
Abstract
PURPOSE: We investigated whether measurement of blood flow in the extracranial distal internal carotid artery (ICA) by transoral carotid ultrasonography (TOCU) can predict the cerebral hemodynamics and the hemodynamic effect of carotid endarterectomy (CEA) in patients with unilateral carotid stenosis.
METHODS: Forty-nine patients with unilateral ICA stenosis who underwent CEA were studied. Preoperative blood flow in the poststenotic portion of the extracranial ICA was studied by using TOCU. Regional cerebral blood flow (rCBF) and vasoreactivity to acetazolamide (VR) in the territory of the middle cerebral artery were investigated by using single-photon emission CT (SPECT) before, 2 weeks after, and 3 months after CEA.
RESULTS: Doppler flow velocities in the extracranial distal ICA measured transorally by TOCU correlated with baseline as well as postacetazolamide rCBF in the ipsilateral side (regression analysis, P < .05). Diameter and blood flow volume in the extracranial distal ICA were associated with ipsilateral postacetazolamide rCBF and VR (regression analysis, P < .05). When the patients were divided into 2 groups according to the ICA volume flow distal to a carotid stenosis, group I < 3.5 mL/s and group II > 3.5 mL/s, ipsilateral postacetazolamide rCBF in group I was significantly lower than that in group II (P = .008). Ipsilateral postacetazolamide rCBF (analysis of variance [ANOVA], P = .02) and VR (ANOVA, P = .03) significantly improved after CEA for 3 months in group I but not in group II.
CONCLUSION: TOCU can detect the decrease in poststenotic flow of the distal extracranial ICA that is indicative of impaired intracranial hemodynamics and predictive for improvement of cerebral blood flow after CEA in patients with unilateral carotid stenosis.
Carotid endarterectomy (CEA) is beneficial for the prevention of ischemic stroke in symptomatic patients.1,2 The main mechanism for the prevention of an ischemic event is probably removal of the embolic source.3 However, the elimination of cerebral hypoperfusion may additionally play a role in the prevention, because a decrease in cerebral perfusion is associated with the risk of ischemic stroke in patients with carotid stenosis.4–7 Thus, the evaluation of cerebral perfusion would be helpful also to estimate the additional benefit for the prevention of an ischemic event.
The hemodynamic change related to high-grade internal carotid artery (ICA) stenosis remains a matter of controversy.5,7–11 Moreover, data concerning the hemodynamic benefit of CEA are conflicting in the short and long term.8,12–20 These discrepancies can be explained in part by the use of different measurement methods and different time periods after the surgery. More importantly, the degree of reduction in poststenotic blood flow in addition to the presence of collateral pathways seems to cause the difference. However, little is known concerning the relationship between poststenotic flow and cerebral perfusion.
Measurement of the poststenotic portion of the ICA with duplex carotid ultrasonography by using a conventional approach is sometimes inaccurate because of inadequate insonation, intrastenotic flow increase, and turbulent flow. A recent study reported that poststenotic blood flow of the distal ICA can be measured transorally by using transoral carotid ultrasonography (TOCU) and is potentially indicative of the development of intracranial collaterals and asymmetry of cerebral blood flow (CBF) determined by single-photon emission CT (SPECT).21 In the present study, we measured the poststenotic blood flow in the extracranial distal ICA by using TOCU and investigated its relation to cerebral hemodynamics and the hemodynamic change after CEA. The aims of the present study were to elucidate whether preoperative transoral measurement of poststenotic blood flow can assess cerebral hemodynamics and predict the long-term effects of CEA on CBF in patients with carotid stenosis.
