
Article Figures & Data
Figures
- Fig 1.
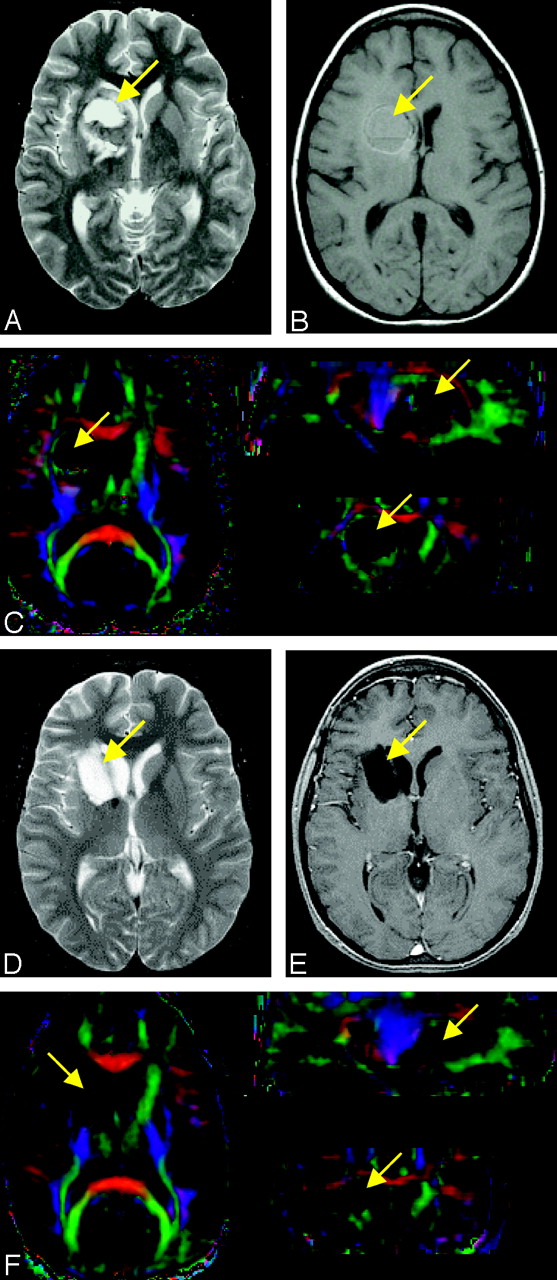
Pre- and postoperative T2-weighted (A and D), gadolinium-enhanced T1-weighted (B and E), and anisotropy-weighted color (C and F–H) maps for patient 1. The color maps allow differentiation of the WM tracts situated in the tumor vicinity: the corpus callosum, cingulum bundles, and the corona radiata. The tumor is visible as a dark region in the color maps (white arrow). Preoperatively, at least a portion of the callosal body appears interrupted by the tumor mass (C). Postoperatively (F) the tract symmetry increases but its near-midsagittal region is characterized by low anisotropy. Preoperatively, considerable deviation and low anisotropy of the left cingulum bundle are visible in axial color maps (G, yellow arrow). Postoperatively (H), the left cingulum bundle has returned to near-normal anatomic position. The left corona radiata (light-green arrowheads) is also improved after surgery, appearing more symmetric with the contralateral corona in both position and shape.
- Fig 2.
Tractograms of the cortico-spinal tracts before (A) and after (B) surgery for patient 1. The color of the fiber trajectories relates to local anisotropy, with yellow indicating high anisotropy and dark red, low anisotropy. The corresponding tract positions are shown superimposed onto axial FA maps in (C) and (D), respectively. Deviation and deformation of the ipsilateral tract in the tumor proximity are apparent in the preoperative tractogram (yellow arrow).
- Fig 3.
