
Abstract
SUMMARY: Atypical teratoid/rhabdoid tumor (AT/RT) is a highly malignant central nervous system neoplasm usually seen in young children and infants. Prognosis for AT/RT is poor, with most patients dying within 1 year of presentation. AT/RT most commonly occurs intracranially. Location in the spine, though previously reported, is rare, and imaging findings have not been emphasized in the past. We present a case of AT/RT occurring in the thoracolumbar spine of a child and review available clinical and imaging findings in previously reported cases of spinal AT/RT.
A 9-year-old boy presented with right-legged numbness. The weakness progressed to lower extremity paralysis and urinary incontinence over a 3-month period. Lumbar spine MR imaging obtained at an outside hospital demonstrated a spinal canal mass. The patient was transferred to our facility for further evaluation, and MR imaging of the entire spine and brain was performed.
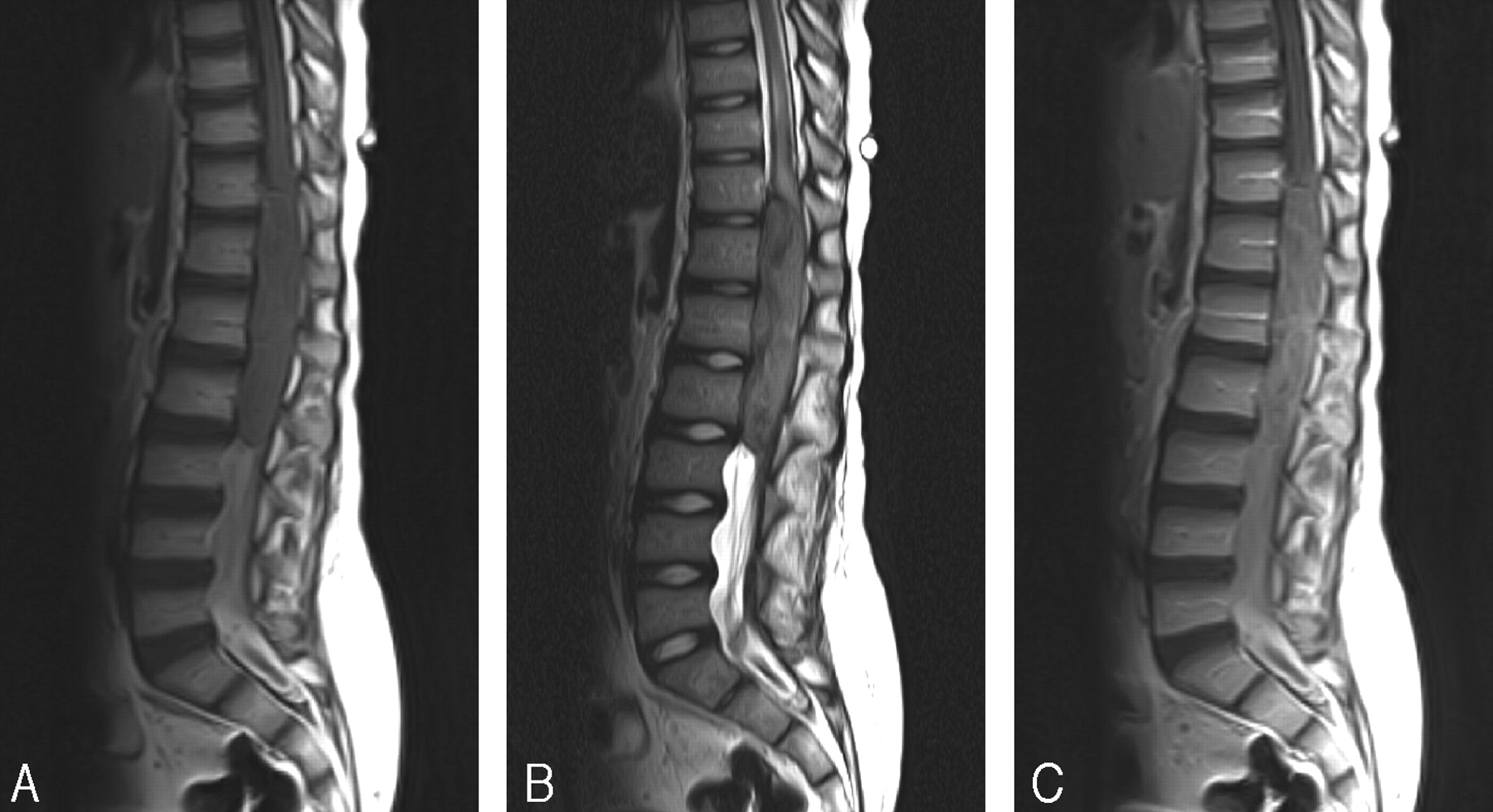
MR imaging showed a large heterogeneous mass that filled the spinal canal from T11 to L2. The lesion was hypointense to cord on T1-weighted images (Fig 1A) and predominantly isointense on T2-weighted images (Fig 1B). Regions of T2 hypointensity within the tumor demonstrated increased susceptibility on the gradient images, consistent with hemorrhage. Abnormal T1 shortening was visualized filling the distal thecal sac, suggestive of hemorrhage, tumor seeding, or proteinaceous debris. On the postcontrast images, there was diffuse enhancement of the tumor, with no further enhancement in the distal thecal sac (Fig 1C). A hypointense cap along the superior margin of the tumor on the T2-weighted images suggested an extramedullary location. Findings of MR imaging of the brain, performed at the same time, were normal. Differential diagnosis based on imaging was myxopapillary ependymoma and atypical nerve sheath tumor. The patient was taken to surgery, which confirmed a hemorrhagic intradural extramedullary mass. The lesion was fully resected.

A, Sagittal T1-weighted image demonstrates a mass filling the spinal canal from T11 through L2. The lesion is hypointense to cord. Hyperintense signal intensity filling the distal thecal sac demonstrated no enhancement on postcontrast images, consistent with hemorrhage or proteinaceous debris.
B, On the sagittal T2-weighted image, the mass is isointense to cord with focal areas that are hypointense. The nerve roots are clumped distally, and there is edema in the cord rostrally.
