
Abstract
BACKGROUND AND PURPOSE: The purpose of this study is to estimate the change in partial pressure of oxygen (Pao2) during percutaneous vertebroplasty and also to examine the factors related to the change in Pao2.
MATERIALS AND METHODS: We retrospectively reviewed preprocedural and postprocedural Pao2 of 59 consecutive patients who underwent percutaneous vertebroplasty between November 2003 and April 2005 (11 men and 48 women; age range, 50–93; mean age, 75 years). Fifty-four patients were treated for osteoporosis-related fractures and 5 had malignant disease. Percutaneous vertebroplasty was performed in a conventional manner under local anesthetics and conscious sedation. Preprocedural and postprocedural blood drawing was performed 5 days to 30 minutes before percutaneous vertebroplasty and also at 30 minutes after the injection of bone cement. The difference between preprocedural and postprocedural data of Pao2 was correlated with patients’ age, number of treated vertebral bodies, presence of cement leakage, and presence of malignant neoplasm for each patient.
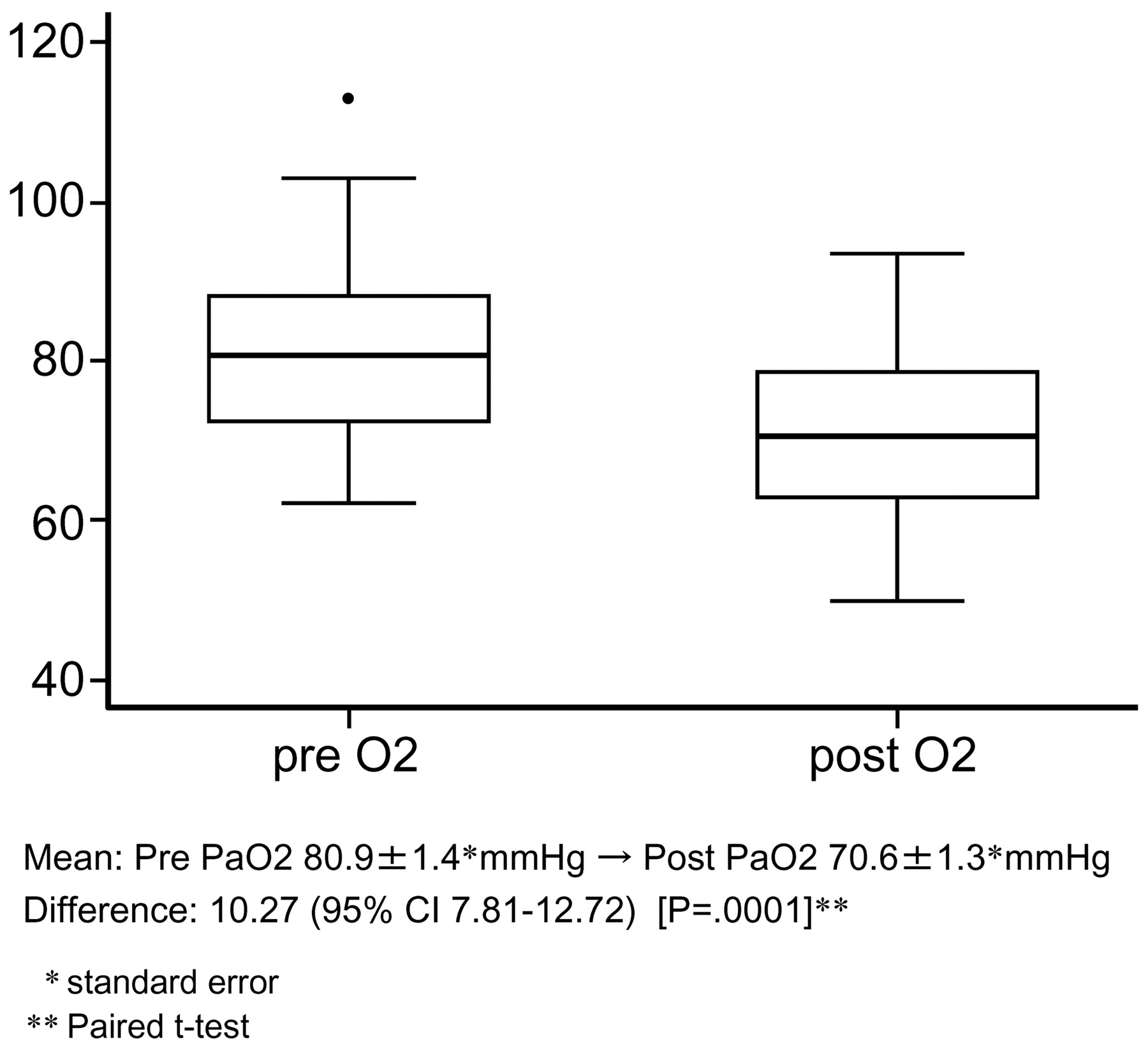
RESULTS: Mean pre-Pao2 and post-Pao2 were 80.9 ± 1.4 and 70.6 ± 1.3 mm Hg (mean ± SE) respectively (P = .0001). Using analysis of variance, there was a significant difference according to the number of vertebral bodies. There was a positive trend of decrease in Pao2 according to the number of vertebral bodies during percutaneous vertebroplasty. Using multiple linear regression and after adjusting by preprocedural Pao2 and other variables, the number of vertebral bodies was still highly significant.
