
Abstract
SUMMARY: For anatomic and technical reasons, it is often difficult to achieve guiding-catheter stability in the segmental arteries during embolization of spinal vascular lesions. We have developed a segmental artery exchange technique using a thin-walled 4F nontapered catheter that is safe and achieves a stable guiding-catheter position. This catheter accommodates both the flow-guided and variable-stiffness microcatheters, allowing selective catheterization and treatment of spinal vascular lesions.
A stable guiding-catheter position is extremely important in the endovascular treatment of spinal arteriovenous shunts. For anatomic and technical reasons, it is often difficult to achieve guiding-catheter stability. Important anatomic factors include the diameter and shape of the aorta, the region of interest, and the orientation and size of the segmental arteries. Tortuous and dilated aortic anatomy, especially in the elderly, poses significant problems, and buckling of the guiding-catheters back into the aorta frequently occurs in these patients. Technical factors also affect stability and include catheter selection and size. It is often necessary to use specialized catheters that have complex distal shapes (eg, Cobra 1 and 2 [Merit Medical Systems, South Jordan, Utah], Simmons 1 and 2 [Merit], unique spinal catheters) to catheterize the origin of the segmental arteries. These catheter shapes are often a barrier to distal navigation in the small segmental arteries, and without selective catheterization, stability is frequently a problem. The use of 5F catheters increases the stability; however, they are often too large to position distally in the segmental artery and can produce flow arrest.
We developed a technique that allows us to overcome the problem of guiding-catheter instability in some patients. During the previous 2 months, we encountered 3 patients whose spinal vascular lesions we were unable to treat initially because of guiding-catheter instability. One of the patients had a spinal cord arteriovenous malformation (AVM) with the radiculomedullary artery arising from the left T8, and 2 patients had spinal dural arteriovenous fistulas (DAVFs) from the right T5 and T6 segmental arteries. Each patient was successfully treated with the use of an intercostal artery exchange technique enabling distal stable positioning of a 4F catheter that acted as a coaxial guide. We have found the 4F Berenstein II (Cordis Endovascular, Miami Lakes, Fla) thin-walled nontapered catheter to be small and flexible enough to position distally in the segmental artery and to have sufficient inner diameter (0.042 inches) to accept the Magic 1.2 FM (Balt, Montmorency, France) and Prowler 10 (Cordis Endovascular) microcatheters that we use in spinal embolization. The purpose of this short communication is to describe our initial experience using this segmental artery exchange technique to facilitate stable positioning of a 4F guiding catheter in the segmental artery supplying spinal arteriovenous shunts.
Description of the Technique
Embolization procedures were performed with the patient under general anesthesia and systemic heparinization (100 U/kg intravenously). Our procedure involved a single femoral puncture access with a 5F sheath. Diagnostic spinal angiography was performed with several specialized catheters, including 4F or 5F Cobra 1 and 2 and Simmons 1 and 2. The choice of catheter depended on the aortic anatomy and orientation of the segmental artery orifice. After identifying the segmental artery supplying the spinal lesion, we then navigated a 260-cm exchange-length 0.035-inch angled Glidewire (Terumo Medical, Somerset, NJ) distally into the segmental artery under roadmap conditions (Fig 1). A torque device aided distal placement. The angiography catheter was removed and exchanged for the 4F Berenstein II catheter. This catheter has the following features: length of 100 cm, inner diameter of 0.042 inches, short primary curve angle of approximately 70° to the shaft, and 0.038-inch guidewire compatibility.