C, Sagittal postcontrast T1-weighted image shows diffuse enhancement of the mass. There is no additional enhancement in the distal thecal sac.
Pathologic examination showed sheets of monomorphous round-to-polygonal cells, with a brisk mitotic rate and necrosis. The cells had moderate amounts of variably clear-to-amphophilic cytoplasm. Nuclei had coarse chromatin, with occasional prominent nucleoli. Rare cells demonstrated rhabdoid features (Fig 2). The tumor was positive for neuron-specific enolase and epithelial membrane antigen (EMA) by immunohistochemistry. The cells revealed loss of nuclear staining for integrase integrator 1(INI1). Cytogenetic testing demonstrated an INI1 gene mutation.

Rare cells with rhabdoid features (arrow), eccentric nuclei, and eosinophilic cytoplasmic hyaline inclusions (hematoxylin-eosin, ×600).
On the basis of the pathologic findings, further imaging was undertaken to exclude a renal mass. Findings of sonography and abdominal CT were normal.
The patient was treated with radiation therapy. Chemotherapy was also offered, but the family declined. MR imaging of the brain and spine at 3 months after surgery demonstrated no evidence of residual tumor, recurrence, or metastatic disease.
Discussion
AT/RT is a highly malignant central nervous system (CNS) neoplasm that most often occurs in children younger than 2 years of age.1, 2 The tumor is markedly aggressive, with a median survival time of less than 1 year.1–3 Formerly called malignant rhabdoid tumor, it was first described in 1978 as an aggressive variant of Wilms’ tumor arising from the kidney.4 Primary intracranial disease was initially reported by Lefkowitz et al in 1987.5 In a large landmark series in 1996, Rorke et al1 defined it further as a distinct CNS neoplasm, and it was given the descriptive diagnostic name “atypical teratoid/rhabdoid tumor” (AT/RT). The term “rhabdoid” was adopted because of the similarity of the lesion to rhabdomyosarcoma under light microscopy.6 The multiplicity of cell types linked it to a form of teratoma, though it was histologically distinct and lacked germ cell markers.1, 7
Historically, the incidence of AT/RT was likely underestimated because of its similarity to primitive neuroectodermal tumor (PNET), both histologically and by imaging.1, 2 Because its response to treatment is unequivocally poor compared with PNET, differentiating AT/RT from other tumors is important for treatment planning. Hilden et al8 documented improved survival time when patients with AT/RT tumor were given more intensive therapy.