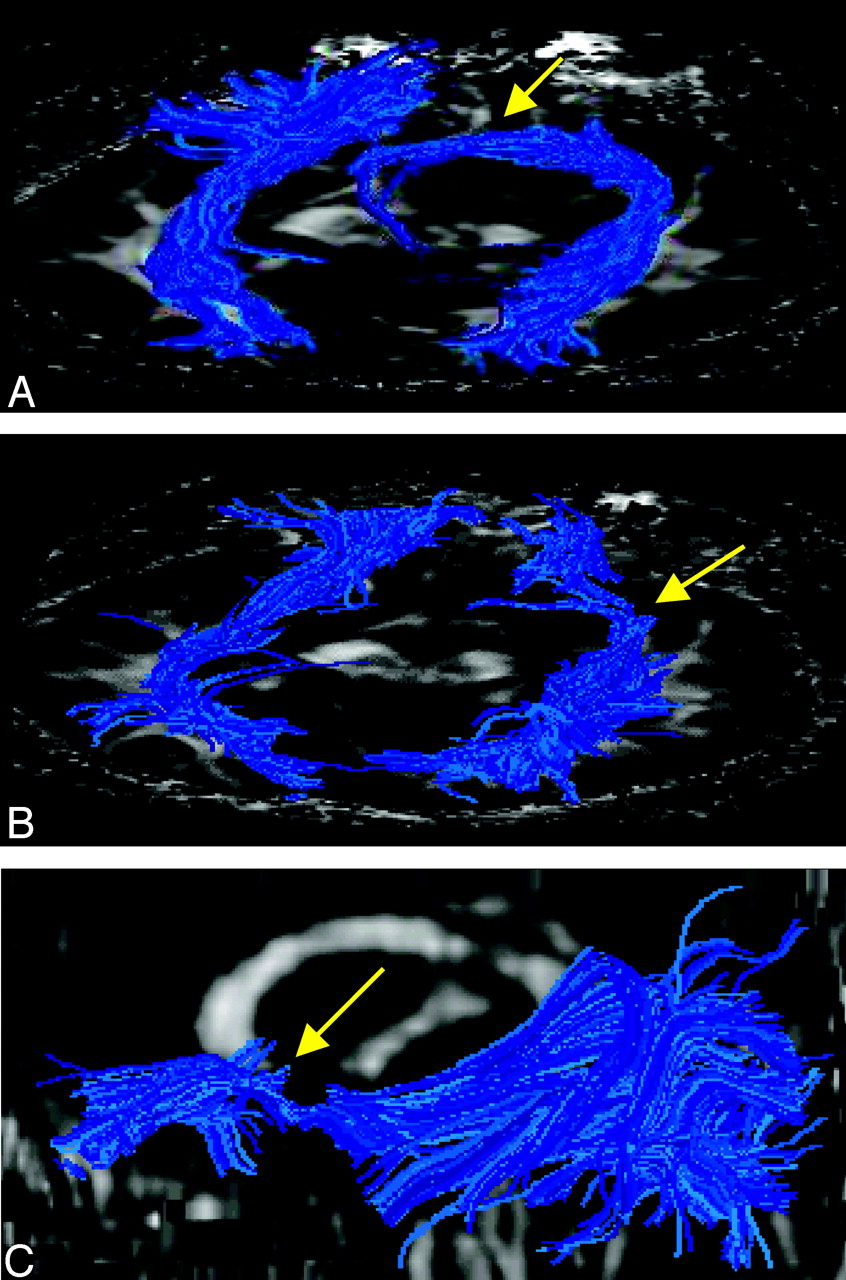
Tractograms of the corpus callosum before (A) and after (B) surgery for patient 1. The color of the trajectories indicates the local tract orientation by using the RGB convention. Preoperatively, many trajectories of the callosal body appear deviated and several appear interrrupted by the tumor mass (arrow). Postoperatively, coherent trajectories appear to cross the midline; however, abnormal trajectories also appear to be present (blue arrows). The position of the seed points in both tractograms is indicated by black dots. The postoperative tractogram of the corpus callosum was generated by using a FA threshold of 0.04.
- Fig 4.
