
Abstract
SUMMARY: We present a case of cerebral fat embolism (CFE) that demonstrated evidence of diffuse white matter cytotoxic edema on diffusion-weighted magnetic resonance imaging, in addition to punctate hyperintensities on T2-weighted and diffusion-weighted imaging. The case suggests that CFE represents a combination of occlusive arteriolar disease and secondary neurotoxicity.
Fat embolism syndrome (FES) is a clinical constellation that includes respiratory disability, petechial skin rash, and neurologic symptoms. It usually occurs after traumatic lower-limb long-bone fractures but may occur after rib or short-bone fractures. Cerebral fat embolism (CFE) results in variable neurologic disability, often with significant recovery. MR imaging has been shown to be the most sensitive means of diagnosing CFE, and the typical findings of multiple punctate hyperintensities on diffusion-weighted (DWI) and T2-weighted imaging have been described in the literature.1–6 The pathophysiology of CFE remains unclear, and the extent to which it represents a primary embolic occlusive or a secondary neurotoxic process is undetermined. A better understanding of the pathophysiology of the condition in turn would improve the appreciation of this condition in terms of prognosis and therapeutic intervention.
Case Report
An 18-year-old woman presented to the accident and emergency department after a high-speed collision in which the horse she was riding was hit by a car. The patient had sustained transverse, closed fractures of the midfemur bilaterally. She remained conscious, with a Glasgow Coma Score (GCS) of 15 throughout. CT images of the head and cervical spine to exclude occult injury were normal on admission. The fractures were