
Abstract
SUMMARY: We report 3 patients with previously undiagnosed spinal dural arteriovenous fistulas (SDAVFs), who developed acute paraparesis following lumbar epidural steroid injection. MR imaging demonstrated spinal cord T2 hyperintensity, edema and/or enhancement of the conus, and intradural enlarged vascular flow voids. Spinal angiography confirmed SDAVFs arising from pedicles remote from the sites of the epidural steroid injection. Fistulas were eliminated with either endovascular or combination endovascular and open surgical approaches, with subsequent partial resolution of paraparesis.
Of 26 patients with spinal dural arteriovenous fistulas (SDAVFs) evaluated at our institution during the last decade, 3 developed new or worsening paraparesis soon after injection of epidural corticosteroids to treat back pain and/or lower extremity sensory symptoms. None of these 3 patients had received the diagnosis of SDAVF before epidural steroid injection, though in retrospect, the patients had findings suggestive of SDAVF on MR imaging performed before epidural injection.
Case Reports
Case 1
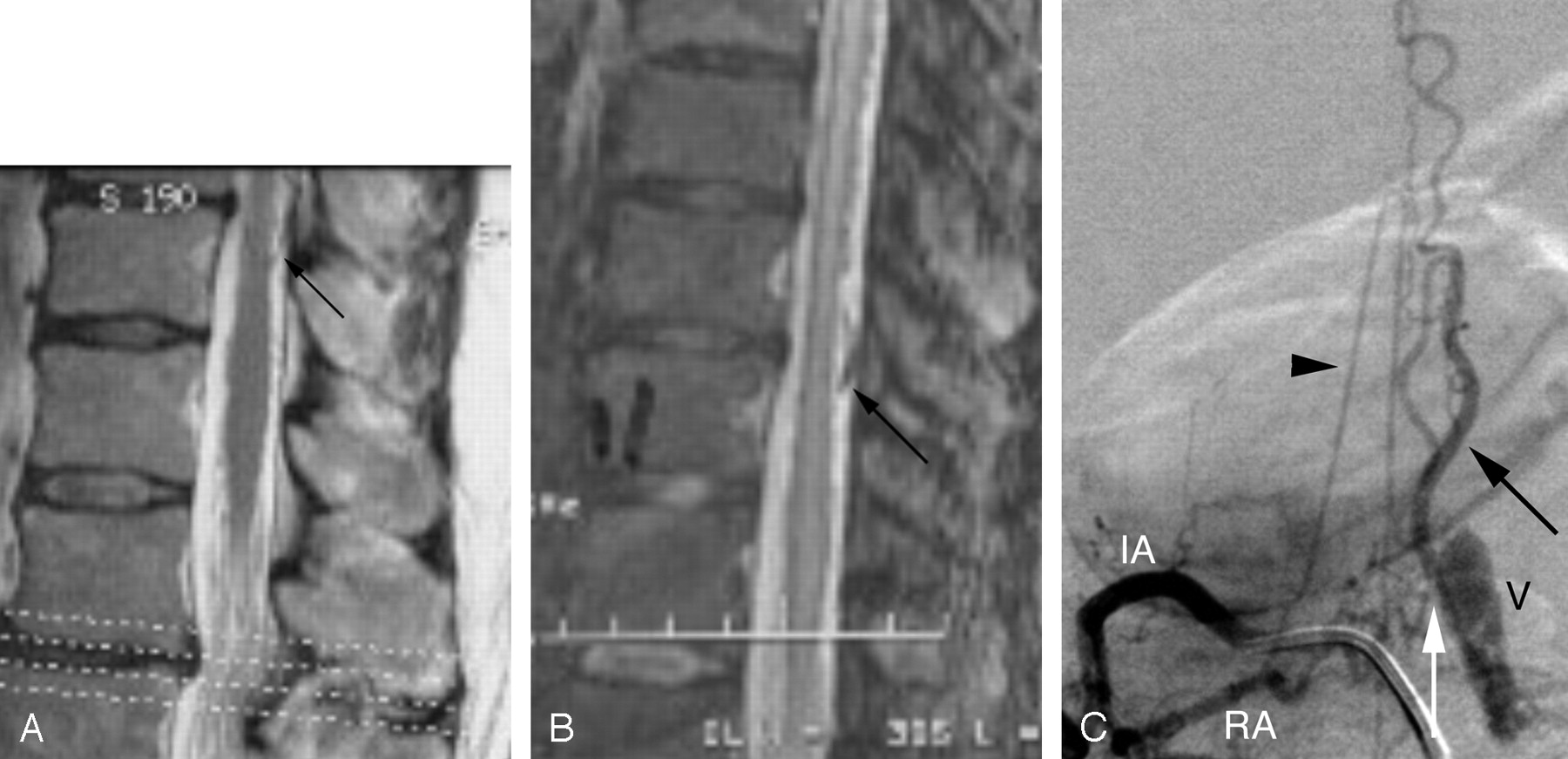
A 56-year-old male high school football coach presented with 6 months of bilateral lower extremity numbness. He was diagnosed with diskogenic spinal stenosis at L1–2 on the basis of a lumbar spine MR imaging (Fig 1A), for which he received an epidural corticosteroid injection (14 mL of a mixture of 12 mL ropivacaine 0.2% and 2 mL of methylprednisolone 80 mg/mL) at L2–3. Seven hours following this procedure, the patient developed acute paraparesis, which progressed during the next 3 days. The patient also developed urinary retention. Thoracolumbar spine MR imaging was performed (Fig 1B), and the patient was transferred to our hospital.