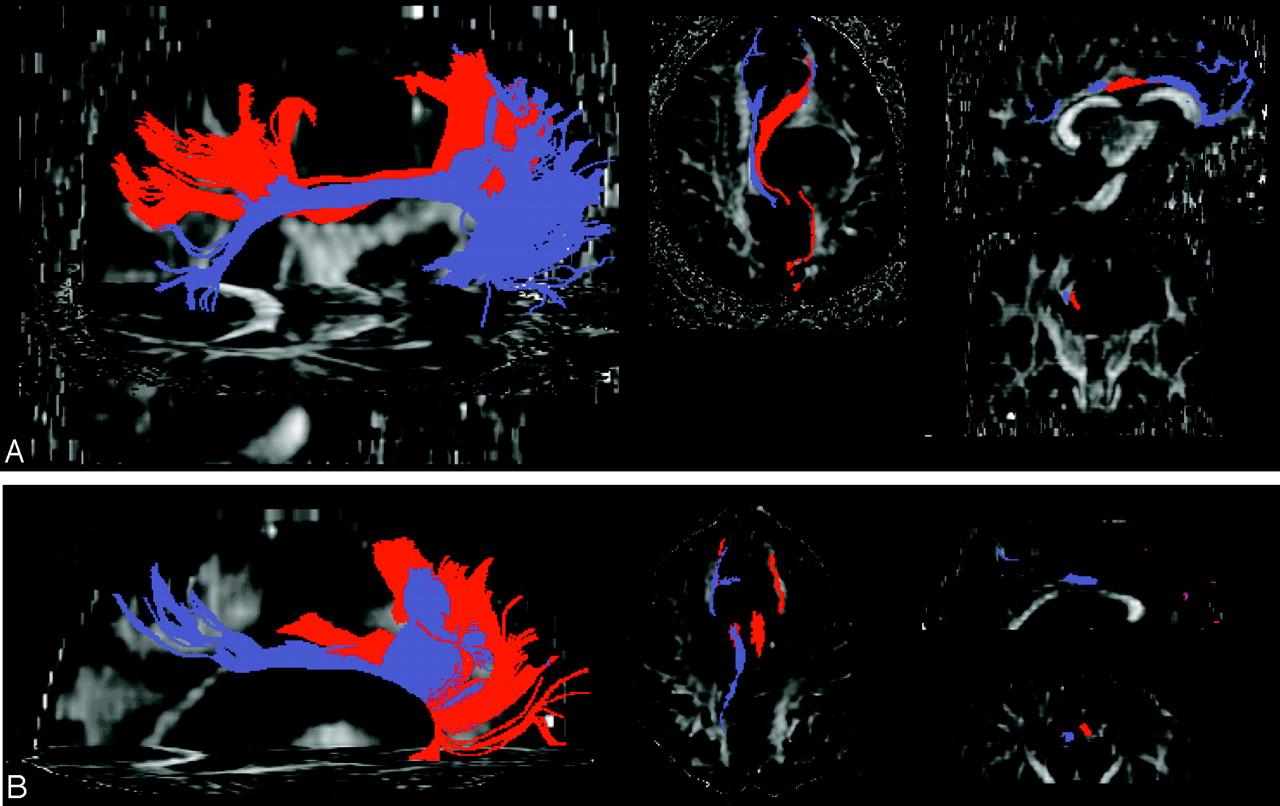
Pre- (A) and postoperative (B) tractograms of the cingulum bundles for patient 1. The tractograms were generated from a set of seeds placed in the anterior region of the tract. The relative positions of the ipsilateral (red) and contralateral (purple) bundles are labeled onto axial, sagittal, and coronal FA maps. Postoperatively, the ipsilateral bundle terminates before reaching the posterior region of the tract.
- Fig 5.
White matter tracts affected by a tumor situated in the left basal nuclei evaluated by using preoperative (A and C) and postoperative (B and D) color maps for patient 2. The postoperative images show improvement in orientation and position of tracts situated in the immediate vicinity of the tumor, such as the cortico-spinal tract (yellow arrows), and more remote tracts, such as the genu of corpus callosum (white arrows) and fornix (light-green arrows). Structures that were compressed due to the tumor mass effect, including the left thalamus (orange arrows), improved in appearance postoperatively.
- Fig 6.