Subjects and Methods
Patients
The subjects were recruited from patients who had unilateral carotid stenosis in the origin of the ICA and underwent CEA at the National Kyushu Medical Center. Forty-nine consecutive patients who had (1) no stenosis greater than 50% in the carotid or vertebrobasilar system, as determined by the method used in the North American Symptomatic Carotid Endarterectomy Trial (NASCET), other than that of the unilateral ICA origin, and (2) no history of infarct involving cortical region or lacunar infarct larger than 1.5 cm in middle cerebral artery (MCA) territory revealed by MR imaging were selected for further analyses. Twelve patients were asymptomatic. All subjects gave informed consent to be examined by various neuroradiologic tests. All patients had a preoperative cranial CT and/or MR imaging and cerebral angiography.
Ultrasonography
Conventional carotid duplex ultrasonography was done with a color-coded duplex ultrasonographic device (Hitachi-ATL HDI 5000, Tokyo, Japan). A 5- to 10-MHz sonography beam was used for conventional carotid imaging. The lumen area at the point of greatest stenosis was measured, and the percentage stenosis was calculated by using the cross-sectional area. Although carotid stenosis was also confirmed by flow velocity measurements, the cross-sectional area was adopted for grading the severity of stenosis.
TOCU was performed by using the 5- to 9-MHz convex array transducer. The methods for TOCU have been described previously.22,23 In brief, the tip of the probe was placed on the posterior pharyngeal wall of the patient in a supine position. The properties of the extracranial distal ICA could be evaluated by the B-mode as well as by color flow imaging. The peak-systolic (PSV), end-diastolic (EDV), and time-averaged mean velocities (TMV) were also measured. The diameter and Doppler flow of the ICA was measured at the point nearest the surface of the posterior pharyngeal wall.22–24 Measurement of the diameter and Doppler flow was performed 3 times, and the median value was adopted. Blood flow was estimated by the formula diameter2 × π× TMV/4 (ml/s). An experienced examiner assessed all measurements blindly.
Angiographic Assessment
Conventional selective angiography was performed before surgery, and the findings were reviewed by a neuroradiologist blinded to all information. The degree of carotid stenosis on angiography was assessed by the NASCET method.2,25
Analysis of CBF
The cerebral circulation was examined by SPECT. SPECT was performed by using a PRISM 2000XP (2-head SPECT system, Picker, Cleveland, Ohio), and the tracer was technetium Tc99m ethyl cysteinate dimmer (Tc99m-ECD). Regional CBF (rCBF) within the territory of the MCA was quantitatively measured before and after the intravenous administration of acetazolamide (0.017 g/kg). The baseline mean CBF was measured from a graphic analysis of the time-activity curve for the brain and aortic arch obtained from radionuclide angiography by an injection of Tc99m-ECD, and the rCBF was calculated by using the Lassen correction algorithm.26,27 Vasoreactivity (VR) was estimated by postacetazolamide rCBF/baseline rCBF.
All patients underwent SPECT preoperatively (33 ± 30 days before surgery). One patient did not undergo the acetazolamide administration. In 38 patients, the test was performed 27 ± 18 days before surgery and repeated approximately 2 weeks (18 ± 4 days) and 3 months (109 ± 14 days) after the surgery.
Statistics
Linear regression analysis was performed to examine the relationship between poststenotic parameters regulating poststenotic flow and ipsilateral rCBF. One-way ANOVA comparing each period as a nominal variable with ipsilateral rCBF or VR as a continuous variable was performed. A post hoc Fisher test was done to detect the difference. Two-way repeated measures ANOVA was also done to detect the difference between time courses in patients with decreased vasoreactivity or reduction of poststenotic blood flow. The difference in the degrees of stenosis and rCBF was analyzed by using the t test. A P value less than 0.05 was considered to be significant, and between 0.05 and 0.1 to be marginally significant. The value was expressed as mean ± SD.
