possible on all suspected thoracic and lumbar disk space infection biopsies. The exception is when the patient’s anatomy precludes this approach—the most common being the lumbosacral interspace, where the anatomy occasionally is such that not enough oblique cephalad angulation can be obtained to angle through the disk space. Also, in obese patients with large body habitus, we may have to utilize an alternative more direct approach because of needle length limitations.
During a 6-month period we have used this technique in 5 patients with suspected spine infections, including the case described in this report. Three of the 5 cases yielded adequate samples and isolation of an organism. In the 2 cases where an organism was not obtained, long-term antibiotic therapy had been instituted before biopsy. Therefore, a definitive diagnosis in these patients would have likely been compromised regardless of the technique employed. We have not experienced any procedure-related complications by using this transpedicular transdiskal approach. This technique is also useful in noninfectious cases where an abnormality is present in the inferior aspect of a vertebral body. The pedicle in the vertebral level below the abnormality can be entered by using the same technique and the normal disk can be traversed. As long as strict attention to sterile technique is maintained, such an approach is a safe and effective way to obtain a tissue sample.
- Received September 29, 2005.
- Accepted after revision October 4, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.