A, Sagittal T2-weighted lumbar MR image demonstrates subtly enlarged flow voids dorsal (arrow) and ventral to the conus, in addition to mild spinal canal stenosis due to a dorsal disk protrusion at L1–2. Signal intensity in the conus itself is normal.
B, Sagittal T2-weighted thoracolumbar MR image demonstrates extensive T2 hyperintensity in the central spinal cord from T4 to the conus, with associated peripheral cord T2 hypointensity. Multiple enlarged flow voids are evident dorsal and lateral to the thoracic and lumbar spinal cord. The same enlarged vein posterior to T10–11 in A is indicated by an arrow but has markedly increased in caliber. Neither epidural hematoma, intrathecal hemorrhage, nor hematomyelia is present on this or other images (not shown) from this study.
C, Anteroposterior view from the arterial phase of an angiogram of the right T11 intercostal artery (IA) demonstrates a SDAVF (fistula site marked with white arrow) originating from the right T11 radicular artery (RA). The artery of Adamkiewicz (black arrowhead) also arises from the right T11 intercostal artery radicular branch. The black arrow indicates the dorsal intradural draining vein of the SDAVF, the same structure seen by MR imaging in A and B. A prominent venous varix (V) of the proximal portion of the draining intradural vein is present just beyond the fistula site.
At our institution, the patient was unable to stand without assistance. Light touch sensation was decreased in the lateral thighs and calves. The patient had a urinary catheter in place and complained of bowel retention. A spinal angiogram demonstrated a SDAVF originating from the right T11 radicular artery (Fig 1C). The intrathecal vein draining this SDAVF coursed both inferiorly toward the conus and superiorly, eventually exiting the thecal sac at C4–5. Because the artery of Adamkiewicz also arose from the right T11 intercostal artery radicular branch, it was decided that liquid adhesive embolization would incur significant risk to the spinal cord blood supply. Thus, the vein draining the SDAVF was surgically clipped. A repeat spinal angiogram performed 2 days after surgery demonstrated minimal residual filling of the dilated perimedullary vein at T11, but no residual arteriovenous shunt surgery. A single electrolytically detachable coil was placed beyond the origin of the artery of Adamkiewicz in the feeding artery to the residual SDAVF, with elimination of arterial flow to the fistula site.
The patient improved, eventually being able to walk with a cane, urinate normally, and have bowel movements by using laxatives and suppositories. Bilateral lateral calf and thigh numbness persisted. A follow-up angiogram was obtained 5 months after the initial treatment because of the persistence of symptoms and a concern for recurrent arteriovenous shunt surgery, given that coil embolization is associated with a significantly higher rate of recurrence than liquid adhesive embolization. This angiogram demonstrated no residual SDAVF and no other sites of shunt surgery.
Case 2
A 71-year-old male retired school teacher presented with 18 months of progressive bilateral lower extremity pain and weakness, eventually requiring a walker. Lumbar spine MR imaging was interpreted as spinal stenosis. The day following a lumbar epidural corticosteroid injection, the patient awoke with complete paralysis from the waist down, was taken to a local hospital, and spent 2 weeks in the intensive care unit receiving intravenous corticosteroids.
On transfer to our institution, the patient had an incomplete T11 sensory level, completely involving the trunk but with preservation of light touch in the lower extremities. Plantar reflexes were mute and deep tendon reflexes were hyperactive. Leg strength was 2/5. A Foley catheter was in place. Review of the patient's initial outside MR imaging demonstrated cord enlargement and T2 hyperintensity from T10 to the conus, with small intrathecal vascular flow voids at the T10–11 level. Minimal diffuse enhancement of the conus was also noted. Spinal angiography demonstrated a single direct SDAVF within the left T10–11 neural foramen, arising from the left T10 radicular artery, with an enlarged draining vein coursing inferiorly around the conus. Endovascular therapy was attempted with a microcatheter injection of N-butyl cyanoacrylate (n-BCA) liquid adhesive, but the glue polymerized proximal to the fistula site. The fistula was exposed surgically, clipped, transected, and excised.
The patient's leg weakness improved for 1 month but then began to worsen, prompting repeat spinal angiography, which demonstrated a persistent fistula on the left at T10, which was not amenable to endovascular therapy. The fistula was surgically coagulated. Postoperative spinal angiography showed no residual SDAVF. Two years later the patient's neurologic status was only mildly improved. The patient could ambulate with a walker and required urinary self-catheterization.