Results
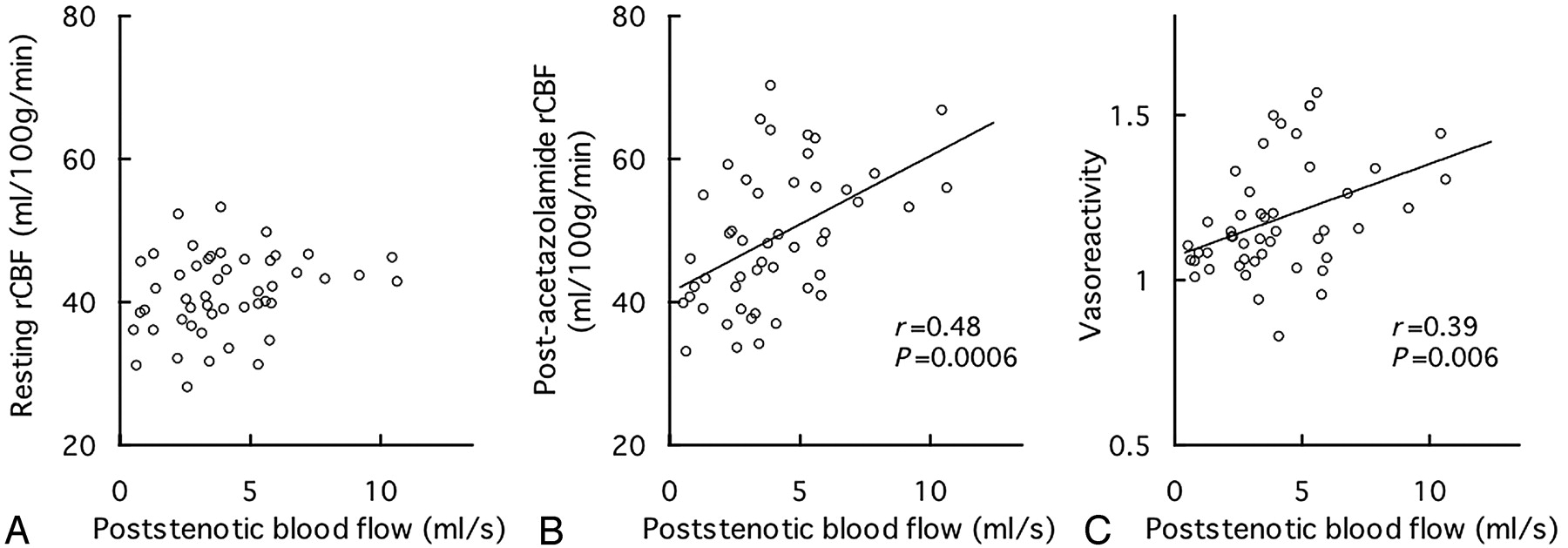
The average age of the subjects (39 men, 10 women) was 69.5 ± 6.8 (mean ± SD) years old. The average degree of stenosis evaluated by conventional ultrasonography or the NASCET method was 89 ± 10% (45%–99%) or 77 ± 14% (44%–99%), respectively. The correlation between Doppler flow parameters or the diameter of the poststenotic distal ICA and cerebral hemodynamics was investigated with regression analysis. Poststenotic flow velocities, including PSV (65.1 ± 26.6 cm/s, mean ± SD), EDV (24.3 ± 9.5 cm/s), and TMV (37.3 ± 14.4 cm/s) correlated with ipsilateral baseline rCBF (40.7 ± 5.3 mL/100 g/min) as well as ipsilateral postacetazolamide rCBF (48.3 ± 9.2 mL/100 g/min; Table 1). The diameter of the poststenotic ICA (3.6 ± 0.7 mm) and blood flow volume (4.0 ± 2.4 mL/s) in the poststenotic portion of the ICA were not significantly associated with ipsilateral baseline rCBF but with ipsilateral postacetazolamide rCBF and VR (1.19 ± 0.17; Table 1 and Fig 1).

Scatter-plot of poststenotic blood flow versus resting regional cerebral blood flow (rCBF) (ml/100 g/min, (A), postacetazolamide rCBF on the ipsilateral side (ml/100 g/min, (B), or VR (C). The abscissa indicates poststenotic flow of the extracranial distal internal carotid artery (ml/s). Lines were drawn based on the linear regression equation. Regression coefficients and P values are shown in the figures.
