
Abstract
SUMMARY:A 48-year-old woman, with right-sided proptosis and decreased visual acuity, presented with acute left sensorimotor deficit. Recent ischemia in the right posterior watershed area was found on CT and MR imaging, as well as a right-sided medial sphenoid wing meningioma causing high-grade stenotic encasement of the cavernous portion of the right internal carotid artery. Because the patient was symptomatic and complete resection of the meningioma was impossible, the stenosis was successfully treated with a balloon-expanding stent.
Encasement and stenosis of the internal carotid artery at the level of the cavernous sinus are known features in cases of meningiomas involving the cavernous sinus, caused by invasion of the vessel wall.1 This finding, however, can make complete resection difficult or even impossible, and an increased risk of cerebral ischemia exists when elective carotid sacrifice is required.1,2
Endovascular stent placement is a promising technique for symptomatic atherosclerotic intracranial carotid artery stenosis,3,4 but no reports exist on nonatherosclerotic intracranial carotid artery stenosis. We report a case of a symptomatic high-grade stenosis of the cavernous portion of the internal carotid artery due to a medial sphenoid wing meningioma treated by endovascular stent placement.
Case Report
A 48-year-old woman who had a painful proptosis of the right eye for 4 months and ipsilateral decreased visual acuity was admitted to the department of neurology with an acute left sensorimotoric deficit. She had no relevant medical history, but work-up of the patient during her hospitalization demonstrated a lesion in the right breast with a diameter of 1 cm. Needle core biopsy of this mass revealed an invasive ductal adenocarcinoma.
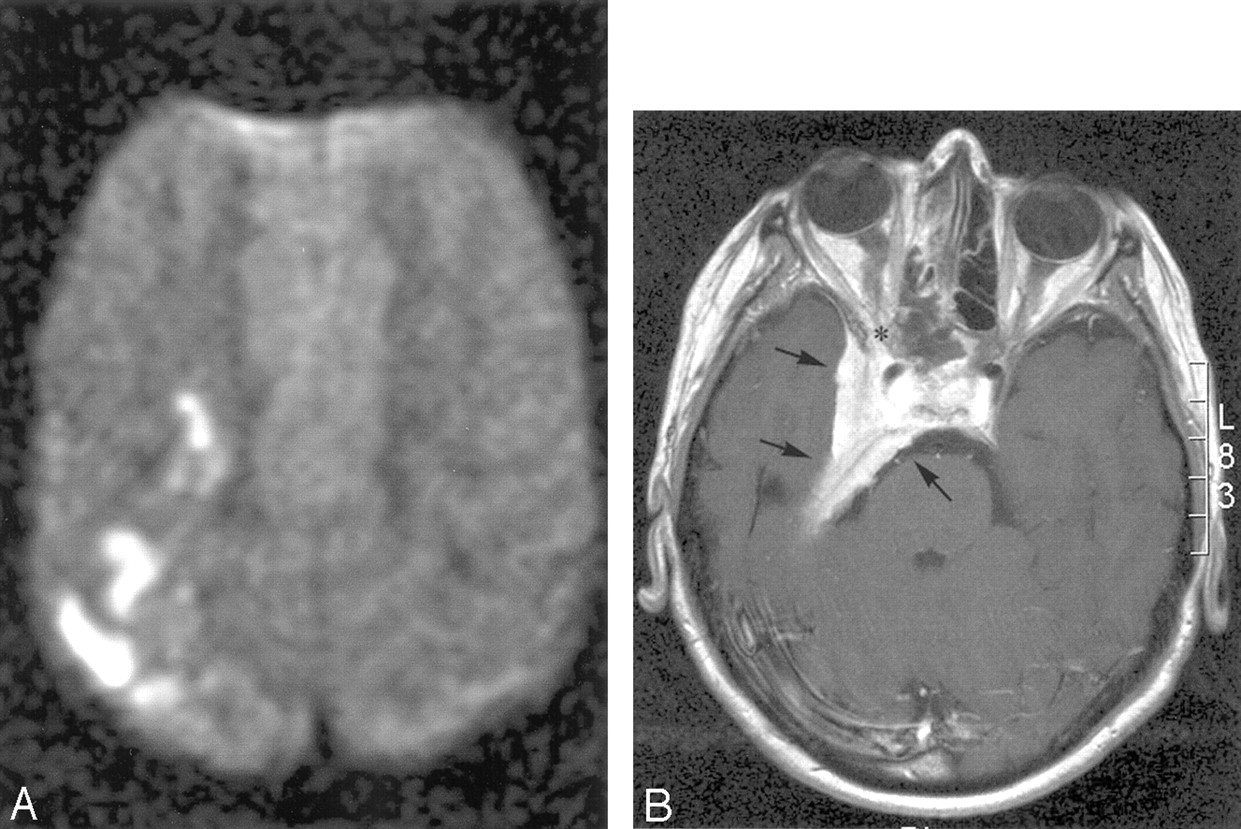
CT and MR imaging of the brain were performed to further investigate her left-sided hemiparesis. Besides a recent infarction zone (Fig 1A) in the right posterior watershed area, these examinations showed a hypervascular mass mainly at the posterolateral wall of the right sphenoid sinus and right cavernous sinus, extending into the superior orbital fissure and orbital apex (Fig 1B). There was also extension along the tentorium cerebelli at the right side as well as in the sellar and suprasellar region. The adjacent bony structures were slightly thickened and sclerotic. Encasement of the cavernous portion of the right internal carotid artery by the lesion was also shown. These findings were highly suggestive of a right-sided medial sphenoid wing meningioma, with encasement of the right internal carotid artery at the level of the cavernous sinus and a recent cerebral infarct in the right posterior watershed area, probably due to hypoperfusion because of this high-grade internal carotid artery stenosis, though a thromboembolic cause could not be fully excluded.

