
Abstract
SUMMARY: We describe a middle-aged woman who inserted a sewing needle into her spinal cord in an attempt at performing her own acupuncture. Reports of neurologic injury are rare in the literature, despite the widespread use of acupuncture. This is the first case we have identified involving spinal cord injury from self-performed acupuncture.
A middle-aged woman presented to our emergency department stating that she had been performing her own acupuncture at home and had lost 1 of the needles. She stated that the treatment was for chronic neck pain. On further questioning, we learned that she had been unable to retrieve a needle placed in the midline of the upper cervical region posteriorly, with the end of the needle no longer palpable.
The patient confessed to having no formal training in acupuncture but had heard of its benefits through her friends. Home hand-sewing needles had been used in her attempt at self-therapy.
On examination, the puncture site showed a clean entry point at the midline upper neck. The neurologic examination showed a slight decrease in left-arm power (4/5) and altered sensation over the left C5–C8 dermatomes. Examination of the right lower limb and bilateral lower limbs revealed no abnormality.
Initial investigation was performed with conventional radiographs. These showed a large sewing needle in the posterior spinal soft tissues with the tip within the spinal canal (Fig 1). A combination of frontal and lateral projections indicated an intradural needle tip with probable cord involvement.

Conventional film showing the position of the sewing needle. Frontal view confirms that the needle is midline.
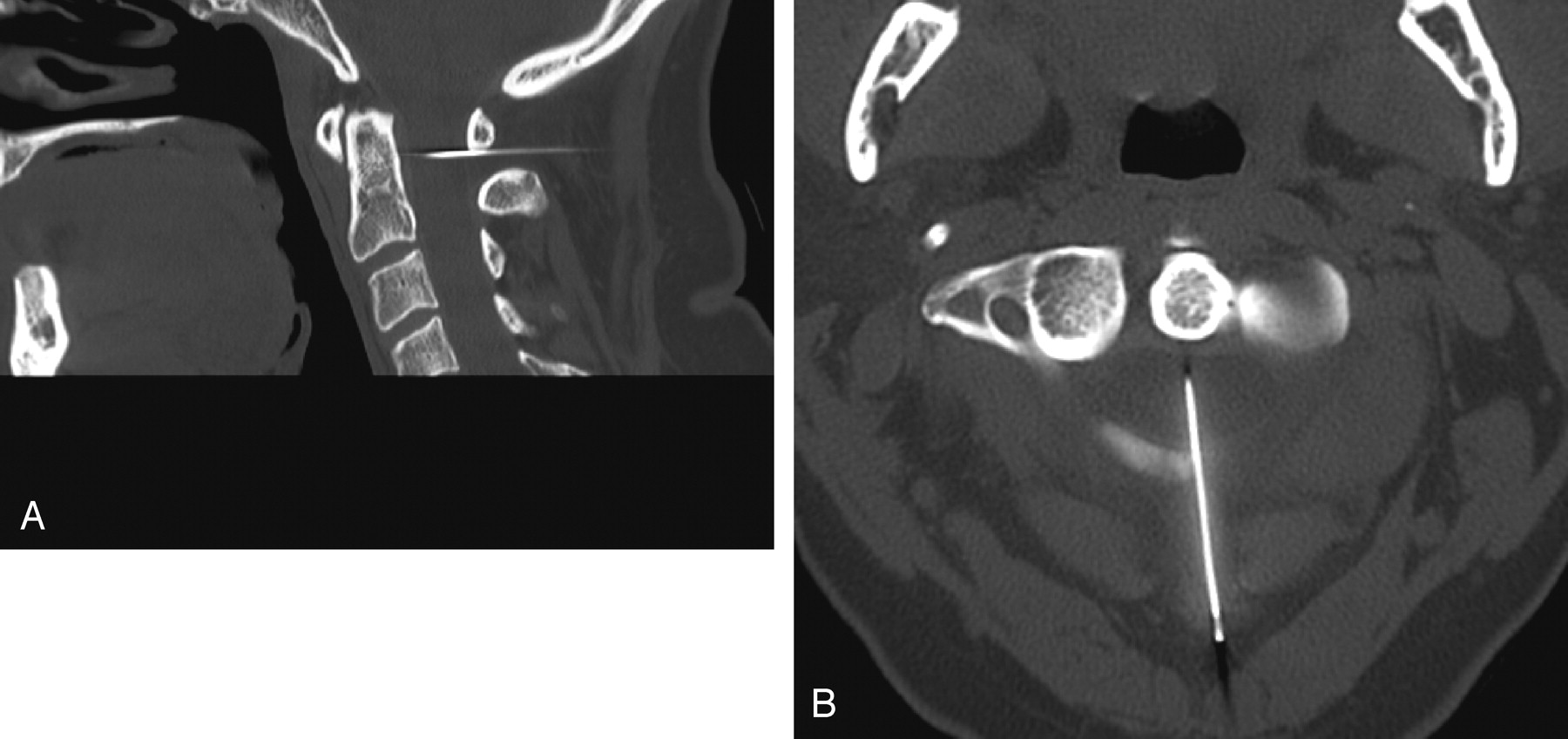
At this stage, further investigation was thought necessary before surgical intervention for needle removal. Because the clinical suspicion of significant cord injury was low and MR imaging was contraindicated given the nature of the needle and its position, we performed CT. This study confirmed the conventional film findings of needle-tip location within the spinal canal, with the spinal cord pierced in the midline posteriorly (Fig 2).

A and B, CT images confirming needle location with the tip appearing to pierce and traverse the cord in the midline posteriorly.
The patient was subsequently taken to the operating room, where the needle was uneventfully removed with the patient under general anesthesia. Postoperative neurologic examination showed improvement in the patient's status, with little in the way of residual neurologic deficit. Prophylactic antibiotics were administered because of the potential contaminated puncture. No further intervention was required by the clinical team. Because of the unusual circumstances, involvement of the social work team was initiated.
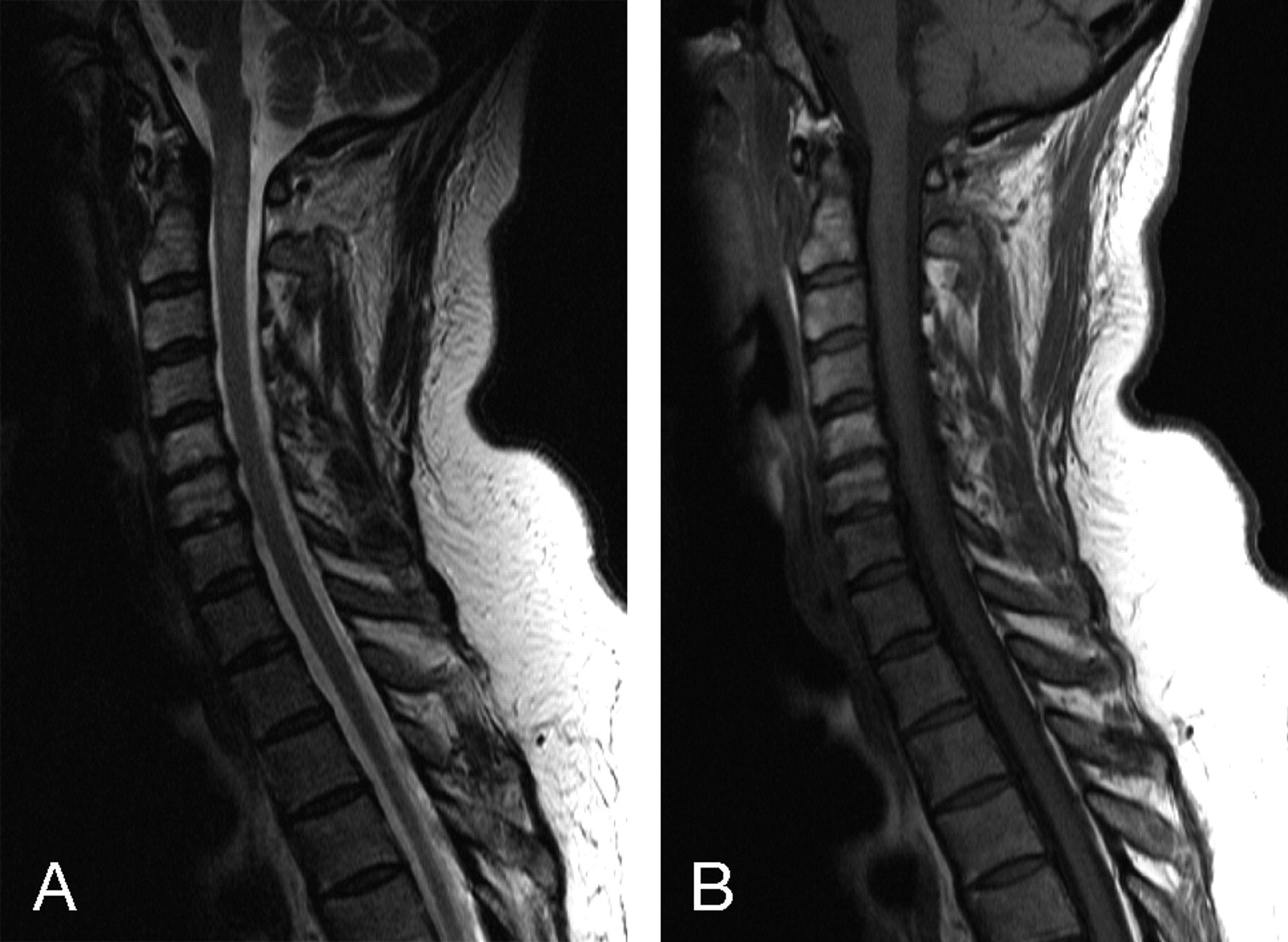
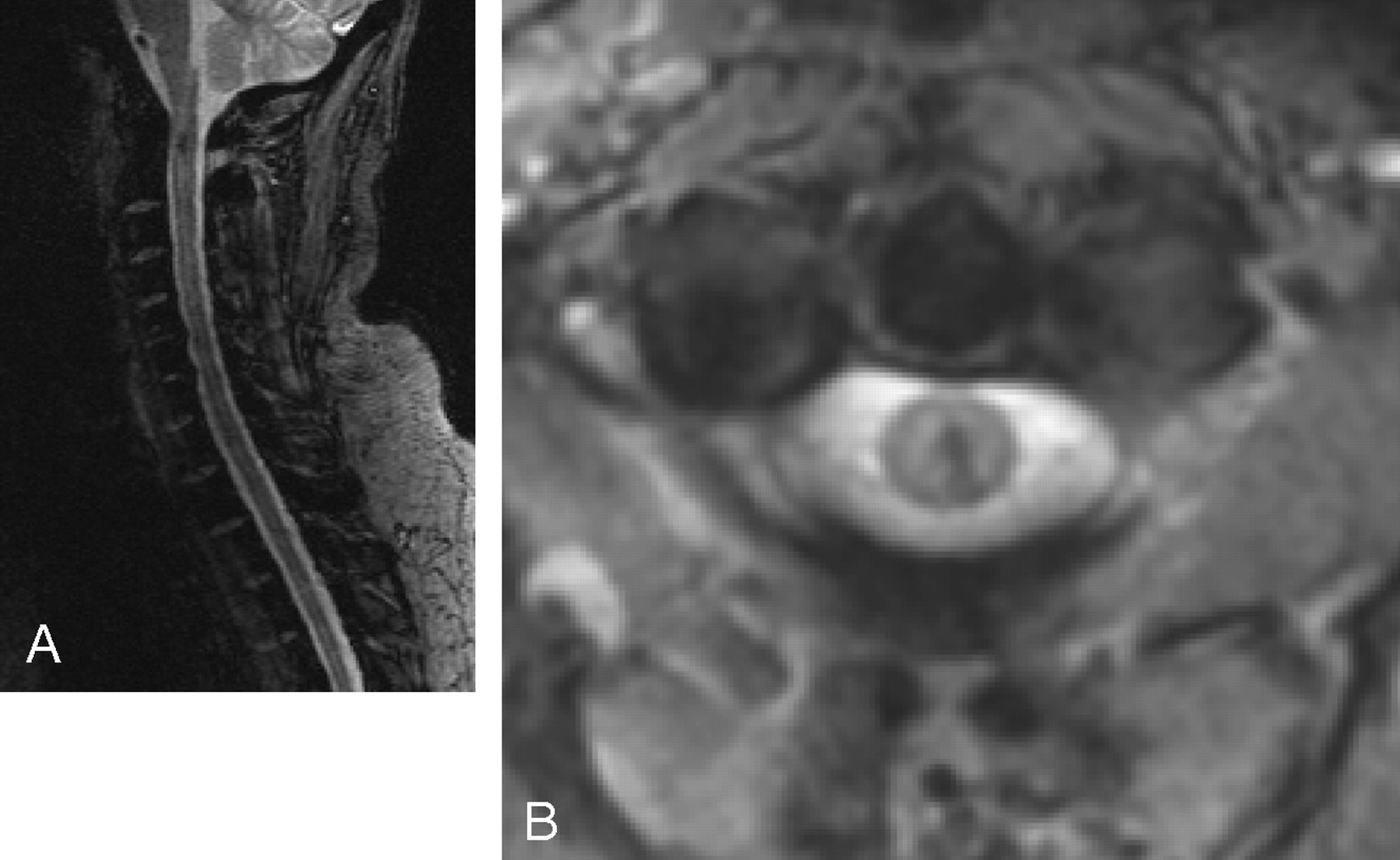
On the first postoperative day, the patient underwent MR imaging examination to document the presence and extent of any cord injury. This study showed relatively minor cord edema and a small amount of cord hemorrhage (Figs 3 and 4). The patient made an uneventful postoperative recovery and remains well.