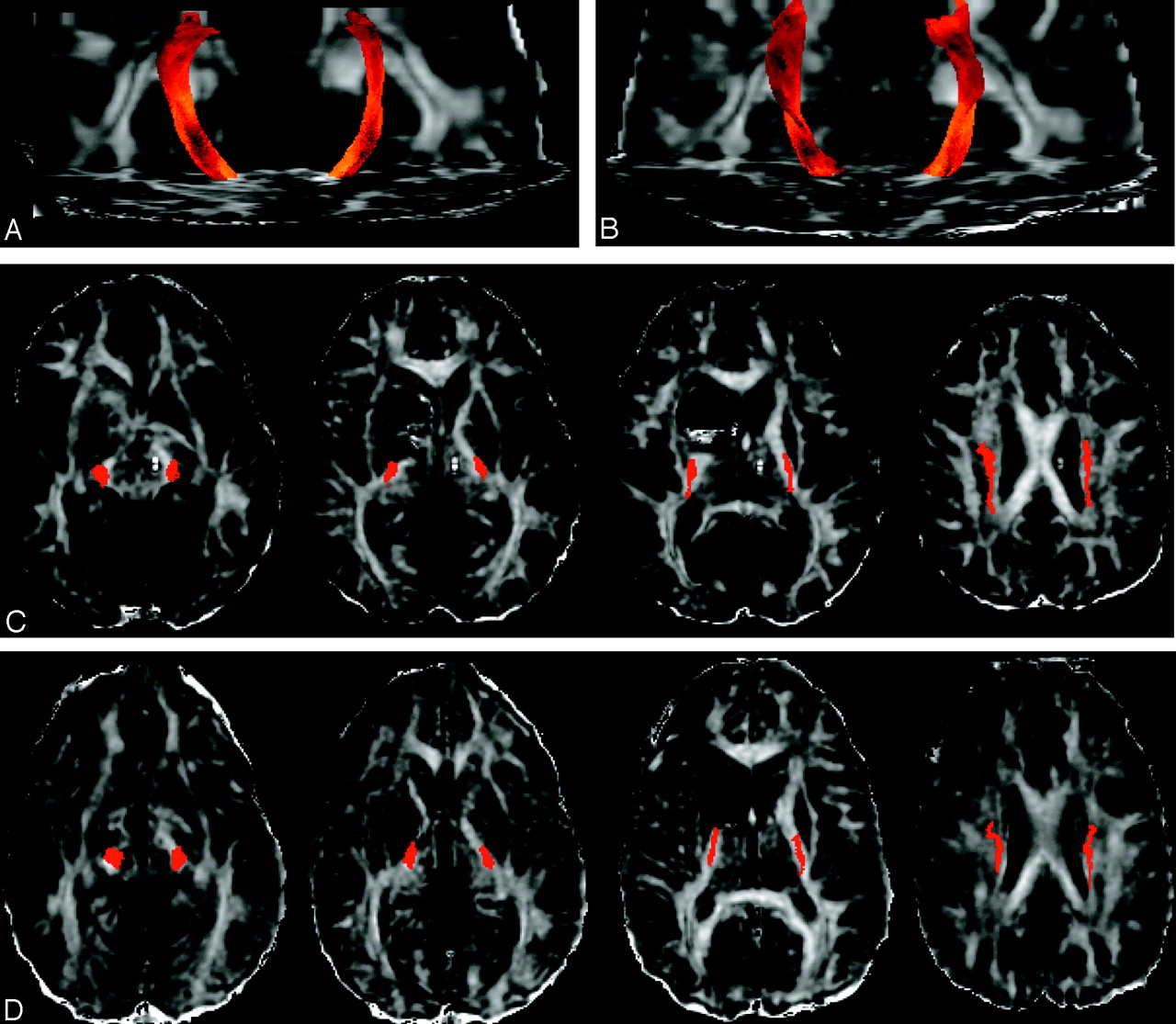
Tractograms of the corticospinal tracts superimposed onto preoperative (A and C) and postoperative (B and D) axial FA maps for patient 2. C and D, Similar axial sections were used to indicate the anatomic locations of the tracts. Coherent and uninterrupted pathways were obtained for both pre- and postoperative tractograms. Postoperatively, the ipsilateral corticospinal tract returns to near-normal anatomic position and becomes more symmetric with respect to the contralateral tract.
- Fig 7.
Pre- (A) and postoperative (B and C) tractograms of the inferior fronto-occipital fasciculi in patient 2. B and C, Two different views of the postoperative tract reconstruction. The tract appears altered before and after surgery. A set of anomalous trajectories that course toward midline before reaching the frontal cortex is observed preoperatively in the anterior portion of the tract (A, yellow arrow). Postoperatively (B and C), most of trajectories originating in either the frontal or temporal lobes appear to terminate near the resection site (yellow arrows).
- Fig 8.