A, Axial diffusion-weighted image shows hyperintense zones in the right posterior watershed area compatible with recent infarction. B, Axial contrast-enhanced T1-weighted image demonstrates clearly the enhancing mass at the posterolateral wall of the right sphenoid sinus and cavernous sinus, with extension into the superior orbital fissure and orbital apex.
Anatomopathologic examination of a specimen of the mass obtained by transnasal endoscopic biopsy confirmed the radiologic findings and demonstrated a meningotheliomatous meningioma, WHO grade I.
Selective angiography of the right internal carotid artery confirmed the high-grade stenosis of the cavernous portion of the right internal carotid artery (Fig 2A). A hypervascular blush, compatible with the meningioma, was also seen, with feeding arteries from an intracavernous branch of the right internal carotid artery and from branches of the right external carotid artery. Selective angiography of the left internal carotid artery during manual occlusion of the right common carotid artery showed that the circle of Willis was insufficiently functional for parent-vessel occlusion of the right common carotid artery.

A, Right carotid angiogram shows a high-grade stenosis of the cavernous portion of the right internal carotid artery. B and C, Control angiograms obtained after the procedure show good position of the stent with good re-expansion of the stenosis.
Because this was a symptomatic stenosis of the internal carotid artery and complete resection of the meningioma was not possible (certainly not without sacrificing the internal carotid artery), we chose to perform endovascular stent placement.
The endovascular procedure was started with the patient under global anesthesia. After positioning a 7F guiding catheter (Guider Softip, Boston Scientific, Paris, France) in the right common carotid artery via femoral approach, a 0.014-inch guidewire was placed in the right medial cerebral artery, passing the stenosis. Over this guidewire, a balloon catheter (12 × 2.5 mm) (Sprinter RX, Medtronic Vascular, Santa Rosa, Calif) was used to dilate the stenosis before stent positioning. Then a balloon-expanding coronary stent (Driver Over-the-Wire coronary stent, Medtronic Vascular) was placed at the stenosis of the cavernous portion of the right internal carotid artery. This stent had a length of 12 mm and, fully expanded, a diameter of 4 mm, and the pressure used to deploy the stent was 12 atm.
Control angiography showed good position of the stent with good re-expansion of the previously mentioned stenosis (Fig 2B, -C). During the procedure, a bolus of 5000 IU of heparin was administrated intravenously.
No new neurologic events occurred during or after the procedure. Therapeutic doses of low-molecular-weight heparin (2 × 60 mg SC) were started after the procedure.
Two weeks later the patient underwent a large excision of the right-sided breast tumor and the ipsilateral axillary lymph nodes. Low-molecular-weight heparin was then reduced to half the dose because of a postoperative hematoma and was stopped after 6 months. Postoperative radiation and hormonal treatment were needed as adjuvant therapy for the malignant breast tumor. During her stay at the hospital, the patient had incomplete recovery of her left-sided hemiparesis.
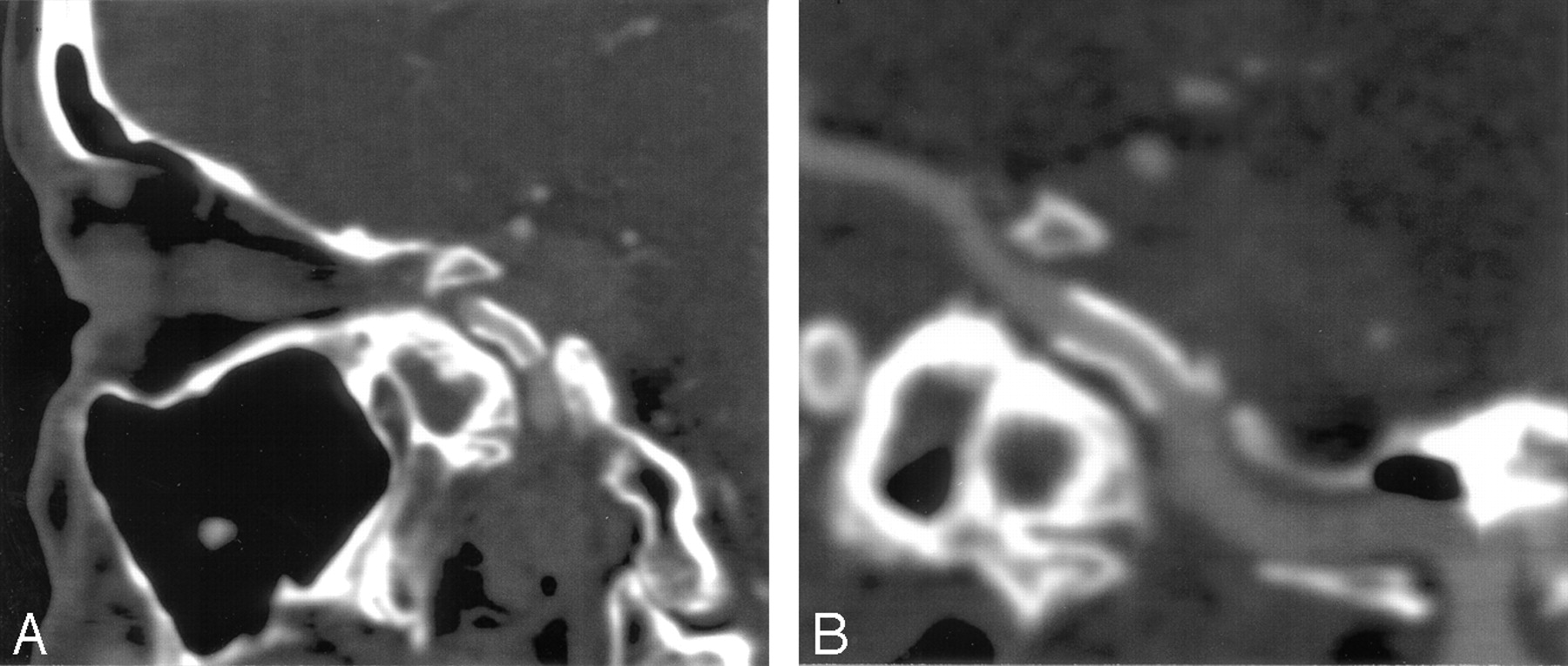
A follow-up CT scan of the carotid arteries after 12 months demonstrated good position of the patent stent without any neointimal hyperplasia (Fig 3A, -B). Clinically the visual disturbances did not deteriorate further, and the left-sided paresis recovered partially, with residual motor deficit of the fourth and fifth finger.