treated with open reduction and intramedullary nail fixation on the day of admission. At the end of surgery, the patient remained unconscious with a GCS of 3 when anesthesia was stopped. She became tachypneic and hypoxic, with oxygen saturations of 92% to 93% on 60% inspired oxygen. Blood pressure was maintained throughout.
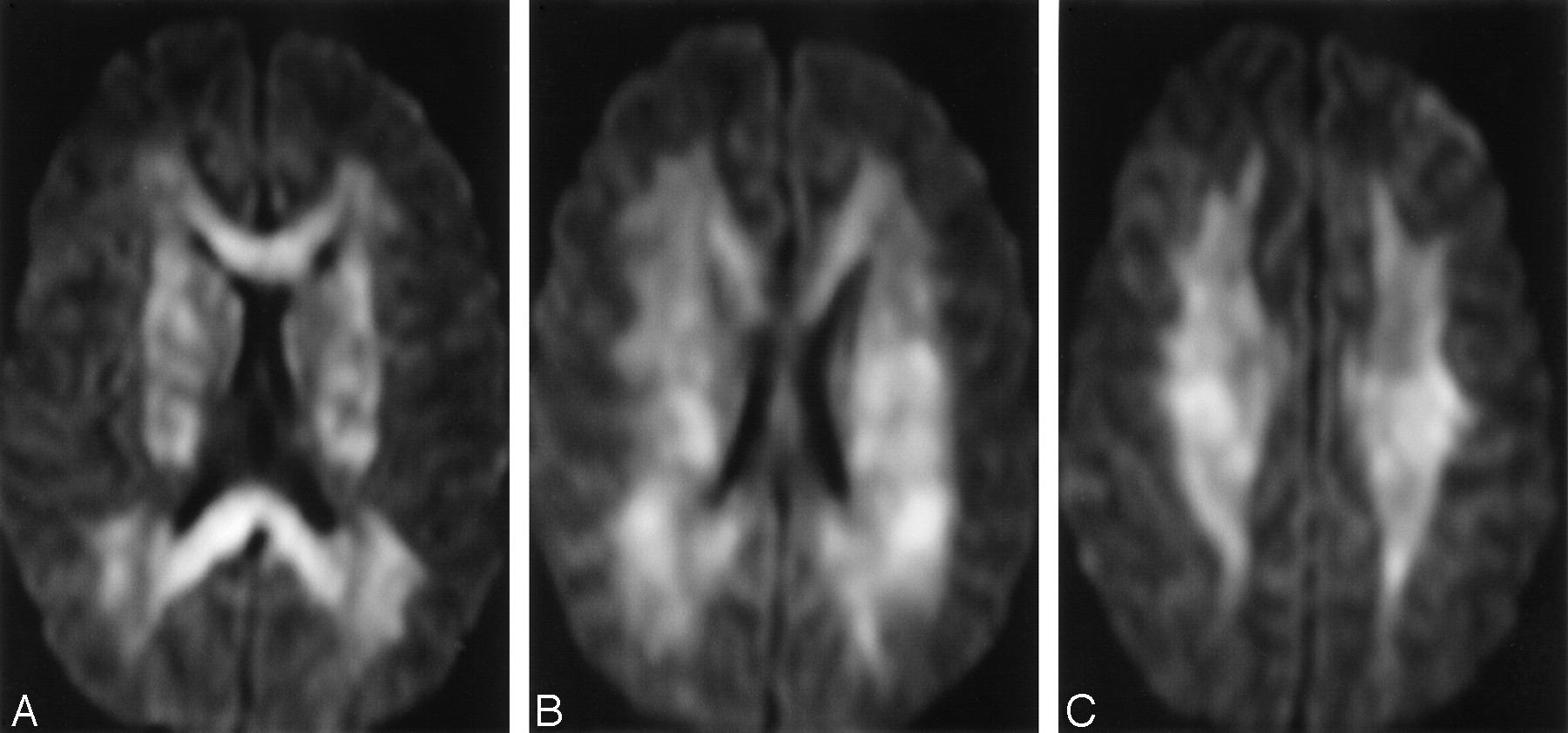
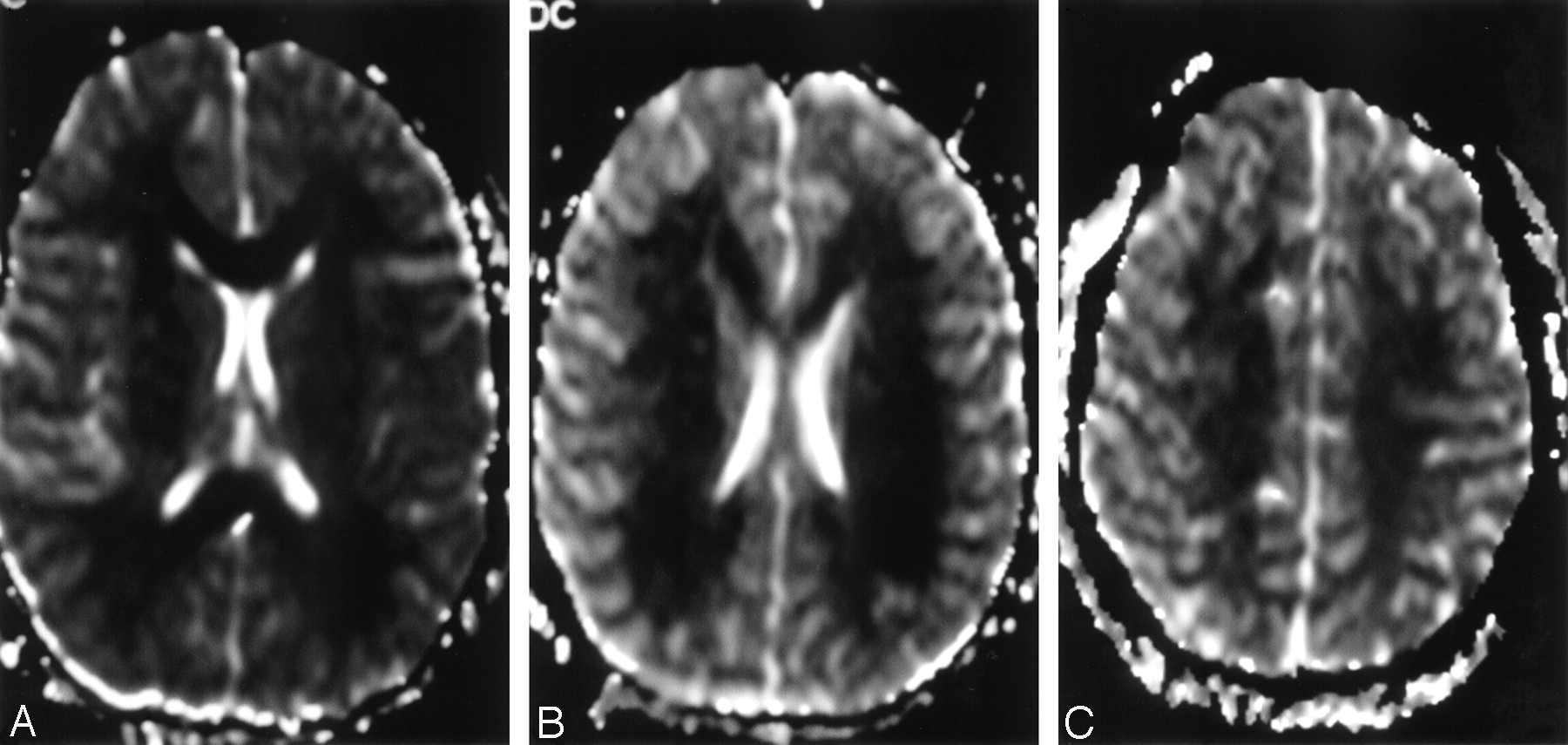
The patient was reanaesthetized and another CT scan of the head was performed. Once again, this was unremarkable. MR imaging was performed 7 days after the ictus by using axial T1, T2, T2*, fluid-attenuated inversion recovery (FLAIR) and DWI, sagittal T2, and coronal T1-weighted sequences. This demonstrated multiple punctate lesions within the basal ganglia, and cerebral white matter radiations of low intensity on T1 and high intensity on T2-weighted scans and reduced diffusivity on DWI (Fig 1 A–C), which is suggestive of CFE. In addition, there was a background of diffuse subtle white matter signal intensity abnormality, with DWI demonstrating reduced diffusivity throughout the white matter radiations, including the corpus callosum, in keeping with diffuse cerebral cytotoxic edema (Fig 2 A–C). This corresponded with extensive low signal intensity on apparent diffusion coefficient (ADC) mapping, confirming reduced diffusivity (Fig 3A–C). Gradient echo imaging demonstrated no evidence of parenchymal or extra-axial hemorrhage. Transthoracic echocardiography performed 10 days after the ictus demonstrated no intracardiac shunts, and chest radiography revealed no evidence of pulmonary arteriovenous malformations.

