
Abstract
SUMMARY: Inserting a guiding catheter into a tortuous artery for neurointerventional procedures can be difficult. In our technique, the carotid artery is manually compressed to stabilize and/or straighten the inserted wire before advancing the guiding catheter. Although this technique is not risk-free and care must be taken to avoid vascular injury by excessive compression, it is useful for the insertion of a guiding catheter into the carotid artery.
The insertion of a guiding catheter system into the desired arterial site is the first, and one of the most important, steps for successful endovascular treatment. Here we present our “carotid-compression technique” that facilitates insertion of the guiding catheter into the tortuous carotid artery.
Technical Considerations
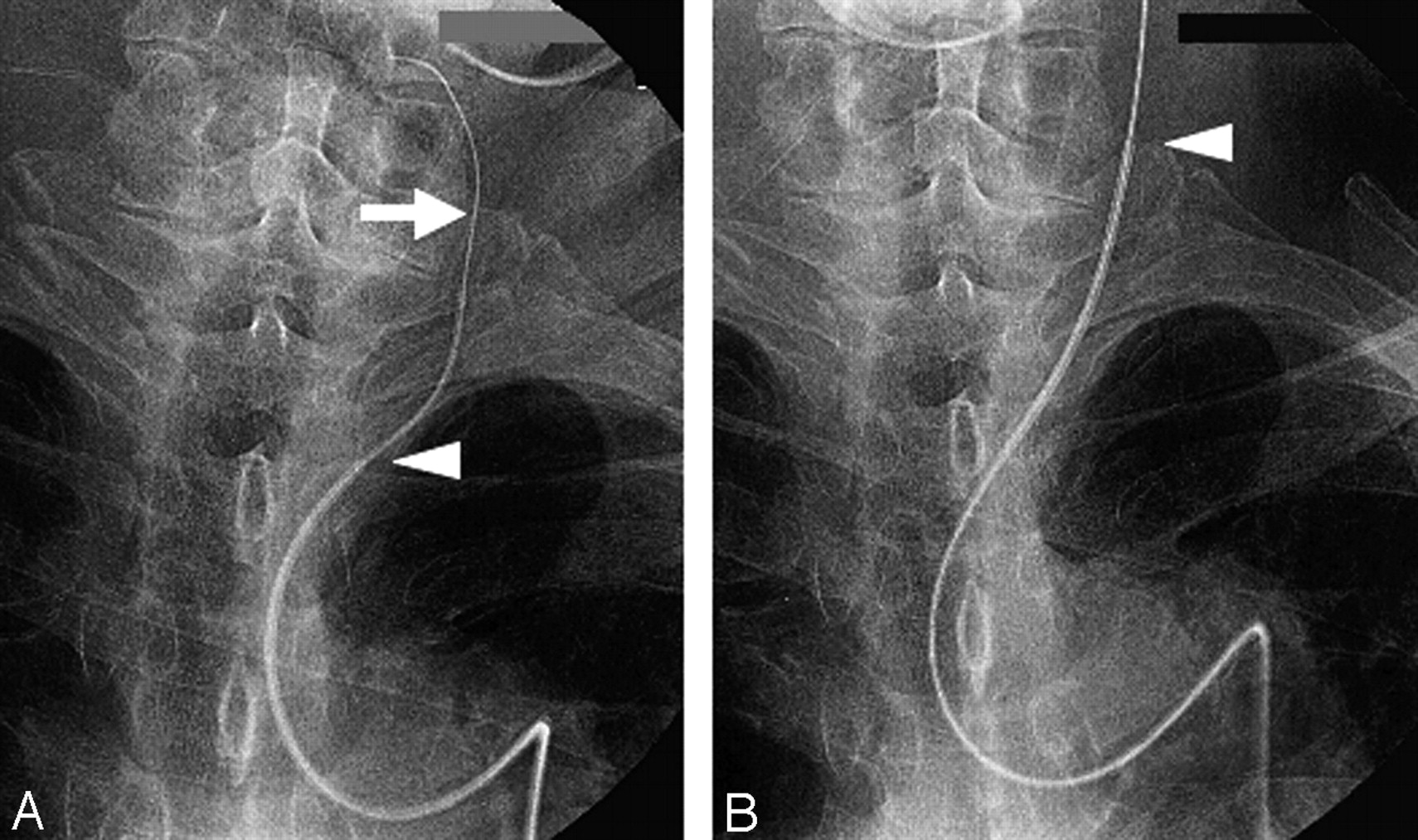
In patients with severe atherosclerosis, the insertion of a catheter, especially a guiding catheter, into the common carotid artery (CCA) can be difficult. Anatomic factors such as a long distance between the origin of the carotid artery and the top of the ascending aorta and sharpness of the angle formed by the CCA and the aorta contribute to this difficulty. Under such conditions, as a first step, a catheter and/or guidewire with a different angle or rigidity must be introduced. Even when the guidewire can be inserted into the CCA, however, its tortuosity may prohibit the introduction of the guiding catheter along the guidewire. In such cases, we manually compress the CCA to stabilize the wire in the artery and then insert the guiding catheter along the wire (Fig 1). When a coaxial catheter system is used, the inner catheter can be compressed for stabilization, and the guiding catheter can then be inserted along the inner catheter. This technique can be used in both conventional angiographic and neurointerventional procedures.