Correlation between poststenotic parameters of extracranial distal internal carotid artery and ipsilateral cerebral hemodynamics
The patients were divided into 2 groups with the poststenotic blood flow below (group I, n = 24) and above (group II, n = 25) 3.5 mL/s, which was the mode of values of the poststenotic flow, and subsequent analysis was done. The degrees of stenosis calculated by the cross-sectional area or NASCET method in group I (cross-sectional area, 93 ± 5%; NASCET, 85 ± 11%) were significantly higher than those in group II (cross-sectional area, 85 ± 12%, unpaired t test, P = .007; NASCET, 70 ± 14%, unpaired t test, P = .0001). Ipsilateral baseline rCBF was not different from the contralateral value in both groups, whereas postacetazolamide rCBF on the ipsilateral side was significantly lower than that on the contralateral side (Table 2). When the difference between the 2 groups was examined, baseline rCBF was similar, but the ipsilateral postacetazolamide rCBF in group I was significantly lower than that in group II (Table 2).
Preoperative rCBF in groups I and II
The time course of changes was analyzed concerning preoperative poststenotic blood flow × time interaction. The time course of the ipsilateral baseline rCBF for 3 months after CEA did not differ between the 2 groups (Fig 2A). On the other hand, the time course of changes in the ipsilateral postacetazolamide rCBF was significantly different between the 2 groups (2-way measures ANOVA, P = .03; Fig 2B). The time course of ipsilateral VR tended to differ between the 2 groups, although the difference did not reach statistical significance (2-way measures ANOVA, P = .1; Fig 2C). When the time course of changes was analyzed concerning preoperative VR × time interaction, ipsilateral postacetazolamide rCBF and VR improved after CEA only in patients with decreased VR<1.1 (2-way measures ANOVA, P = .0003 and P = .0008, respectively), whereas ipsilateral resting rCBF did not differ between the groups.

Resting regional cerebral blood flow (rCBF) (A), postacetazolamide rCBF (B), and VR (C) on the ipsilateral side before, 2 weeks after, and 3 months after carotid endarterectomy (CEA). Group I, patients with poststenotic flow <3.5 mL/s; group II, patients with poststenotic flow >3.5 mL/s. The time courses in group I (open columns in A and B; open symbols in C) and group II (hatched columns in A and B, closed symbols in C) are shown. *, P < .05; #, P < .01, analysis of variance, versus preoperative value. Post hoc analysis was done by Fisher test.
Discussion
The major findings of this study are that (1) blood flow of the extracranial distal ICA transorally measured with the use of TOCU correlated with cerebral hemodynamics and (2) long-term improvement of cerebral hemodynamics after CEA could be expected only in selected patients with decreased preoperative poststenotic flow.
Few data have been available concerning the association between cerebral circulation and poststenotic blood flow in the extracranial distal ICA. Measurement of the poststenotic portion of the ICA is sometimes inaccurate because of inadequate insonation, intrastenotic flow increase, or turbulent flow with duplex carotid ultrasonography using a conventional approach.21–23 In the present study, the poststenotic flow of the ICA in the distal extracranial portion measured by using TOCU was proportional to vasodilatory capacity. The degree of stenosis estimated by cross-sectional area measured by using conventional technique did not correlate with vasodilatory capacity in 43 patients with severe stenosis, in whom the percentage stenosis exceeded 80% (P = .2). On the other site, the poststenotic flow of the ICA measured by TOCU still showed significant correlation with VR in these patients (P = .01). Cerebral circulation is little impaired if blood flow via efficient collateral pathways compensates for the disturbed hemodynamics.4,28 However, the remarkable reduction of poststenotic flow with collapse of the artery may not be compensated for by the collateral flow, which results in hemodynamic compromise. Therefore, TOCU is more useful than conventional ultrasonographic techniques in predicting cerebral hemodynamics even in patients with severe carotid stenosis. The poststenotic blood flow measured with TOCU potentially becomes a new parameter for assessing cerebral perfusion pressure.