A and B, Sagittal T2- and T1-weighted MR images showing cord edema on T2-weighted images, with appreciable minor T1-signal-intensity abnormality.

A and B, Sagittal and axial gradient MR images showing a small focus of susceptibility within the cord, compatible with a small focus of cord hemorrhage.
Discussion
The use of acupuncture is becoming increasingly popular among medical and nonmedical therapists. In Australia, at least 15% of general practitioners use acupuncture.1
Treatment with traditional acupuncture consists of the insertion through the skin of solid needles from 15 to 50 mm in length. The depth of insertion varies from a few millimeters to several centimeters. The tip of the needle often lies within muscle; however, many recognized acupuncture points overlie other significant structures.2
Although acupuncture is accepted as an alternative method for the treatment of various medical conditions,3 little has been published regarding the safety and efficacy of self-acupuncture. To our knowledge, few articles in the literature describe major complications from acupuncture such as death or serious disability. Review of the literature revealed 1 reported death of an elderly woman through accidental cardiac tamponade caused by self-needling with a sewing needle through the anterior chest wall.4
Most commentary regarding acupuncture safety refers to acupuncture administered by trained practitioners. As far as we are aware, this is first documented case of spinal cord injury secondary to self-administered acupuncture. With respect to spinal cord or nerve root injury or both, a total 10 cases have been previously documented.2 In 4 cases, migration of broken needle fragments was responsible for the injury. Six cases were caused by direct penetrating injury. The level of the injury varied from C1 to S1. Focal neurologic signs as well as paraplegia have been reported.2 There have been reported cases of arachnoiditis or subarachnoid hemorrhage or both from direct puncture.2
The discrepancy between the puncture level and the neurologic deficits demonstrated in our patient was attributed to a slightly left-of-midline needle tract as demonstrated on the postoperative MR images, with involvement of traversing fibers by adjacent edema. Resolution of deficits was attributed to resolution of edema as well as the small focus of blood products. The potential exists for similar injury in radiologic practice with cervical thecal punctures.
The general complications of acupuncture have been widely documented.2,5,6 More common adverse effects include fainting, nausea, vomiting, bruising, headaches, sweating, dizziness, and needle breakage. Rarer complications include septicemia, punctured organs, and convulsions.5
Conclusion
Spinal cord injury is a rarely reported outcome from trained acupuncturists, and to our knowledge, this is the first reported case from self-administered treatment.
- Received March 26, 2006.
- Accepted after revision May 26, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.