Tractograms of the corticospinal tracts superimposed on preoperative (A and C) and postoperative (B and D) FA maps for patient 3. C and D, Similar axial sections were selected to indicate the anatomic locations of the tracts. Preoperatively, trajectories originating from the cerebral peduncle and reaching the motor cortex in the ipsilateral hemisphere form 1 main bundle deviated posterolaterally (yellow arrow) and several thinner bundles deviated anteromedially (white arrow). These bundles appear stretched in the tumor vicinity. The ipsilateral tract appears preserved after the surgery and positioned closer to normal anatomic position, except in the immediate vicinity of the resection.
- Fig 9.
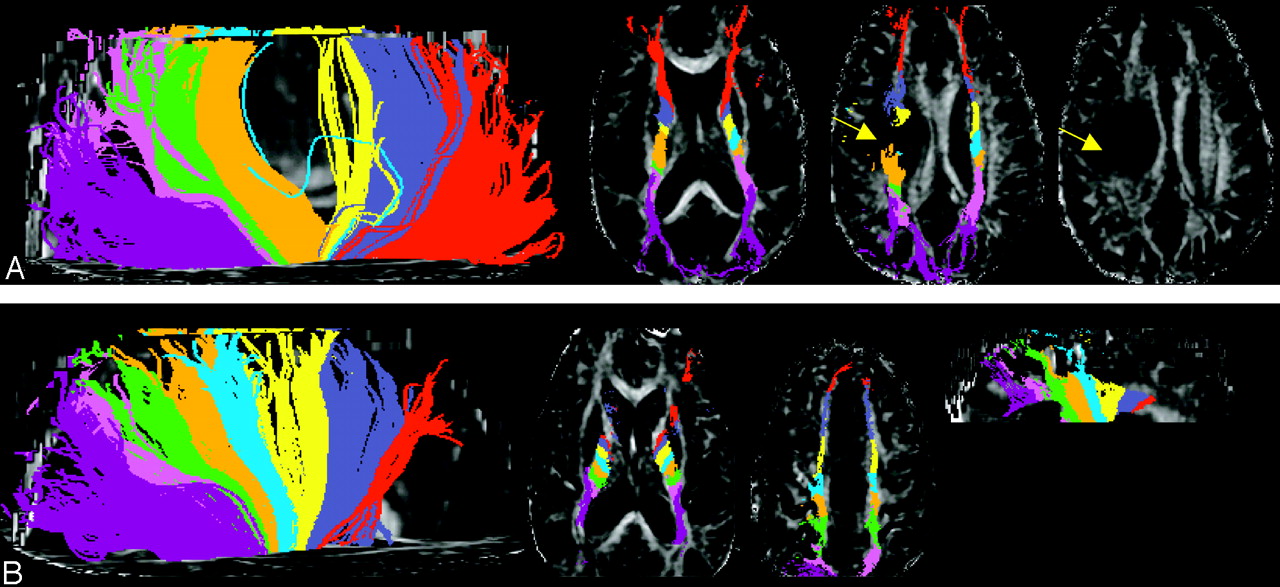
Tractograms of the projection fibers and corona radiata pre- (A) and postoperatively (B) for patient 4. An FA threshold of 0.08 was used for terminating fiber trajectories. The trajectories are color-coded according to their anteroposterior position. Their relative position is shown in axial and sagittal FA maps. Continuous trajectories were obtained even through regions of low anisotropy (arrows, A).
- Fig 10.