The impact of unilateral ICA stenosis on cerebral hemodynamics is still controversial. Previous studies disclosed that the cerebral circulation does improve after CEA in patients with both a severe stenosis and a contralateral ICA occlusion.5,9,13,14,18,19,29,30 On the other hand, in patients with unilateral carotid stenosis alone, the effects of surgical removal of the stenosis on hemodynamic changes are still controversial.10,15–17,19,20 This seems to be due mainly to patient heterogeneity in degrees of stenosis and development of intracranial collaterals.11 Recent studies have suggested that improvement of intracranial hemodynamics can be expected only in patients with decreased vasoreactivity.8,12,15–17 Although the cutoff value of VR determined by ECD SPECT for predicting misery perfusion is still not unequivocal, recent studies reported that VR determined by ECD SPECT in the controls was 1.26 ± 0.1231 and that the values of VR predicting lesions with high oxygen extraction fraction were proposed to be <1.23 or <1.07 by [123I]N-isopropyl-p-iodoamphetamine ([123I]IMP) SPECT32 or positron-emission tomography,33 respectively. Thus, VR<1.1 determined by ECD SPECT seems to indicate decreased vasodilatory capacity. In the present study, postacetazolamide rCBF and VR improved after CEA only in patients with VR < 1.1. Therefore, the time course changes after CEA in the present cases are in accordance with the previous studies.
The present study revealed that resting rCBF did not change, but vasoreactivity to acetazolamide significantly improved after CEA in patients with poststenotic flow <3.5 mL/s and that the hemodynamic benefit was sustained for 3 months after surgery in those patients. The poststenotic blood flow <3.5 mL/s indicates VR below 1.1 with a sensitivity of 71% and specificity of 61%. The decrease in poststenotic flow transorally measured with TOCU allows identification of the patients with carotid artery disease in whom intracranial hemodynamics are impaired and postoperative improvement of cerebral hemodynamics can be expected.
Various techniques have been used to assess cerebral circulation in patients with carotid stenosis, including dynamic susceptibility contrast MR imaging,8,10,19 transcranial Doppler sonography,10,12,13,17,29 MR angiography,9,18,29 MR spectroscopy,29 SPECT with technetium Tc99m-hexamethylpropyleneamine oxime or [123I]IMP.15,16,20 Compared with MR, SPECT, and conventional angiography, TOCU has the advantages of lower cost, bedside availability, noninvasiveness, absence of exposure to radiation and medium, and no significant contraindication. In this study, the test could be performed in all patients without any discomfort, such as gag reflex, by touching the pharyngeal wall gently. TOCU is also superior to the other conventional ultrasonographic methods in that it enables us to observe morphology and Doppler signals of the distal portion of the extracranial ICA without inaccuracies as a result of inadequate insonation. Therefore, this simple technique allows easier selection of the patients who will benefit in terms of cerebral hemodynamics after surgery.
In the present study, the ICA stenosis was estimated by the cross-sectional area, though the flow velocity criteria are generally used in the detection of significant carotid stenosis. Moreover, the subjects included only the patients who had unilateral carotid stenosis without major stroke and underwent the surgery in a single hospital. Thus, further studies would be required to generalize the present results to all the patients undergoing CEA.
In conclusion, TOCU provides a new, noninvasive method for the measurement of carotid circulation. It can be used for evaluation of the distal circulation and prediction of postoperative hemodynamic improvement after CEA. We hope that this simple tool will provide better understanding of cerebral hemodynamics and long-term improvement of postoperative blood flow after CEA in patients with carotid stenosis.
Acknowledgments
This study was supported by research grants for Cardiovascular Diseases (12A-2, 12C-10 and 14A-3) from the Ministry of Health, Labor and Welfare of Japan.
References
- Received July 17, 2005.
- Accepted after revision October 13, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.