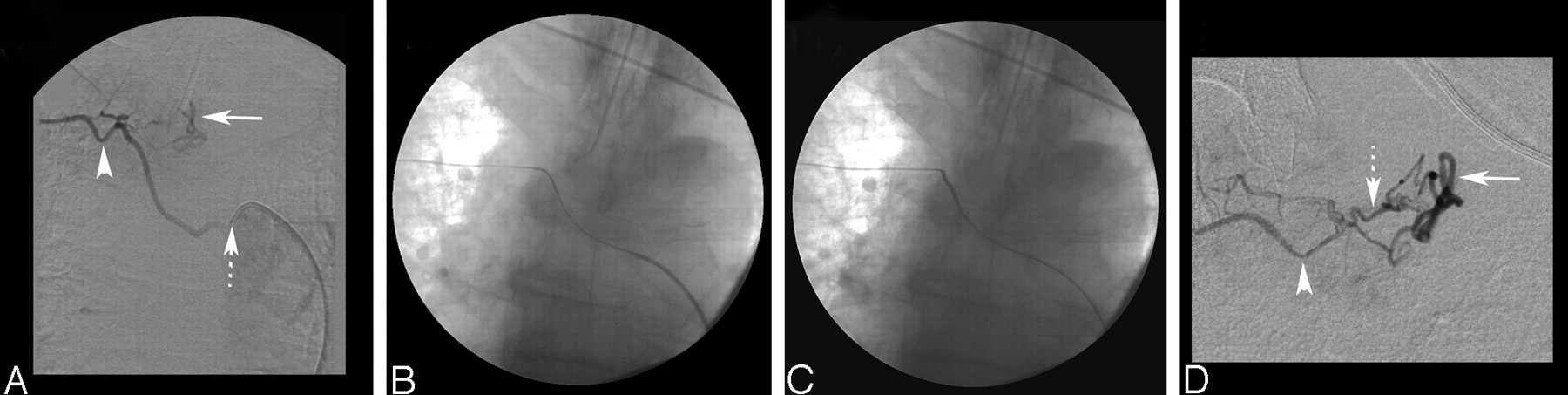
A, Selective right T6 intercostal artery digital subtraction angiogram (DSA) showing a DAVF. The dotted arrow points to the position of the 5F Cobra 2 catheter at the orifice of the right T6 intercostal artery. Note the size of the 5F catheter relative to the small size of the T6 intercostal artery (arrowhead). The solid arrow indicates the perimedullary vein. B, Nonsubtracted film shows the 0.035-inch Terumo exchange-length wire in the right T6 intercostal artery. C, Final distal position of the 4F guiding catheter with the exchange wire in situ. D, Superselective DSA through a Magic 1.2FM microcatheter shows the right T6 intercostal artery (arrowhead), the dural branch supplying the fistula (dotted arrow), and the draining perimedullary vein (solid arrow).
The catheter was positioned distally in the segmental artery, as close as possible to the origin of the dural or radiculomedullary arteries supplying the vascular lesion (Figs 1 and 2). A Magic 1.2 FM microcatheter or Prowler 10 was then easily tracked without friction though the 4F catheter in all patients. The Magic microcatheter advancement was supported with a 0.008-inch guidewire (Mirage 008, ev3, Irvine, Calif), and the Prowler 10 microcatheter advancement was supported with a 0.010-inch guidewire (Transend 10, Boston Scientific/Target Therapeutics, Fremont, Calif), allowing selective catheterization of the main arterial branches feeding the lesion. The stable guiding-catheter position greatly improved the push ability of the microcatheter. Roadmap injections could not be performed through the 4F catheter with the microcatheter in place; however, roadmap injections through the microcatheter could be performed. We have not found this feature to be a limitation. In all 3 patients, treatments were considered successful in that the planned treatments were completed.

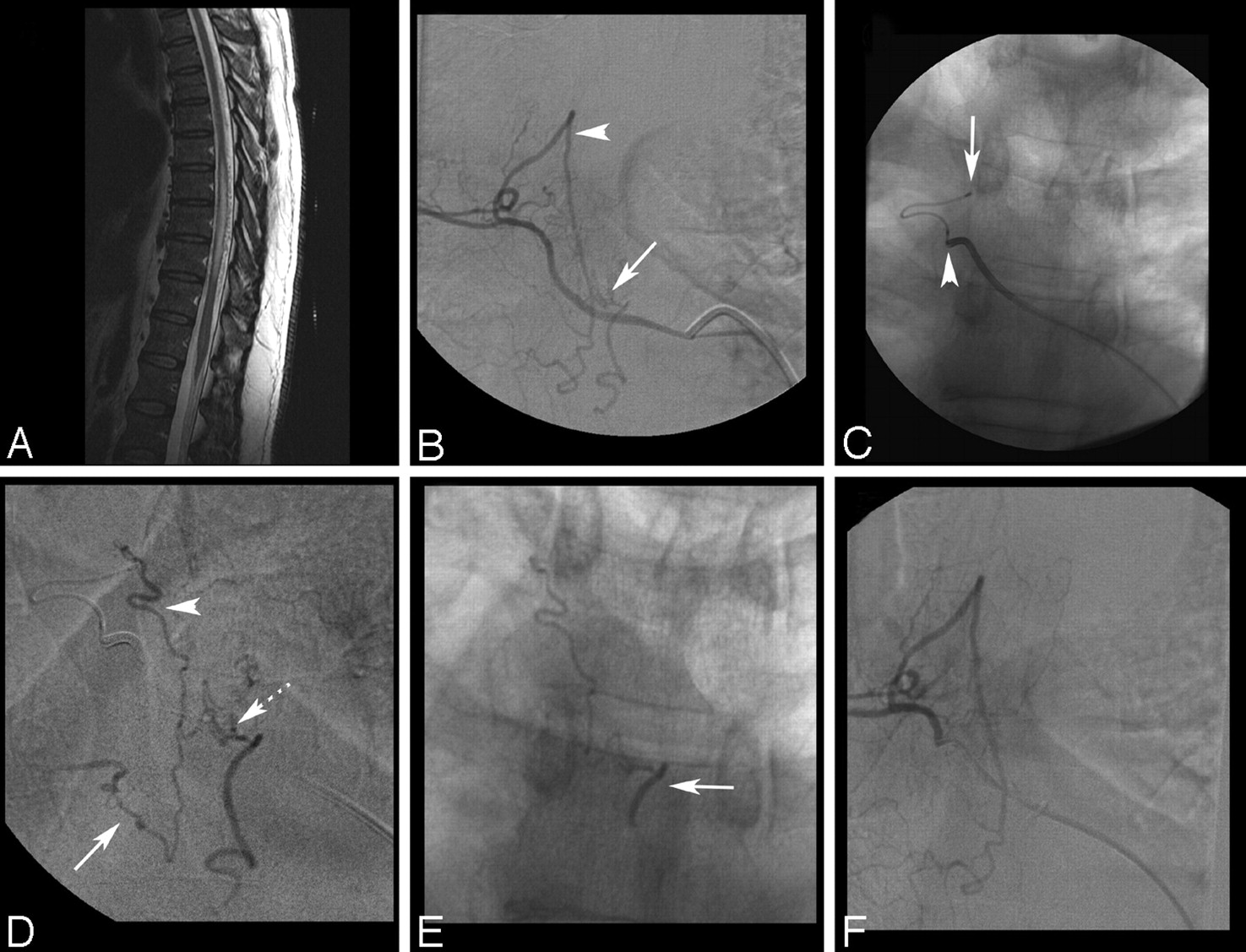
A, Sagittal T2-weighted MR image shows diffuse edema and mild expansion of the thoracic cord from T6 to T12. Extensive vascular flow voids are seen intradurally behind the spinal cord, suggesting a DAVF. B, Selective right T5 intercostal artery DSA shows the DAVF as it drains into a perimedullary vein (arrow). The arrowhead indicates a prominent retrolaminar muscular branch. C, Nonsubtracted film shows the distal position of the 4F catheter in the right T5 intercostal artery after the exchange procedure (arrowhead) and the selective position of a Prowler 10 microcatheter in the dural branch feeding the fistula (arrow). D, Superselective DSA through the microcatheter shows a bimetameric supply to the fistula from the right T5 (arrowhead) and T6 (solid arrow) dural branches. The dotted arrow marks the fistulous point. E, Nonsubtracted x-ray shows the glue cast reaching the draining perimedullary vein (arrow). F, Selective right T5 segmental artery DSA confirms disconnection of the dural AVF.
