
Abstract
SUMMARY: MR imaging is typically obtained during the work-up of patients who have undergone allogeneic hematopoietic stem-cell transplant who present with unexplained change in mental status, amnesia, or seizures. Although the differential diagnosis is broad in this setting, the presence of T2 prolongation limited to the medial aspect of one or both temporal lobes with or without associated reduced water diffusion may help limit the possible diagnoses. A frequent etiology seen in this context is human herpesvirus-6 (HHV6) infection. We report the evolution of MR imaging findings and clinical course in 4 patients with limbic encephalitis probably related to HHV6.
Human herpesvirus-6 (HHV6) is a ubiquitous neurotropic virus latent in most adults. Primary infection typically occurs in the first 2 years of life. This infection usually presents as a nonspecific febrile illness sometimes associated with the characteristic rash of roseola infantum and infrequently with febrile seizures.1,2 Although rare cases of acute CNS infection have been reported in immunocompetent adults3–6 and HHV6 has been proposed as a factor in the development of multiple sclerosis,1 latent HHV6 causes no ill effects in most healthy adults. In contrast, HHV6-associated encephalitis is an emerging syndrome in transplant recipients, especially those undergoing allogeneic hematopoietic stem-cell transplantation (HSCT).7–16
We describe the serial MR imaging findings in 4 patients undergoing HSCT who exhibited acute onset of anterograde amnesia and were diagnosed with HHV6-associated encephalitis on the basis of positive CSF polymerase chain reaction (PCR) for HHV6 at the time of presentation and the lack of other identifiable cause.
Case Reports
Each of the following patients had undergone myeloablative conditioning with cyclophosphamide and total-body irradiation before transplantation and was receiving oral acyclovir for herpesvirus prophylaxis at the time of presentation.
Patient 1
