
Article Figures & Data
Figures
- Fig 1.
Comparison of the signal intensity of 26 metastatic brain tumors on diffusion-weighted images. All 6 well differentiated adenocarcinomas (Well diff. AC) were classified as grade −2, −1, or 0. All 3 small-cell carcinomas (Small cell ca.) and 1 large-cell neuroendocrine carcinoma (LCNC) were graded as +2. A malignant melanoma was grade −1; all other tumors were grade 0 or +1. Poorly diff. AC, indicates poorly differentiated adenocarcinomas; Large cell ca., large cell carcinoma; SCC, squamous cell carcinoma; Papillotubular ca., papillotubular carcinoma; Mucoepidermoid ca., mucoepidermoid carcinoma; Mod. diff. AC, moderately differentiated adenocarcinoma. The signal intensity was graded on a point scale: −2 = hypointense relative to the normal-appearing white matter; −1 = isointense relative to the normal-appearing white matter; 0 = isointense relative to the normal-appearing cortical gray matter; +1 = slightly hyperintense relative to the normal-appearing cortical gray matter; and +2 = hyperintense relative to the normal-appearing cortical gray matter.
- Fig 2.
A 67-year-old man with a well differentiated adenocarcinoma from the lung.
A, T2-weighted fast spin-echo image shows a parietotemporal lesion (arrow) near the trigone of the left lateral ventricle. It is hypointense relative to the normal-appearing white matter. The CNR of the solid lesion was 12.
B, On contract-enhanced T1-weighted image, the lesion is enhanced (arrow).
C, On DWI, the lesion is hypointense relative to the normal-appearing white matter (arrow). It was graded as −2.
D, On ADC map, the nADC of the lesion was calculated as 1.95.
E, Photomicrograph of the specimen (hematoxylin-eosin stain; original magnification, 40×) shows a well-differentiated acinar structure. Tumor cellularity was calculated as 0.179.
- Fig 3.
A 41-year-old man with a poorly differentiated adenocarcinoma from the lung.
A, T2-weighted fast spin-echo image shows a left parietal subcortical lesion (arrow). It is slightly hyperintense relative to the normal-appearing white matter. The CNR of the solid lesion was 32.
B, On contract-enhanced T1-weighted image, the lesion is well enhanced (arrow).
C, On DWI, the lesion is slightly hyperintense relative to the normal-appearing cortical gray matter (arrow). It was graded as +1.
D, On ADC map, the nADC of the lesion was calculated as 1.45.
E, Photomicrograph of the specimen (hematoxylin-eosin stain; original magnification, 40×) shows higher cellularity than Fig 2E. Tumor cellularity was calculated as 0.334.
- Fig 4.
A 69-year-old man with small-cell carcinoma from the lung.
A, On T2-weighted fast spin-echo image, the solid portion of a right parietal mass lesion (arrow) is hyperintense relative to the normal-appearing white matter. The CNR of the enhancing lesion was 45.
B, On contract-enhanced T1-weighted image, the peripheral region of the lesion is enhanced (arrow).
C, On DWI, the lesion is hyperintense relative to the normal-appearing cortical gray matter (arrow). The lesion was graded as +2.
D, On ADC map, the solid lesion is slightly hyperintense. Its nADC was calculated as 0.57.
E, Photomicrograph of the specimen (hematoxylin-eosin stain; original magnification, 40×) shows high cellularity. The tumor cellularity was calculated as 0.72.
- Fig 5.
A 63-year-old man with large cell neuroendocrine carcinoma from the lung.
A, On T2-weighted fast spin-echo image, the solid portion of left occipital lesion (arrow) is hyperintense relative to the normal-appearing white matter. The CNR of the enhancing lesion was 56.
B, On contrast-enhanced T1-weighted image, the posterior part of the lesion is enhanced (arrow). There are multiple enhancing areas (arrowheads) in the left frontal lobe indicative of subacute infarction.
C, On DWI, the solid lesion is hyperintense relative to the normal-appearing cortical gray matter (arrow). The lesion was ranked as grade +2.
D, On ADC map, the solid lesion is hypointense; its nADC was calculated as 1.04.
E, Photomicrograph of the specimen (hematoxylin-eosin stain; original magnification, 40×) shows high cellularity. The tumor cellularity was calculated as 0.51.
- Fig 6.