Carotid-compression technique I. A, After insertion of the guidewire, the CCA is manually compressed (arrow). B, The inner catheter (Glidecath, Terumo, Tokyo, Japan) is first inserted along the guidewire stabilized by manual compression of the CCA. The guiding catheter (Guider, Boston-Scientific, Natick, Mass) is then inserted along the inner catheter. Arrowheads indicate the tip of the guiding catheter.
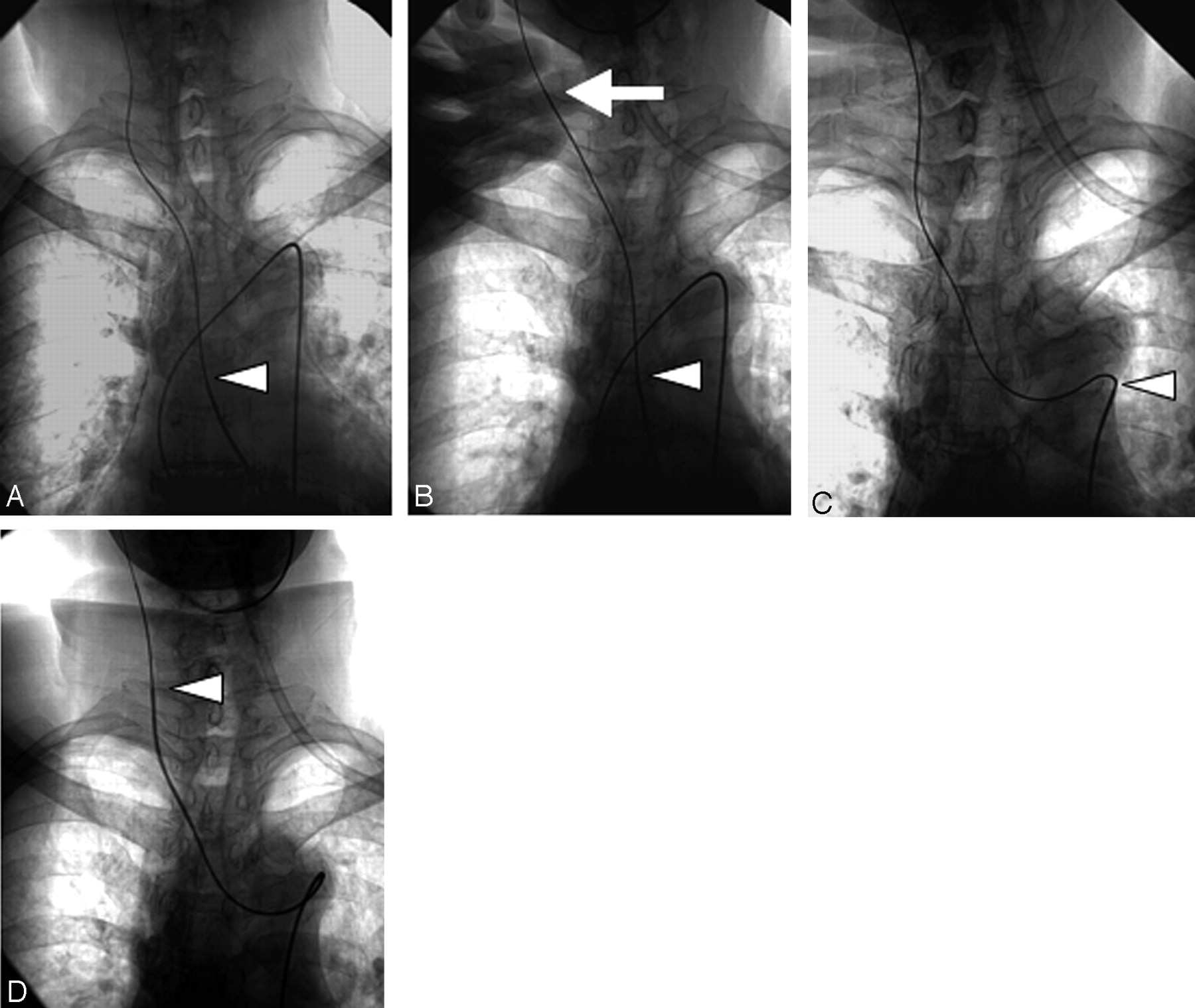
In cases where insertion of the guidewire is impossible, different approaches such as the transbrachial- and transcarotid artery approach can be taken. If the femoral approach is considered optimal, the “turn-over technique” can be used to insert the guidewire into the CCA.1,2 In patients undergoing neurointerventional procedures, the inserted guidewire must be straightened. Otherwise, the inserted guiding catheter moves into the left ventricle over the aortic valve. It is rarely possible to straighten the catheter by simply pulling on the tail of the guidewire, because this maneuver risks withdrawal of the inserted guidewire from the CCA. If the CCA is compressed manually, however, the stabilized guidewire can be straightened with the coaxial catheter by pulling on its tail regardless of the presence or absence of an inner catheter (Fig 2). The catheter can then be inserted into the CCA along the straightened wire and the manual compression is released. The wire and catheter are subsequently advanced as far as necessary in the internal or external carotid artery.

Carotid-compression technique II. A, The coaxial system (Shuttle, Cook/Glidecath, Terumo, Bloomington, Ind) is inserted into the ascending aorta, and the guidewire and inner catheter are then introduced into the target CCA or ICA by using the turn-over technique. B, The CCA is then compressed manually (arrow) to stabilize the guidewire and inner catheter. C, Withdrawal of the system toward the femoral artery results in its straightening. D, The guiding catheter is then advanced along the inner catheter. Arrowheads indicate the tip of the guiding catheter.
Results and Discussion