This 32-year-old man with refractory stage IV Hodgkin disease was admitted on posttransplant day (PTD) 31 with altered mental status, anterograde amnesia, and seizures. CT of the head performed on admission was normal. Lumbar puncture yielded the following CSF levels: protein, 106.8 mg/dL; glucose, 76 mg/dL; 25 white blood cells (WBC)/mm3; and 47,000 red blood cells (RBC)/mm3. CSF appeared clear after centrifugation. Bacterial, mycobacterial, and fungal cultures revealed no growth. Results of a Cryptococcus neoformans latex agglutination test were negative. Rapid plasma reagin was nonreactive. CSF PCR was negative for herpes simplex virus (HSV), cytomegalovirus (CMV), varicella-zoster virus (HZV), enterovirus, and human herpesvirus 8. HHV6 DNA was detected in the CSF with the use of a qualitative PCR technique.
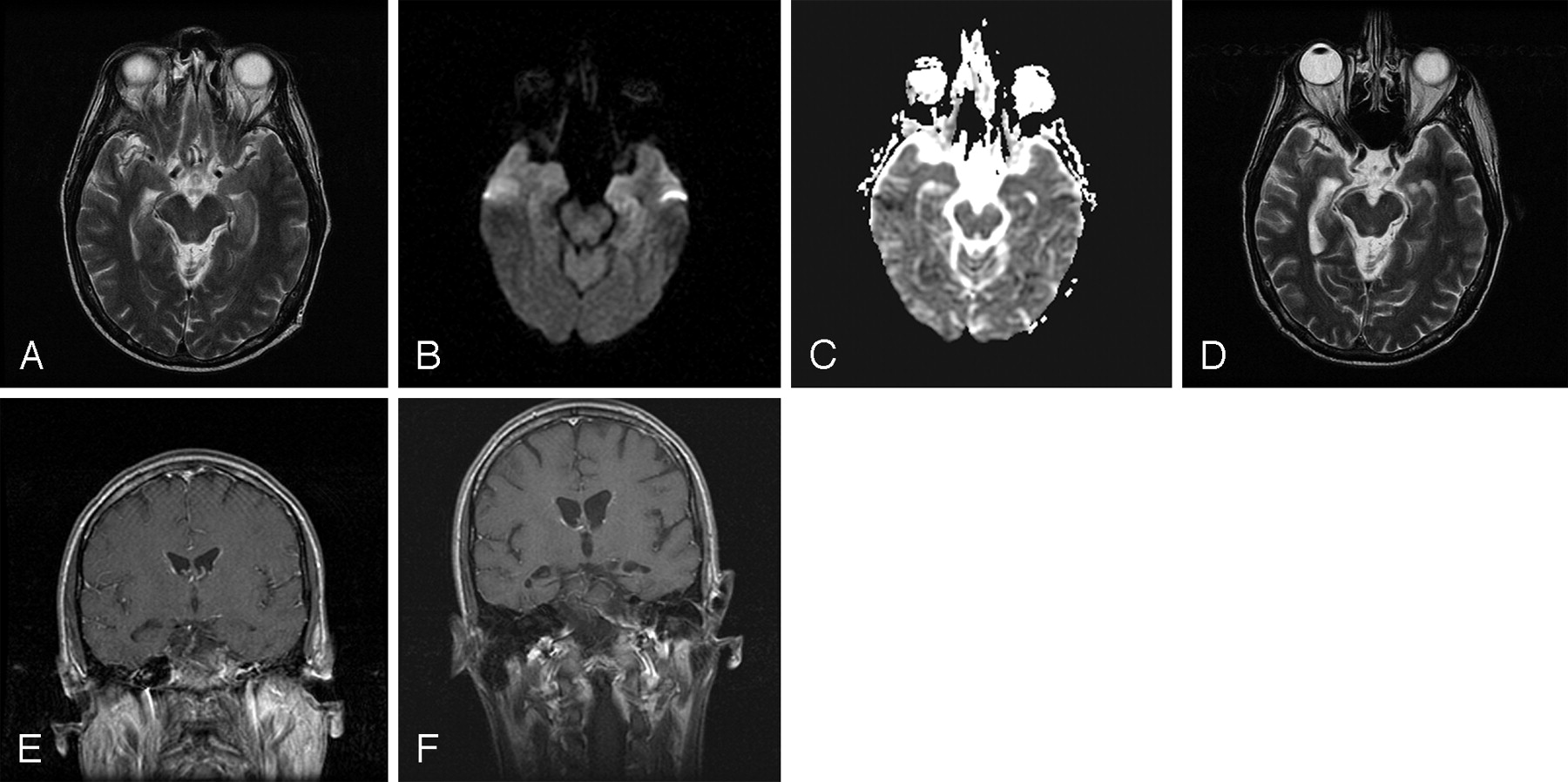
MR imaging (Fig 1) on admission demonstrated T2 prolongation within the medial aspect of both temporal lobes. Reduced water diffusion was seen in the right medial temporal lobe, demonstrated by hyperintensity on diffusion-weighted imaging (DWI) with corresponding hypointensity on the apparent diffusion coefficient (ADC) map. No abnormal enhancement or hemorrhage was present.

Patient 1. Axial fluid-attenuated inversion recovery (FLAIR) imaging (A), diffusion-weighted imaging (DWI) (B), and apparent diffusion coefficient (ADC) mapping (C) performed on admission show T2 prolongation in the medial temporal lobes with reduced diffusion on the right. Follow-up FLAIR images obtained at approximately 5 weeks (D) and 8 weeks (E) after admission show persistent T2 prolongation in the medial temporal lobes and mild volume loss more pronounced in the medial temporal lobes.
The patient received a 28-day course of the antiviral drug foscarnet (trisodium phosphonoformate). MR imaging on PTD 63 showed persistent T2 prolongation in the medial aspect of both temporal lobes. No reduced water diffusion was seen. Mild global cerebral volume loss was proportionately most pronounced in the medial temporal lobes. Repeat CSF PCR for HHV6 on PTD 64 was negative. Follow-up MR imaging on PTD 84 showed persistent medial temporal lobe signal intensity abnormality and mild cerebral volume loss. The patient had no further seizures and his mental status remained stable, although his short-term memory remained impaired. After a lengthy hospitalization to treat hepatic graft-versus-host disease and veno-occlusive disease, the patient died of bronchopneumonia and multisystem organ failure.