Comparison of the nADC value and CNR on T2-weighted images of 26 metastatic brain tumors of different histologic types. Most well differentiated adenocarcinomas (Well diff. AC) are distributed at high nADC and low CNR. Of the 3 small-cell carcinomas (Small cell ca.), 2 exhibit nADC values below 1.0. The large-cell neuroendocrine carcinoma (LCNC) manifests low nADC value and high CNR. Poorly differentiated adenocarcinoma (Poorly diff. AC), papillotubular carcinoma (Papillotubular ca.), sarcoma, and malignant melanoma (Melanoma) also exhibit low nADC values. Large cell ca. indicates large cell carcinoma; SCC, squamous cell carcinoma; Mucoepidermoid ca.: mucoepidermoid carcinoma; Mod. diff. AC, moderately differentiated adenocarcinoma.
- Fig 7.
Comparison of the signal intensity of 13 histologically confirmed brain lesions on diffusion-weighted images. All 4 well differentiated adenocarcinomas (Well diff. AC) were graded as −2 or −1, and 2 poorly differentiated adenocarcinomas (Poorly diff. AC) as +1. One small-cell carcinoma (Small cell ca.) and 1 large-cell neuroendocrine carcinoma (LCNC) were both graded as +2. The other lesions were graded as 0 or +1. The signal intensity was graded on 5-point scale as described in Fig 1. Large cell ca., large cell carcinoma; SCC, squamous cell carcinoma; Papillotubular ca., papillotubular indicates carcinoma; Mucoepidermoid ca., mucoepidermoid carcinoma.
- Fig 8.
Comparison of the nADC value and CNR on T2-weighted images of 13 histologically confirmed brain lesions. Most well differentiated adenocarcinomas (Well diff. AC) are distributed at high nADC and low CNR. One small-cell carcinoma (Small cell ca.) and 1 large cell neuroendocrine carcinoma (LCNC) were distributed at low nADC and high CNR. Poorly diff. AC indicates poorly differentiated adenocarcinoma; Large cell ca., large cell carcinoma; SCC, squamous cell carcinoma; Mucoepidermoid ca., mucoepidermoid carcinoma; Papillotubular ca., papillotubular carcinoma.
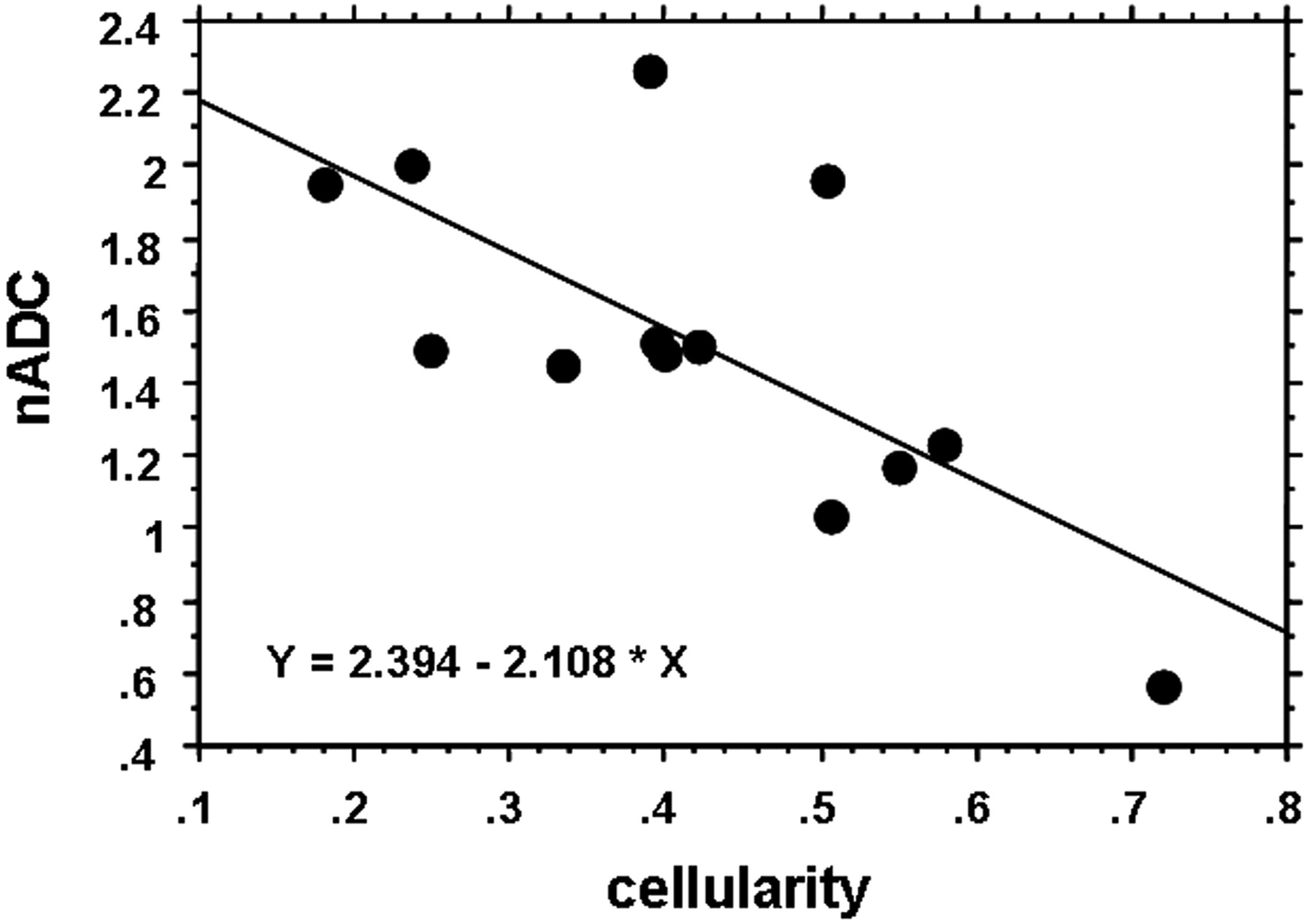
- Fig 9.