Between April 2003 and March 2005, 303 patients with cerebrovascular disease were referred to our institution for endovascular treatment. In 12 of them, regular catheterization was not possible and they (8 men and 4 women, ranging in age from 58 to 89 years; mean age, 74.6 years) underwent our carotid-compression technique. We successfully inserted the guiding catheter in 10 of these 12 patients. In one patient we could not insert the guiding catheter into the CCA because the guidewire slipped down despite sufficient compression of the vessel. In the other patient, the guiding catheter was inserted into the CCA, but it developed a kink because the angle between the origin of the CCA and the aorta was very acute. None of the 12 patients experienced clinical complications, and subsequent procedures were carried out uneventfully.
Our “carotid-compression technique” requires neither special catheters or guidewires nor the puncture of other vessels and is less risky than direct puncture of the carotid artery. Nevertheless, it is not risk-free, because excessive compression of the CCA may result in vessel injury. Therefore, other techniques (eg, distal guidewire insertion, compression of the wire inserted into the occipital artery, the coaxial technique using the microcatheter system, and use of a Simmons-type guide catheter) should be considered before attempting our technique. In addition, before undertaking our procedure, the degree of atherosclerosis in the target carotid artery should be assessed by preoperative MR/CT angiography or by angiography following the injection of contrast material into the origin of the CCA. Braided, nonkinking catheters may yield the best results. Hydrophilic-coated guidewires are sometimes unsuitable because they tend to slip during insertion of the guiding catheter. Our technique can also be used with the transbrachial artery approach.
In patients subjected to neurointerventional procedures, excessive manipulation of the target artery in the course of attempted catheter insertion can result in thromboembolic complications. Thromboemboli after coil embolization3,4 and conventional cerebral angiography have been reported.5,6 Our carotid-compression technique is a simple and relatively safe option in patients who require neurointerventional procedures but whose vascular anatomy is tortuous.
Acknowledgments
We thank Ms. U. Petralia for editing this manuscript.
- Received December 29, 2005.
- Accepted after revision April 3, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.