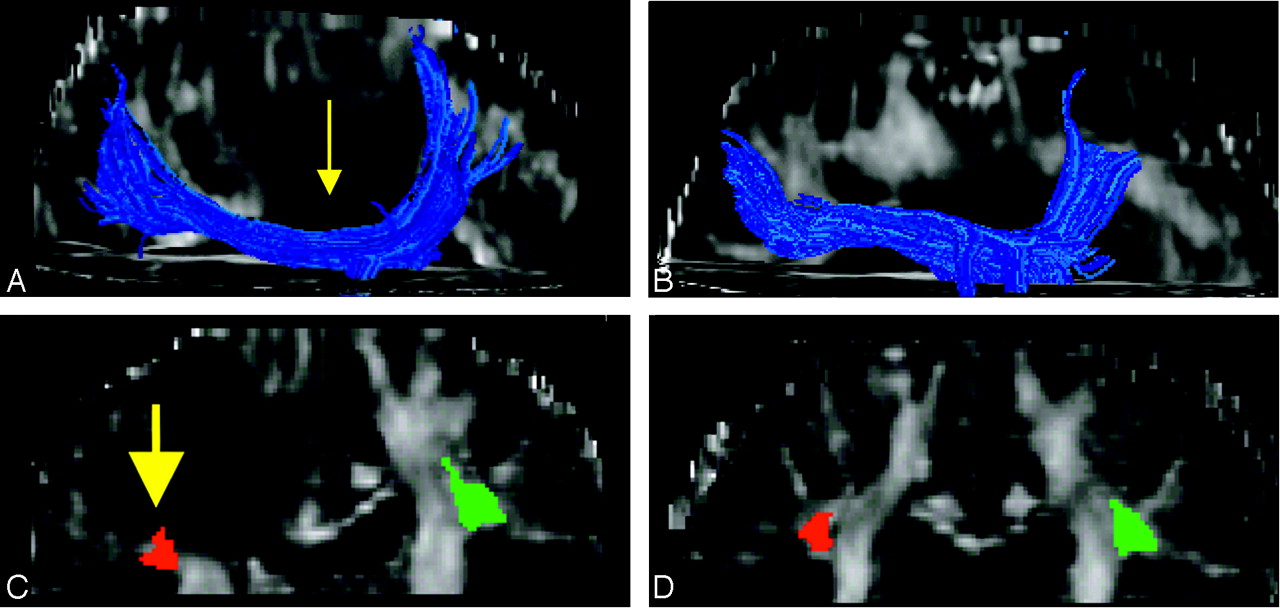
Pre- (A) and postoperative (B) tractograms of the ipsilateral superior longitudinal fasciculus for patient 4. The relative anatomic positions of the ipsilateral (red) and contralateral (green) tracts are shown superimposed onto coronal FA maps for the pre- (C) and postoperative (D) images. Preoperatively, the tract is deviated inferiorly because of the mass effect of the tumor (arrows) and consequently is positioned lower than the contralateral tract in coronal cross-section. Postoperatively, the tract appears to return to a more normal anatomic position and is positioned symmetrically with respect to the contralateral tract.
- Fig 11.
Pre- (A–C) and postoperative (D–F) axial images for patient 5: T2-weighted images (A and D), T1-weighted images (B and E), and directional color maps (C and F). Before surgery, the color images show posteromedial deviation and deformation (compression) of the posterior limb of the internal capsule (arrow, C). After surgery, the tract appears more symmetric with the contralateral tract (arrows, F) in position, cross-sectional shape, and orientation.
- Fig 12.
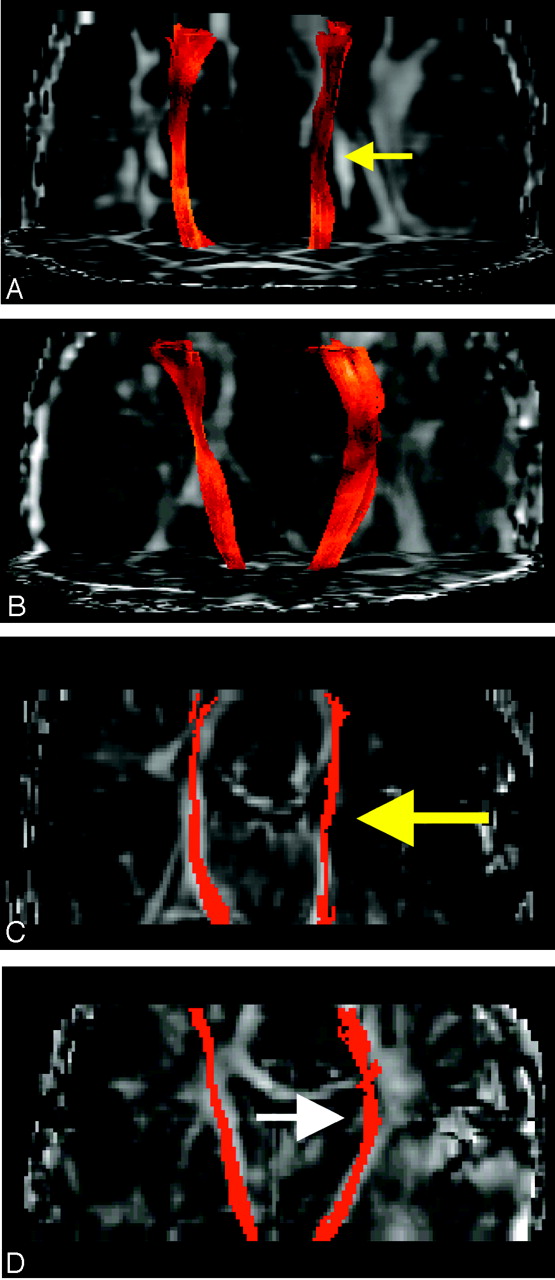
Pre- (A) and postoperative (B) tractograms of the ipsilateral and contralateral corticospinal tracts for patient 5. C and D, The corresponding tract positions in the coronal plane are shown before and after surgery, respectively. Preoperatively, the ipsilateral tract appears to be deviated medially due to the mass effect of the tumor (yellow arrows). Postoperatively, the tract returns to a more normal anatomic position (white arrow). An FA threshold of 0.15 was used to terminate trajectories for both pre- and postoperative tractograms.