CONCLUSION: Pao2 decreases during percutaneous vertebroplasty, and there is a correlation between the number of treated vertebral bodies and decrease in Pao2.
Cardiopulmonary disorder is one of the most serious complications during percutaneous vertebroplasty. Transient hypotension during percutaneous vertebroplasty has been reported.1 Kaufmann et al2 reported that oxygen saturation was significantly lower at 10 minutes after injection of polymethylmethacrylate (PMMA) than before injection, though the mean difference was negligible. The potential risk of cardiopulmonary changes during percutaneous vertebroplasty is of interest because percutaneous vertebroplasty is now widely implemented.
The purpose of this study was to estimate the change in partial pressure of oxygen (Pao2) during percutaneous vertebroplasty and also to examine the factors related to the change in Pao2.
Materials and Methods
All procedures were performed according to institutional review board-approved guidelines. We extracted the relevant data from the medical records of 59 consecutive patients (11 men and 48 women) who underwent percutaneous vertebroplasty between November 2003 and April 2005. Patients’ age range was 50–93 with mean age 75 years. The number of vertebral bodies treated was similar in terms of categories (1, n = 17; 2, n = 19; ≥3, n = 23). The level of vertebral bodies was from T6 to L5. Fifty-four patients had compression fractures as a result of osteoporosis, and 5 patients had malignant neoplasm. Cement leakage was evaluated on a postprocedural multidetector CT and classified into cement leakage into adjacent disk and outside disk. Cement leakage into adjacent disk and outside disk was found in 33 of 59 and 16 of 59, respectively.
Percutaneous vertebroplasty procedure was performed in a conventional manner using a biplane angiography unit under local anesthesia and conscious sedation. The patient was placed in a prone position on an angiography table with sterile conditions. After a small skin incision was made, a disposable 11- or 13-gauge bone biopsy needle (Cook, Bloomington, Ind) was positioned with its tip near the center of the pedicle. Anteroposterior and lateral fluoroscopy was used to advance the needle through the pedicle into the vertebral body. PMMA was prepared by combining sterile barium and cranioplastic cement (Codman Cranioplastic; Johnson & Johnson Medical, Berkshire, United Kingdom). Injection of PMMA was performed either manually or with an injection device.
Pao2 was measured by a conventional blood gas analyzer (ABL700; Radiometer Medical, Copenhagen, Denmark). Arterial blood drawing was taken from the radial or femoral artery with the patient in a supine position. We measured preprocedural Pao2 5 days to 30 minutes before percutaneous vertebroplasty and postprocedural Pao2 30 minutes after percutaneous vertebroplasty.
For statistical analysis, paired t test was used to examine the difference between preprocedural and postprocedural Pao2. Analysis of variance followed by t test was used to examine the difference in Pao2 according to the number of treated vertebral bodies. Nonparametric trend test was used to estimate the trend of difference in Pao2 depending on the number of treated vertebral bodies. Multiple linear regression technique was used to examine the correlation between the difference in Pao2 and the following factors: patients’ age, sex, number of treated vertebral bodies, presence of cement leakage, and presence of malignant diseases (adjusted by preprocedural Pao2).