Case 3
A 60-year-old female administrative assistant presented with 14 months of bilateral thigh burning sensation, for which she received a lumbar epidural corticosteroid injection. The next day, she developed acute paraparesis and collapsed to the floor. She had bilateral lower extremity numbness and hyperreflexia and bilateral quadriceps weakness. An MR imaging of the lumbar spine showed multiple lumbar disk protrusions and enlargement of the conus. Intravenous corticosteroids were administered. The patient's leg strength improved initially but worsened within a month, prompting the initiation of intravenous immunoglobulin for a clinical diagnosis of Guillain-Barré syndrome. The patient then developed urinary retention, bilateral lower extremity areflexia, and reduced bilateral leg strength. A second MR imaging of the lumbar spine demonstrated progressive enlargement and postgadolinium enhancement of the lower thoracic spinal cord to the conus, prompting an interpretation of spinal cord tumor. Conus biopsy yielded a pathologic diagnosis of arteriovenous malformation, and the patient was transferred to our institution.
At our hospital, the patient initially was paraplegic, with bilateral lower extremity numbness and urinary and bowel retention. Angiography demonstrated an SDAVF in the right L5-S1 neural foramen, with a draining vein coursing superiorly toward the conus. Endovascular occlusion of the fistula was successful by using n-BCA delivered to the medial sacral branch of the right internal iliac artery. The day following embolization, the patient had improved bilateral lower extremity strength. One month later, the patient had 3/5 strength in the legs, but no improvement in leg numbness or in bowel and bladder retention.
Discussion
SDAVFs are thought to cause myelopathy due to venous hypertension, venous engorgement, and eventually ischemia of the spinal cord.1-7 The ability to drain arterialized venous blood from the spinal cord pial venous plexus to extradural veins depends on patent intradural-to-extradural venous connections and the pressure in the epidural space. Various mechanisms are proposed to prevent transmission of increased extradural pressures (such as during the Valsalva maneuver) to the intradural veins, including narrowing of the radiculospinal veins as they pierce the dura and the presence of the glomeruli of Manelfe between the layers of the thoracic and lumbar dura mater.
The ambient pressure in the epidural space is zero or negative.8 The instillation of material into the lumbar epidural space normally has little effect on the pressure of intradural veins because of the antibackflow mechanisms and the large epidural potential space. However, in patients who have a pre-existing (though in the current cases undiagnosed) SDAVF causing early symptoms, the addition of material to the epidural space may be enough to exacerbate venous hypertension in the spinal cord, thus leading to acute worsening of symptoms. If patients with undiagnosed SDAVFs also have epidural adhesions or spinal stenosis, the local pressure near the epidural steroid injection site could be further raised.
The patients in this series demonstrated SDAVFs in which both the arteriovenous fistula site and the principal intradural-to-extradural venous drainage sites were not at the exact site of epidural steroid injection. This argues against the trauma of the injection directly causing a fistula. Instead, it seems more likely that the instillation of materials into the epidural space can raise the epidural pressure enough to impair or redirect venous drainage, causing symptomatic decompensation in patients who are, by virtue of having untreated SDAVFs, already experiencing the early manifestations of venous congestive myelopathy. Alternatively, placement of a needle or materials in the lumbar epidural space might directly thrombose a radiculospinal vein that previously drained the SDAVF; redirection of venous flow to more remote sites of intradural-to-extradural drainage (such as in patient 1, who had drainage in the cervical spine) could also increase the intramedullary pressure, resulting in congestive myelopathy. However, many SDAVFs in patients who have not received epidural injections or other spinal instrumentation present with intradural-to-extradural venous drainage remote from the fistula site.
Although hemorrhagic complications of epidural injections have been reported to cause acute myelopathy,9 the imaging studies of the patients in this case series do not provide evidence for such an explanation in these specific cases. Injection into the spinal cord itself, development of a compressive epidural hematoma, or induction of extensive intrathecal hemorrhage would provide logical alternative explanations for the rapidly declining clinical course of these patients. MR imaging performed at outside institutions shortly after the epidural injections and, when applicable, MR imaging performed at our institution in a more-delayed manner, did not demonstrate epidural hematomas, intrathecal hemorrhage, or hematomyelia. For example, it can be posited that the T2 prolongation in the conus and lower thoracic spinal cord in patient 1 (Fig 1B) could have been due to direct injection of the spinal cord. However, both the documentation of needle placement at L2–3 and the craniocaudal extent of the T2 abnormality over several vertebral segments argue against direct cord puncture.
Injection of medications into the lumbar epidural space is associated with development of acute paraparesis in patients with previously undiagnosed SDAVFs. Careful scrutiny of spine MR images for signs of SDAVF is warranted before injection of materials into the epidural space. If MR imaging findings suggestive of SDAVF are present either before or after epidural injection, spinal angiography is recommended to facilitate early endovascular or surgical intervention to minimize the duration of spinal cord venous hypertension and reduce the likelihood of permanent paraparesis.
- Received March 21, 2006.
- Accepted after revision June 5, 2006.
- Copyright © American Society of Neuroradiology





{kind=link}