Discussion
Embolization of spinal DAVFs and AVMs can be difficult because of tortuosity and the small diameter of the feeder and distal location of the fistula site. A meta-analysis found that only approximately 46% of patients who underwent embolization were successfully treated.1 Oran et al2 used a triple-axial technique (a guiding catheter inside a long vascular sheath) to improve the proximal stiffness and enhance the push ability of the microcatheter; however, this technique required the use of a 7F vascular sheath. Touho et al3 described successful endovascular treatment of a spinal DAVF at the L5-S1 level by using a thin-walled nontapered 4F catheter (Glidecath II, Terumo) and Tracker-18 microcatheter (Target Therapeutics). This fistula was fed from dural branches of the internal iliac artery and therefore likely had anatomy that favored catheter stability. The advantages of our exchange technique are that it is compatible with a short 5F femoral sheath, that it allows guiding-catheter stability in segmental arteries arising from the aorta, and that it enables distal safe placement of a 4F guiding catheter in small segmental arteries close to the origin of the radicular or dural arteries feeding a vascular spinal lesion.
We have bench-tested the 4F Berenstein II catheter and found it large enough to accommodate the Magic catheter range (proximal/distal outer diameter [OD]: 2.7F/1.2–1.8F) and the Prowler catheter range: Prowler 10, 14, and the larger Prowler Plus (proximal/distal OD: 2.9F/2.3F). It likely will accept other microcatheters with a proximal OD of 2.9F or smaller. Its simple shape necessitates selective catheterization of the orifice of the segmental artery by using specialized spinal angiographic catheters. Its inner diameter is not sufficient to allow the Spinnaker Elite (Boston Scientific) catheters (proximal/distal OD: 3.0F/1.8F or 1.5F) to pass without friction. A 5F guide should be used if these specific flow-directed catheters are required. This exchange technique may allow patients to the receive endovascular treatment that would not be feasible with standard catheters used for spinal angiography.
- Received November 29, 2006.
- Accepted after revision November 30, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.