Results
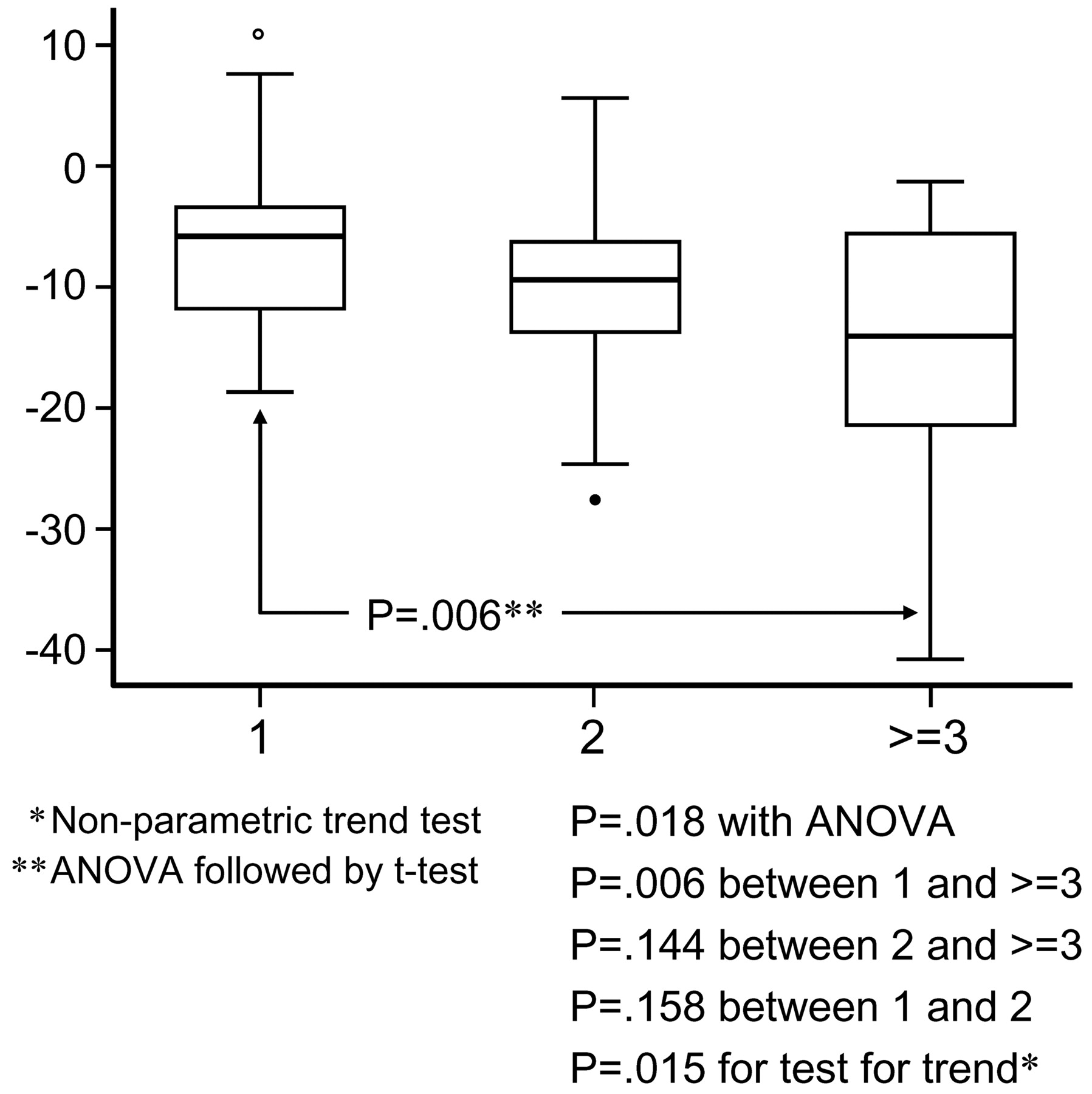
Mean (± SE) preprocedural and postprocedural Pao2 values were 80.9 ± 1.4 and 70.6 ± 1.3 mm Hg, respectively. The difference between mean preprocedural and postprocedural Pao2 was 10.3 mm Hg and was highly significant at P < .0001 levels (Fig 1). Difference in Pao2 between preprocedure and postprocedure, depending on the number of treated vertebral bodies, is shown in Fig 2. Using analysis of variance, there was a significant difference according to the number of vertebral bodies. We found significant difference between the patients who had 1 and ≥3 vertebral bodies during percutaneous vertebroplasty (P = .006), though there was no significance between 1 and 2 (P = .158), or 2 and ≥3 (P = .144). Using a test for trend, there was a positive trend of decrease in Pao2 according to the number of vertebral bodies during percutaneous vertebroplasty (P = .015). We confirmed our finding of bivariate analysis by using multivariate technique (Table 1). We used multiple linear regression, and after adjusting by preprocedural Pao2 and other variables, the number of vertebral bodies was still highly significant (P = .011) for the decrease in Pao2. This was confirmed with a high level of confidence using the multiple regression model with independent variables: preprocedural Pao2 and number of vertebral bodies (R2 value 0.336 versus 0.296, P = .005) (Table 2).