A–C, Axial T2-weighted images 7 days after the ictus, demonstrating punctate hyperintensities throughout the white matter, on a background of slightly increased white matter signal intensity consistent with edema.

A–C, Axial diffusion-weighted images (DWI) at corresponding sections. Marked signal intensity hyperintensity throughout the white matter demonstrates reduced diffusivity consistent with cytotoxic edema. Punctate areas of greater signal intensity correspond to the lesions shown on T2-weighted images.

A–C, Axial apparent diffusion coefficient (ADC) maps at corresponding sections, demonstrating reduced diffusivity as low signal intensity throughout the cerebral white matter.
The patient remained intubated and ventilated in the intensive treatment unit for 3 weeks. After she was weaned off ventilation, a repeat MR imaging was performed 30 days after the ictus. Axial T1, T2, T2*, DWI, sagittal T1, and coronal FLAIR sequences were performed. These showed almost complete resolution of the diffuse white matter signal intensity changes, with some residual signal intensity abnormality in the splenium of the corpus callosum. Several residual punctate lesions were present in the left centrum semiovale consistent with small lacunar infarcts (Fig 4A–I). The patient has made a slow recovery but remains in long-term neurologic rehabilitation with significant but improving deficits.

Axial T2-weighted (A–C) and diffusion-weighted images (DWI) (D–F), and apparent diffusion coefficient (ADC) maps (G–I) at corresponding sections 30 days after the ictus. Scattered punctate hyperintensities consistent with lacunar infarcts are present in areas that correlate with focal areas of signal intensity abnormality in the previous figures. The generalized mild T2 hyperintensity and reduced DWI and ADC map diffusivity have resolved.