Patient 2
This 41-year-old man, who had a history of refractory chronic lymphocytic leukemia, presented on PTD 24 with tonic-clonic seizures. On examination, the patient was drowsy but arousable and had impaired short-term memory with preserved long-term memory. Results of head CT were normal. Lumbar puncture yielded the following CSF levels: protein, 64 mg/dL; glucose, 74 mg/dL; 7 WBC/mm3; and 138 RBC/mm3. CSF cultures showed no growth. CSF PCR was negative for HSV, HZV, and JC virus. Using a qualitative PCR technique, HHV6 DNA was detected in the CSF.
MR imaging on PTD 25 (Fig 2) showed T2 prolongation and hyperintensity on DWI in the left medial temporal lobe. ADC maps revealed that the hyperintensity in the medial temporal lobe on DWI represented T2 prolongation alone rather than reduced diffusion. No abnormal enhancement or intraparenchymal hemorrhage was seen.

Patient 2. Axial T2-weighted image (A), diffusion-weighted imaging (DWI) (B), apparent diffusion coefficient (ADC) mapping (C), and coronal postcontrast T1-weighted (E) image obtained on admission show left medial temporal T2 prolongation on fast spin-echo T2-weighted image and DWI (“T2 shine-through” effect) as confirmed by ADC map demonstrating normal diffusivity. Axial T2-weighted and coronal T1 postcontrast images at the same level performed 3 months later (D) show resolution of abnormal T2 signal intensity with interval mild volume loss, most apparent in the medial temporal lobes (F).
Treatment with foscarnet was initiated. On PTD 29, MR imaging revealed new T2 prolongation within the right medial temporal lobe and persistent T2 prolongation on the left. CSF PCR on PTD 36 was negative for HHV6. MR imaging on PTD 43 showed a slight decrease in the extent of T2 prolongation. At discharge, the patient was seizure-free, although short-term memory remained impaired. Follow-up imaging on PTD 124 showed resolution of all signal intensity abnormality and mild cerebral volume loss that was most prominent in the medial temporal lobes.
Patient 3
This 55-year-old man with myelodysplastic syndrome received a CD-8-depleted HSCT. On PTD 25, the patient was admitted because of 2 to 3 days of confusion and anterograde amnesia. Initial head CT showed no significant abnormality. Lumbar puncture yielded the following CSF levels: protein, 44.5 mg/dL; glucose, 72 mg/dL; 0 RBC/mm3; and 4 WBC/mm3. Prophylactic oral acyclovir was discontinued, and empiric treatment for herpes simplex encephalitis was initiated with high-dose intravenous acyclovir. All CSF cultures showed no growth. CSF cryptococcal antigen was negative. CSF PCR was negative for HSV types 1 and 2, JC virus, adenovirus, CMV, HZV, and Tropheryma whippleii. CSF was also negative for West Nile virus IgM, HU autoantibody, YO autoantibody, and MaTa autoantibody. Rapid plasma reagin was nonreactive. Cytology was negative for malignant cells. HHV6 DNA was detected in the CSF by using qualitative PCR.
MR imaging (Fig 3) on PTD 27 showed abnormal T2 prolongation involving the bilateral medial temporal lobes, left more than right. DWI was normal. No abnormal enhancement or intraparenchymal hemorrhage was seen.

Patient 3. Axial diffusion-weighted imaging (DWI) (A) and FLAIR imaging of the temporal lobes performed 2 days (B), 3 weeks (C), and 4 months (D) after admission demonstrate initial T2 prolongation in the medial temporal lobes with subsequent gradual normalization of signal intensity abnormality culminating in complete resolution by 4 months.
During a 2-week period, the patient’s mental status improved. PCR of CSF obtained by repeat lumbar puncture on PTD 39 was negative for HHV6. MR imaging on PTD 47 showed a decrease in the intensity and extent of T2 prolongation in the temporal lobes. Additional follow-up MR imaging on PTD 146 (approximately 4 months after admission) revealed complete resolution of the temporal lobe signal intensity abnormality.