The difference between preprocedural and postprocedural Pao2.

Difference in Pao2 before and after the procedure depending on the number of treated vertebral bodies.
Results of multiple regression: model 1
Results of multiple regression: model 2
Discussion
Percutaneous vertebroplasty was first described in France in 1987.3 The potential risk of cardiopulmonary changes during percutaneous vertebroplasty is of interest because percutaneous vertebroplasty is now widely used for the standard treatment of osteoporotic fractures and metastatic tumors of the vertebral bodies. We found a decrease in Pao2 after percutaneous vertebroplasty, but the cause of the decrease remains unclear.
According to the US Food and Drug Administration (FDA) Center for Devices and Radiologic Health, through the on-line data base (http://www.fda.gov/cdrh/maude.html) for adverse event reporting, 19 complications associated with percutaneous vertebroplasty were reported, including 7 deaths and 4 cardiovascular events. Of the 7 patients who died, 4 underwent percutaneous vertebroplasty with lateral approach and 3 with transpedicular approach.4 Two had undergone multilevel vertebroplasty (8 in one case and 10 in the other) and experienced cardiovascular collapse, and 1 had a presumed anaphylactic reaction to bone cement, resulting in cardiac and/or respiratory arrest and death. In addition, of 4 patients who survived, 2 experienced diminished blood pressure and 2 had cardiac arrest. Pulmonary collapse during percutaneous vertebroplasty, including pulmonary embolism and acute respiratory distress syndrome, is a major concern, and symptomatic or asymptomatic pulmonary emboli associated with percutaneous vertebroplasty were reported.5-10 Although the overall number of such cases is small, the cardiopulmonary complications can be fatal.
There have been a few reports describing oxygen desaturation during conscious sedation.11-13 Sedative drugs are known to decrease respiratory function, and there is a report that myocardial ischemia occurred with the use of sedative drugs.14 In most cases of percutaneous vertebroplasty, sedative drugs are prescribed preoperatively and can affect oxygenation during percutaneous vertebroplasty. Furthermore, functional residual capacity may decrease during percutaneous vertebroplasty as a result of thoracic compression attributable to the prone position, which may be an important factor of deoxygenation. Patients who received supplemental oxygen during procedure were not included in this study. However, the use of supplemental oxygen during the procedure might avoid decrease in Pao2.
Another cause of postprocedural decrease in Pao2 may be pulmonary embolism. The source of emboli could be fragments of fatty bone marrow, which are created by increased intramedullary pressure during injection of PMMA or may be particles of PMMA themselves.5-7
Several reasons why the number of treated vertebral bodies affects postprocedural decrease in Pao2 can be speculated upon. The reasons include increase in duration of percutaneous vertebroplasty procedure in prone position, increase in unpolymerized liquid monomer, cement volume, and possibly fragments of bone marrow. The consecutive augmentation of multilevel vertebral bodies with PMMA may induce a cumulative pulmonary embolism that deteriorates baseline Pao2. Increase in number of needles, causing breath-holding due to procedural pain, could be another contributing factor. Another reason that multilevel vertebroplasty may correlate with decrease in Pao2 is that perhaps more sedation was used. However, the pathophysiology for the Pao2 decrease seems to be multifactorial.
The limitations of this study may be lack of sequential evaluation of Pao2 after percutaneous vertebroplasty. Continuous intra-arterial blood gas monitoring during percutaneous vertebroplasty would be ideal. Although pulse oximetry is convenient to assess the oxygenation, blood gas analysis is more sensitive to oxygenation compared with pulse oximetry.
Our methodology has no power to suggest that PMMA injection has any effect on Pao2 beyond the effects of prone positioning and moderate sedation, which plausibly may contribute to decreased Pao2. Moreover, no data were collected to show that the decrease in Pao2 was sustained more than 30 minutes beyond the procedure.
Conclusion
Pao2 decreases during percutaneous vertebroplasty, and there is a correlation between the number of treated vertebral bodies and a decrease in Pao2. However, the pathophysiology of the decrease in Pao2 is not clear and may be related to sedation, the patients’ prone position, and/or pulmonary embolism. Physicians should be aware of the potential for a drop in Pao2 with percutaneous vertebroplasty.
Footnotes
Paper previously presented at: Annual Meeting of the American Society of Neuroradiology; May 21–27, 2005; Toronto, Ontario, Canada.
References
- Received February 18, 2006.
- Accepted after revision May 23, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.