Discussion
FES consists of the triad of acute respiratory distress with hypoxia, cutaneous petechial hemorrhages, and variable neurologic dysfunction. Secondary signs of tachycardia, pyrexia, thrombocytopenia, and anemia may also be found. The syndrome typically occurs after trauma with long-bone fractures but may also occur because of small-bone fractures and after orthopedic manipulation or interventions. It is thought that subclinical fat embolism occurs after most long-bone fractures, but clinical FES occurs in only 0.5% to 3.5% of cases. The severity is variable, and the outcomes range from complete recovery to death.7 There are several reports of isolated neurologic disorder after CFE.1,8 Clinical manifestations of CFE are protean and nonspecific and may include headache, decreased consciousness level or coma, seizures, or irritability.
The etiology of fat emboli after trauma is not clear. Two hypotheses that may coexist are mechanical, in which there is dissemination of bone marrow elements from the trauma site, and biochemical, in which elevated plasma catecholamine levels act to release lipids from body stores and destabilize circulating chylomicrons. Subsequently the action of pulmonary lipases results in the release of free fatty acids and the induction of a systemic inflammatory response.9 Microemboli may pass into the systemic circulation either via cardiac or intrapulmonary right-left shunts or directly through the pulmonary capillary bed.8 A study of orthopedic surgery in dogs has shown that fat globules of <5 μm can traverse the pulmonary micovasculature.10
MR imaging is the most sensitive technique demonstrating evidence of CFE,2–4 in particular the use of DWI sequences. In experimental CFE, DWI and T2 abnormalities have been demonstrated as early as 30 minutes after the ictus.11 The abnormalities typically described in CFE are of multiple small, nonconfluent hyperintense lesions on DWI and T2-weighted images, usually situated within the cerebral white matter and deep gray matter.1–6 The number and size of the lesions is variable but correlates with the degree of neurologic disability as measured by the GCS. These findings are thought to represent microinfarcts arising from fat emboli occluding cerebral arterioles and are more likely to result in permanent MR imaging and pathologic changes such as cyst formation and gliosis. Animal studies correlating MR imaging and pathologic findings in CFE, however, suggest that a second type of lesion occurs, demonstrating mildly increased signal intensity on DWI and T2-weighted imaging, isointensity on ADC mapping, and prominent enhancement after gadolinium administration.12 These lesions have been suggested to represent vasogenic edema as a result of blood-brain barrier dysfunction and may show complete resolution. Free fatty acids have been shown to be particularly toxic to brain tissue12 and have been proposed as the cause of this second type of lesion.
In our case, MR imaging performed 7 days after the ictus demonstrated not only multiple small, scattered T2 and DWI hyperintensities previously described in clinical and experimental cases of CFE but also a diffuse T2 hyperintensity of the cerebral white matter, including the corpus callosum, with prominent reduction in diffusivity. Reduced cerebral diffusivity is most commonly found in association with cytotoxic edema with neuronal and glial cell swelling, usually after cerebral infarction. In this case, however, the lack of cortical involvement, the symmetrical appearance, and the abnormality of the corpus callosum render emboli unlikely as a sole cause. The relatively mild pulmonary dysfunction that occurred during the ictus was not sufficient to cause global cerebral hypoxia, and a different cause must be proposed. On repeat MR imaging 30 days after the ictus, several of the punctate hyperintensities remained, in keeping with small areas of lacunar infarction, but the diffuse white matter signal intensity abnormalities had normalized, with only some residual high signal intensity in the splenium of the corpus callosum and with no persistent signal intensity changes indicative of gliosis. This is strongly suggestive of a generalized and transient neurotoxic event occurring at the time of CFE, possibly as a result of the toxic effect of local free fatty acids. This process may well be accentuated by primary blood-brain barrier breakdown as a result of arteriolar occlusion, and we believe that this case supports experimental findings of a combination of both infarction and diffuse cerebral toxicity in the pathophysiology of brain injury.11–13 In light of the severe and prolonged neurologic deficits suffered by the patient in this case, it may be that the finding of diffuse cytotoxic edema on MR imaging after CFE is associated with more severe neurotoxicity and a poorer long-term prognosis than in cases with more typical imaging findings.
References
- Received March 21, 2005.
- Accepted after revision April 29, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}