Patient 4
This 59-year-old-man had a 7-year history of chronic lymphocytic leukemia. On PTD 32, the patient was admitted with acute mental status changes and new onset of severe amnesia, both anterograde and retrograde. Lumbar puncture revealed glucose of 71 mg/dL, protein 47.9 of mg/dL, lactate dehydrogenase at 27% of serum levels, and 16 WBC/mm3 with a differential of 1 neutrophil/mm3 and 92 lymphocytes/mm3. CSF cultures showed no growth. CSF PCR was negative for HSV, CMV, Epstein-Barr virus, enterovirus, JC virus, and HZV. HHV6 (genotype B) was detected and quantified at >999,000 viral DNA copies/mL.
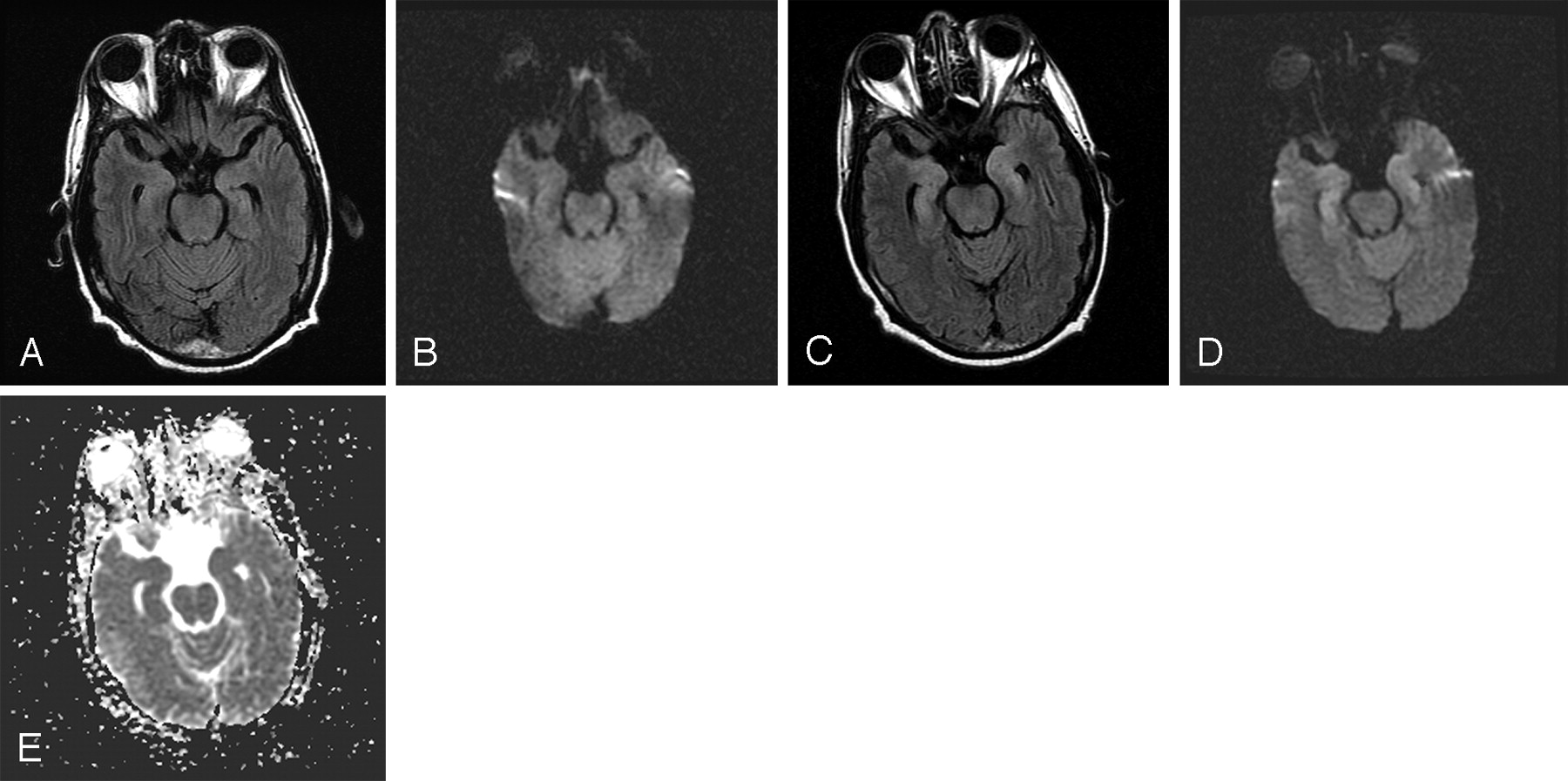
Brain MR imaging (Fig 4) showed only mild ventriculomegaly and periventricular, subcortical, and pontine signal intensity abnormality, which was thought most likely to represent chronic microangiopathy. After the PCR results became available, empiric ganciclovir was discontinued and foscarnet was started. Repeat brain MR imaging on PTD 37 demonstrated bilateral mild symmetric T2 prolongation within the medial temporal lobes. DWI showed bilateral hyperintensity in the medial temporal lobes, but ADC maps demonstrated this to represent T2 shine-through effect rather than reduced diffusion. No abnormal enhancement or intraparenchymal hemorrhage was seen.