CT scans with (A) sagittal and (B) curved multiplanar reconstruction demonstrate good patency of the stent in the cavernous portion of the right internal carotid artery without any neointimal hyperplasia.
A neurosurgical intervention with decompression of the optic nerves and postoperative radiation therapy has been discussed with the patient and will be planned after patient consent.
Discussion
Meningiomas are the most common type of brain tumor involving the cavernous sinus.1 When they extend into the medial cavernous compartment, encasement of the cavernous segment of the internal carotid artery can be expected.5 In such cases, total resection of the tumor is not possible without sacrificing the carotid artery (with or without reconstruction) or without major risk for ocular cranial nerve deficit/palsy.5
Although encasement and narrowing of the internal carotid artery are commonly seen in meningiomas involving the cavernous sinus, with a reported incidence varying between 8% and 100%,1,5 neurologic deficits and cerebral ischemia due to reduced cerebral perfusion pressure by the stenosis are very rare. Because this implicates an insufficiently developed circle of Willis, sacrificing the internal carotid artery, either operatively or by endovascular parent vessel occlusion, would be impossible. Therefore an alternative therapy was required. Surgical reconstruction, such as an extracranial-intracranial bypass, is a possibility, but this has not been found to be beneficial in cases of intracranial stenosis.4
Percutaneous transluminal angioplasty (PTA) is another strategy, but besides issues of recoil and dissection, PTA in atherosclerotic stenosis of the petrous or cavernous portion of the internal carotid artery appears to be less effective in relation to the restenosis rate compared with stent placement.6
Intracranial stent placement can be a safe and feasible alternative therapy in patients with symptomatic atherosclerotic lesions of intracranial arteries, with an overall postprocedural stroke occurrence of less than 8%.3,4 One of the major problems in intracranial stent placement is deployment of the stent at the correct position, especially in tortuous carotid arteries. This was overcome in our patient by using a flexible coronary stent with a low profile, which can be exactly delivered because it is a balloon-expanding stent. Another problem of an intracranial stent is the possible risk of neointimal hyperplasia during follow-up. A common scheme of postprocedural antiplatelet therapy is clopidogrel (75 mg daily) for at least 4 weeks, followed by lifetime aspirin regimen (at least 100 mg daily).3 Although we usually use this scheme for intravascular stent procedures, it was not used in our patient because she still required breast surgery. As an alternative, we chose an anticoagulant therapy with therapeutic doses of low-molecular-weight heparin, which we had to reduce because of a postoperative hematoma. Low-molecular-weight heparin was stopped after 6 months. Nevertheless, the stent remained patent without any signs of neointimal hyperplasia after 1 year.
In summary, an unusual case of a symptomatic encasement of an internal carotid artery by a medial sphenoid wing meningioma is described. Minimally invasive treatment, consisting of percutaneous placement of a stent, led to radiologic restoration of normal blood flow after a 12-month follow-up period, and no recurrent ischemic symptoms were seen during the same follow-up period.
- Received June 27, 2005.
- Accepted after revision August 21, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}