- Fig 13.
Cavernoma (A–C) and resection site (D–F) positions indicated by arrows in axial T2- (A and D) and T1-weighted (B and E) images and 3-plane cross-sectional color maps (C and F) for patient 6. C, The cavernoma appears to deviate the right corticospinal tracts posteriorly and the fornix medially. The lesion appears to interrupt the anterior limb of the internal capsule and deform (compress) the external capsule and inferior fronto-occipital fasciculus. Postoperatively (F), the fornix and the corticospinal tracts return to normal anatomic positions.
- Fig 14.
Pre- (A) and postoperative (B) tractograms of the corticospinal tracts for patient 6. C and D, The corresponding anatomic locations of the tracts are shown. The tract appears to be preserved postoperatively.
- Fig 15.
Pre- (A) and postoperative (B) tractograms of the ipsilateral inferior fronto-occipital and uncinate fasciculi for patient 6. The relative positions of the pre- (C), postoperative (D), ipsilateral (yellow), and contralateral (red) tracts are shown in coronal FA cross-section. E, Approximate positions of the ipsilateral uncinate fasciculus and inferior fronto-occipital fasciculi (yellow arrows) on postoperative axial color images. Note that the 2 tracts run adjacent to each other in the frontal lobe, with the inferior fronto-occipital fasciculus situated slightly superior to the uncinate.















Tables
Patient No. Preoperative Assessment Postoperative Assesssment Notes 1 4/5 right upper/lower extremity Normal Potential involvement of motor cortex 2 4/5 right upper/lower extremity Normal —* 3 3–4/5 right upper/lower extremity Normal —* 4 4/5 left upper/lower extremity Normal Potential involvement of motor cortex 5 Normal Normal Potential involvement of motor cortex 6 Normal Normal —* * Clinical assessment of patients 2, 3, and 6 was first presented in Laundre et al.19
- TABLE 2:
Lesion effect on the adjacent white matter tracts and tract assessment after surgery
Patient No. Tract Preoperative Assessment Based on Tractography Postoperative Assessment Based on Tractography 1 Left CB Deviated and infiltrated Returns to normal position; locally interrupted Left CST Deviated and deformed Close to normal CC Interrupted and partially deviated Reduced deviations/thinned 2 Left CST Deviated Normal Left IFOF Locally interrupted Locally interrupted 3 Left CST Deviated (with splaying and deformation) Reduced deviation 4 Right CR Infiltrated and partially deviated More normal appearing; no apparent deviation; reduced region of infiltration Right CC Deviated and partially infiltrated No apparent deviation; reduced region of infiltration Right SLF Deviated and possible infiltration No apparent deviation or infiltrations of the trunk region 5 Left CST Deviated More normal position 6 Right CST Slightly deviated Normal Right IFOF/UF Minor deviations with deformation More normal position Note:—CB indicates cingulum bundle; CST, cortico-spinal tract; CC, corpus callosum; IFOF, inferior fronto-occipital fasciculus; CR, corona radiata; SLF, superior longitudinal fasciculus; UF, uncinate fasciculus.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}