Patient 4. Axial FLAIR image (A) and diffusion-weighted imaging (DWI) (B) through the temporal lobes obtained on admission show no medial temporal lobe abnormality. Axial FLAIR image (C), DWI (D), and apparent diffusion coefficient (ADC) mapping (E) obtained 5 days later revealed new medial temporal T2 prolongation both on FLAIR and diffusion-weighted images. ADC map demonstrates normal diffusivity.
During foscarnet treatment, the patient’s mental status and short-term memory improved dramatically. Follow-up MR imaging on PTD 43 showed no significant change. PCR of CSF obtained from a repeat lumbar puncture on the same day demonstrated a large decrease in the HHV6 DNA CSF titer to a level below the threshold of quantitation of the assay (<1000 HHV6 DNA copies/mL). Over the ensuing 3 months, the patient’s memory slowly improved but did not return completely to baseline. HHV6 DNA was undetectable on follow-up quantitative CSF PCR 3 and 4 months after presentation. Further imaging follow-up has not been performed.
Discussion
Patients undergoing HSCT tend to have complex management issues because of their underlying disease and required immunosuppressive regimens. When these patients present with encephalopathic symptoms, such as a change in mental status, drowsiness, or short-term memory loss, the differential diagnosis is broad, including direct drug effects, electrolyte abnormalities and other metabolic derangements, intracranial hemorrhage related to thrombocytopenia, immunosuppressant-related hyperperfusion encephalopathy, autoimmune paraneoplastic demyelinating and other syndromes, as well as numerous infectious etiologies.
Imaging evidence of encephalitis involving one or both hippocampi and variably involving adjacent medial temporal lobe structures of the limbic system, including amygdalae and parahippocampal gyri (“limbic encephalitis”), should help narrow the differential diagnosis. In addition to HHV6 encephalitis, other infectious etiologies of limbic encephalitis to be considered include HSV types 1 and 2, HZV, and neurosyphilis. HSV, like HHV6, has a predilection for the temporal lobes and may show similar imaging characteristics, especially early in the course of infection. HZV, a member of the Herpesviridae family, has also been detected in limbic encephalitis.17 In HSCT patients, acyclovir is universally used to prevent HSV and HZV infection or reactivation. Neurosyphilis has also been described as a rare mimicker of herpes infection18, 19 producing bilateral medial temporal lobe T2 prolongation. In addition, paraneoplastic limbic encephalitis associated with various autoantibodies has been reported,20 and at least one case was described in a patient with non-Hodgkin lymphoma after HSCT.21 Limbic encephalitis with similar MR imaging findings has also been described in systemic lupus erythematosis.22 Finally, seizure edema may show transient T2 prolongation and reduced water diffusion in the medial temporal lobes.23
Numerous reports have implicated HHV6, which was first isolated in 1986, as a cause of encephalitis. Although more extensive areas of meningoencephalitis and myelitis have been described in immunocompetent patients, in most previously reported cases of posttransplant CNS infection associated with HHV6, signal intensity abnormality on MR imaging was either not detected or was limited to the medial temporal lobes,7–16 which is similar to the cases described here. Three of the 4 cases presented in this report demonstrated T2 prolongation in one or both medial temporal lobes on admission. The one patient who initially showed no temporal lobe signal intensity abnormality underwent follow-up MR imaging 5 days later, because of clinical suspicion and high HHV6 CSF titer, which demonstrated bilateral medial temporal lobe T2 prolongation. No evidence of abnormal enhancement or intraparenchymal hemorrhage was seen in any of the 4 patients. Although areas of abnormal hyperintensity were seen on DWI in 3 of the cases, in only a single case did the ADC map demonstrate actual reduction in water diffusivity. Because that patient also had clinically apparent seizure activity, the reduced water diffusivity may have been related to seizure rather than encephalitis per se.