Relationship between nADC and tumor cellularity. The nADC value inversely correlated well with tumor cellularity (r = −0.70, P = .0059).









Tables
Histopathology of Primary Lesion No. of Lesions Primary Site (No. of Sites) Adenocarcinoma 13 Well differentiated 6 Lung (4), ovary (1), uterus (1) Moderately differentiated 1 Lung (1) Poorly differentiated 6 Lung (6) Small-cell carcinoma 3 Lung (3) Large-cell carcinoma 2 Lung (2) Squamous cell carcinoma 2 Esophagus (2) Papillotubular carcinoma 2 Breast (2) LCNC 1 Lung (1) Mucoepidermoid carcinoma 1 Lung (1) Sarcoma 1 Synovium (1) Malignant melanoma 1 Skin (1) Note:—LCNC indicates large-cell neuroendocrine carcinoma.
Histopathology of Brain Lesion No. of Lesions Primary site (No. of Sites) Adenocarcinoma 6 Well differentiated 4 Lung (3), ovary (1) Poorly differentiated 2 Lung (2) Squamous cell carcinoma 2 Esophagus (2) Small-cell carcinoma 1 Lung (1) Large-cell carcinoma 1 Lung (1) Papillotubular carcinoma 1 Breast (1) LCNC 1 Lung (1) Mucoepidermoid carcinoma 1 Lung (1) Note:—LCNC indicates large-cell neuroendocrine carcinoma.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Associations Between ADC Texture Analysis and Tumor Infiltrating Lymphocytes in Brain Metastasis - A Preliminary Study
- Sequential Apparent Diffusion Coefficient for Assessment of Tumor Progression in Patients with Low-Grade Glioma
- Diffusion-Weighted Imaging of Brain Metastasis from Lung Cancer: Correlation of MRI Parameters with the Histologic Type and Gene Mutation Status
- A Multiparametric Model for Mapping Cellularity in Glioblastoma Using Radiographically Localized Biopsies
- Differentiating Hemangioblastomas from Brain Metastases Using Diffusion-Weighted Imaging and Dynamic Susceptibility Contrast-Enhanced Perfusion-Weighted MR Imaging
- The efficacy of diffusion weighted imaging and apparent diffusion coefficients mapping for liver metastasis of colonic adenocarcinomas
- Parametric Response Mapping of Apparent Diffusion Coefficient as an Imaging Biomarker to Distinguish Pseudoprogression from True Tumor Progression in Peptide-Based Vaccine Therapy for Pediatric Diffuse Intrinsic Pontine Glioma
- "Dazed and diffused": making sense of diffusion abnormalities in neurologic pathologies
- Correlation of 18F-FDG Uptake with Apparent Diffusion Coefficient Ratio Measured on Standard and High b Value Diffusion MRI in Head and Neck Cancer
- Differentiation between Glioblastomas, Solitary Brain Metastases, and Primary Cerebral Lymphomas Using Diffusion Tensor and Dynamic Susceptibility Contrast-Enhanced MR Imaging
- Diffusion-weighted magnetic resonance imaging for monitoring prostate cancer progression in patients managed by active surveillance
- Imaging Immune Response In vivo: Cytolytic Action of Genetically Altered T Cells Directed to Glioblastoma Multiforme