Although imaging may suggest AT/RT, diagnosis is based on immunochemistry findings and light microscopy and can be further supported by genetic analysis. Histologically, AT/RT is characterized by the presence of large rhabdoid cells, areas of tumor that resemble PNET, and malignant epithelial and mesenchymal components that lack divergent tissue-differentiation characteristics of malignant teratomas. Immunohistochemically important markers are EMA, vimentin, and smooth-muscle antigen.1, 2 Loss of nuclear staining for INI1 is also characteristic. Associated molecular genetic abnormalities, seen in up to 50% of cases,6 include inactivating mutations of the INI1 gene, which maps to chromosomal region 22q11.29; monosomy 22; or novel complex rearrangements involving chromosome 6 and 11.1
AT/RT most commonly occurs in the posterior fossa but can also occur supratentorially. Location in the spine is rare, and only 7 cases of primary CNS AT/RT arising from the spine were discovered in the literature.1, 3,9–12 Large series of CNS AT/RT emphasize the rarity of spine AT/RT. Series from Rorke et al1 and Cheng et al3 each reported 1 case of spine AT/RT out of 52 and 20 patients, respectively. In the largest series from Burger et al, 2 which included 55 patients, all of the lesions occurred intracranially.
Review of the 7 documented cases of spine AT/RT revealed an age range of 7 months to 17 years with 6 of the 7 cases occurring in children younger than 3 years.1, 3, 8–12 The oldest patient, aged 17, presented with a diffuse spinal cord tumor.10 Of the 6 focal lesions, 2 occurred in the cervical spine, both of which were intradural extramedullary1, 11; 2 were found in the thoracic spine, presenting as intramedullary masses9, 12; and 1 occurred in the thoracolumbar region and was intramedullary as well.10 One reported lumbar case was described as having an intradural location.3 In our patient, the lesion occurred in the thoracolumbar spine and was intradural extramedullary. There was no sex predilection, with 3 lesions occurring in girls, 3 in boys, and sex not specified in 1 case.1 Association with genetic abnormalities was not found9 or tested in other cases, whereas genetic analysis in our patient revealed a mutation in the INI1 gene. Outcome was dismal, with 6 of the 7 patients dying within 10 months of diagnosis and time of death not specified in 1 patient.1
Imaging findings in intracranial AT/RT have been previously well documented. The tumors are heterogeneous with solid portions that are isointense/hypointense on T2-weighted images. Hemorrhage and calcifications may be seen, and early CSF dissemination is common.2, 3, 7–10, 13 Imaging findings visualized thus far in spine AT/RT are nonspecific but are in keeping with findings described in the brain. The lesions are heterogeneous, reflecting their histopathologic complexity. Other imaging features include isointensity/hypointensity to cord on T2-weighted sequences and contrast enhancement.3, 9 Hemorrhage is not uncommon and was found at surgery in 1 other patient10 and was seen at imaging and at surgery in our patient. CSF dissemination was identified at presentation in 3 of the 6 previously reported cases3, 10, 11 and was not present in our patient. There was a syrinx or edema rostral to the tumor in 3 other cases,9–11 similar to what was visualized in our patient.
The differential diagnosis is dependent on site and origin of the lesion. For extramedullary lesions in the lumbar canal, the differential includes myxopapillary ependymoma and malignant nerve sheath tumor. PNET, ependymoma, astrocytoma, and ganglioglioma are in the differential diagnosis for intramedullary tumors in children, though the latter 2 are less likely to be hemorrhagic. Metastases should also be considered, and imaging of the entire CNS is recommended. If AT/RT is discovered at pathology, abdominal imaging should be obtained to exclude a primary renal tumor. On the basis of CNS cancer protocols, surveillance imaging is recommended every 3 months for 1 year following tumor resection.
AT/RT in the spine is rare but can be considered in the differential diagnosis of spinal canal tumors in children. The tumor can occur anywhere along the spinal axis and may be intramedullary or intradural extramedullary in origin. Imaging findings consistent with the diagnosis include heterogeneity, isointensity/hypointensity to cord on T2-weighted images, and hemorrhage. These findings, however, are nonspecific, and histology supported by immunochemistry and genetic analysis are essential in making the final diagnosis.
Acknowledgments
The authors thank Peter Burger, Alexander Judkins, and Bryan Wolf for their expertise in making the pathologic diagnosis.
References
- Received March 3, 2006.
- Accepted after revision April 3, 2006.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}