The localization of the signal intensity abnormality to the medial temporal lobes correlates well with the neurologic deficit in these patients, because all 4 patients presented with signs or symptoms of limbic dysfunction, most notably anterograde amnesia. The clinical association between the medial temporal lobes and dysfunction of memory formation is well documented. In 1957, Scoville and Milner first described the inability of a patient who had undergone bilateral medial temporal lobe resection to form new long-term memories.24 Since then, dozens of studies have supported the concept that the medial temporal lobes, specifically the hippocampus and surrounding structures, are intrinsically important in the processing of declarative memory functions—ie, conscious memory for facts and events.25
Because latent infection with HHV6 is common, separating incidental detection of latent HHV6 unrelated to the patient’s acute presentation from active HHV6 infection is necessary to reliably attribute a case of encephalitis to HHV6. Although latent HHV6 may be detected in blood or brain tissue, detection of HHV6 DNA in the CSF by PCR is considered substantive evidence of active CNS infection in HSCT patients presenting with acute onset of amnesia in the first 2 months after transplantation. Clinically, CSF PCR is the most definitive test used in the evaluation of HHV6-associated encephalitis, because of the risk associated with obtaining pathology via brain biopsy. Because HHV6 DNA has occasionally been detected in CSF by PCR in patients without active encephalitis, positive CSF PCR has been described as “suggestive, but not definitive, evidence of virus encephalitis.26” Nevertheless, Wang et al.27 detected HHV6 in the CSF of only 1 of 107 (0.9%) immunocompromised patients without CNS symptoms whose CSF was probed with PCR. In view of the higher pretest probability of HHV6 encephalitis in the symptomatic HSCT population than in the asymptomatic group tested, this suggests that the false-positive rate for HHV6 CSF PCR in suspected acute HHV6 encephalitis may be quite low. Thus, it seems reasonably certain that the patients presented here did have limbic encephalitis because of HHV6 reactivation in the setting of increased immunosuppression early after HSCT. In addition, the disappearance of HHV6 from the CSF demonstrated by repeat PCR after resolution or improvement of these acute clinical symptoms supports a causal association. In 3 patients, qualitative PCR retesting of CSF no longer detected HHV6 DNA. In the fourth patient, quantitative PCR retesting showed serial reduction in HHV6 DNA from >999,000 copies/mL to below the threshold of quantitation and later to undetectable levels.
As in our patients, the clinical outcomes reported in patients with HHV6 encephalitis vary from near complete recovery to death.3–16 The resolution of acute symptoms in one case was accompanied by clearing of HHV6 DNA from the CSF and complete resolution of the MR imaging signal intensity abnormality after treatment with high-dose acyclovir. Although there is no consensus about the best antiviral treatment, if any, for HHV6-associated encephalitis, patients are usually treated with foscarnet or ganciclovir, not acyclovir.1,28 In this case the patient’s transplanted immune system may have also contributed substantially to suppression of the HHV6 infection. Symptoms in the other 3 patients improved significantly but did not completely resolve, despite clearance of HHV6 from the CSF. The extent of abnormal T2 prolongation in these patients remained unchanged or decreased in the short term. In 2 of these patients, both of whom had clinically evident seizures, follow-up MR imaging was performed 2 to 3 months after presentation. In both, MR imaging demonstrated cerebral volume loss that was disproportionately prominent in the temporal lobes. This suggests relatively severe parenchymal injury that may contribute to the persistence of their symptoms, although chronic steroid use may also be a contributory factor in this volume loss. Likewise, evidence of hippocampal volume loss has been reported at autopsy by Wainwright et al13 in one patient who had subacute hippocampal sclerosis and HHV6 positive immunostaining 30 days after presenting with HHV6-assosciated encephalitis after HSCT.
References
- Received April 18, 2005.
- Accepted after revision June 3, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}