
Abstract
BACKGROUND AND PURPOSE: Patients undergoing parenteral nutrition and those with portosystemic encephalopathy secondary to chronic liver disease and acquired and congenital portosystemic venous shunts frequently present manganese deposition in the basal ganglia, detected by MR imaging as hyperintense areas on T1-weighted sequences. We also observed similar abnormalities in the basal ganglia of patients with chronic renal failure undergoing maintenance hemodialysis. Our aim was to evaluate the pallidal signal intensity on T1-weighted images in a series of patients undergoing hemodialysis, with further evaluation of serum manganese levels and neurologic correlation, comparing them with patients with chronic renal failure without dialytic treatment.
MATERIALS AND METHODS: We performed MR imaging examinations in 9 patients with chronic renal failure, 5 of whom were undergoing hemodialysis. An experienced neuroradiologist scrutinized the presence of symmetric hyperintensities in the basal ganglia on T1-weighted sequences. We also determined the serum manganese levels and performed the neurologic evaluations in all patients.
RESULTS: All patients undergoing hemodialysis presented elevated serum manganese levels and symmetric hyperintensities within the globus pallidus. In this group, 4 patients presented with parkinsonian symptoms, myoclonus, and syndromes with vestibular and vestibular-auditory symptoms. The patients without dialytic treatment presented with neither bilaterally increased T1 MR imaging signal intensity within the globus pallidus nor symptoms of manganism.
CONCLUSION: Our preliminary results demonstrated the occurrence of bilateral pallidal hyperintensity on T1-weighted images in all patients undergoing hemodialysis associated with high serum manganese levels, revealing a new association.
Patients undergoing parenteral nutrition and those with portosystemic encephalopathy secondary to chronic liver disease and acquired and congenital portosystemic venous shunts frequently present manganese accumulation in the adenohypophysis and in specific regions of the brain, more precisely in the globus pallidus, putamen, subthalamic region, substantia nigra, and sometimes diffusely in hemispheric white matter.1–7 A biologic marker of manganese accumulation within the central nervous system (CNS) is bilaterally increased T1 MR imaging signal intensity within the basal ganglia, especially in the globus pallidus but also in the striatum.8–21 Recently, some authors have described the same pattern of manganese accumulation in welders, secondary to inhalation of ambient welding fumes with reported inadequate ventilation or other safety measures.10,15–17 Although T1 signal-intensity changes in these nuclei may be seen in several different conditions such as nonketotic hyperglycemic episodes, hypoxia, neurofibromatosis, calcium accumulation, Wilson disease, and the early phase of kernicterus, it is an uncommon pattern.22–27 Manganese neurotoxicity presents commonly as a parkinsonian syndrome,6,10,11,15–17,28–31 although a syndrome of multifocal myoclonus and limited cognitive impairment, a mixed syndrome with vestibular-auditory symptoms, and a minor syndrome with subjective cognitive impairment, anxiety, and sleep apnea were also described in this setting.15 We have observed a similar pattern of bilaterally increased T1 MR imaging signal intensity restricted to the globus pallidus of patients with chronic renal failure undergoing hemodialysis. The reason for this phenomenon is, as yet, unclear, and we presume that these signal-intensity abnormalities may also reflect manganese accumulation in the CNS, which should raise important questions concerning the prevention of manganism in this setting.
Our aim was to evaluate the pallidal signal intensity on T1-weighted images, to perform neurologic correlation based on an active search for symptoms related to manganism, and to determine the serum manganese levels of a series of patients undergoing maintenance hemodialysis, comparing these individuals with patients with chronic renal failure without dialytic treatment.
Methods
Our institutional review board approved this study, and we obtained informed consent from all patients. At a minimum, all patients had blood studies (complete blood count; chemistry profile; total serum protein levels; bilirubin levels; hepatitis B, C, and HIV tests; iron studies; and thyroid, parathyroid, liver, and renal function tests). Our hemodialysis unit is in accordance with the laws of The National Sanitary Vigilance Agency.
We performed brain MR imaging at 1T in all patients. After 3 localizing scans in the axial, coronal, and sagittal planes, axial sections covering the whole brain were aligned with the bicommissural line. Imaging parameters were identical (24-cm FOV, 6-mm thickness, 0.6-mm gap, 205 × 512 matrix). Our protocol included an axial turbo spin-echo (TSE) fluid-attenuated inversion recovery (FLAIR) sequence (TR, 11,000 ms; TE, 140 ms; TI, 2600 ms, TSE factor, 29) and a spin-echo acquisition to obtain T1-weighted images (TR, 509 ms; TE, 14 ms). We also performed an axial T2* sequence (TR, 615 ms; TE, 21 ms; flip angle, 15°) to exclude hemorrhagic lesions in the basal ganglia. For each patient undergoing hemodialysis, we additionally performed an axial nonenhanced brain CT (20-cm FOV, 5-mm infratentorial and 10-mm supratentorial thickness, 512 × 512 matrix) to exclude prominent calcifications in the basal ganglia and an abdominal Doppler ultrasonography to exclude hepatic portosystemic venous shunts.
The inclusion criteria were the following: in patients who agreed to participate in this protocol, serum creatinine level above 1.5 mg/dL and creatinine clearance below 60 mL per minute. We included only individuals who had undergone hemodialysis for more than 2 years. The exclusion criteria were the following: MR imaging contraindication; positive tests for hepatitis B, C, or HIV; hepatic failure; hepatic portosystemic venous shunt or biliary obstruction on abdominal Doppler ultrasonography; elevated serum bilirubin levels; detection of exuberant calcifications or hemorrhage in basal ganglia on CT or MR imaging; total parenteral nutrition; and welding activity.
From January to May 2006, we consecutively enrolled 9 patients (5 men) with chronic renal failure at our institution, 5 of whom were undergoing maintenance hemodialysis. An experienced neuroradiologist (A.J.R.), blinded for clinical data, analyzed the MR images and CT scans of each patient independently. The films were presented in random order (not sequential) without identification. MR imaging and CT studies were not presented together, and he searched for the presence of bilaterally increased T1 MR imaging signal intensity within the basal ganglia, especially in the globus pallidus. We obtained serum manganese levels of all patients by means of atomic absorption spectrophotometry and considered values above 0.85 ng/mL as elevated. An experienced neurologist (M.F.M.), blinded for imaging data, performed neurologic correlation in all patients based on an active search for symptoms related to manganism.
Results
Clinical data, serum manganese levels, and some blood study results are summarized in Tables 1 and 2.
Clinical data and serum manganese levels of the 9 patients with chronic renal failure
Serum creatinine, BUN, hemoglobin, hematocrit, albumin, and calcium levels of the 9 patients with chronic renal failure
Patients 8 and 9 presented with low albumin levels (normal range, 3.5–5.5 g/dL) due to associated nephrotic syndrome. In the dialytic group, patients 2 and 4 presented with hypercalcemia (normal range, 8.5–10.2 mg/dL), but none of those showed calcifications in the basal ganglia on CT scans. Only 1 individual in this group (patient 1) presented with faint bilateral foci of calcification in the medial aspect of the globus pallidus on CT, also demonstrated as small marked hypointense foci on T2* sequences (Fig 1). All patients undergoing hemodialysis presented with high serum manganese levels and bilateral pallidal hyperintensities on T1-weighted images (Fig 1). None of the patients without dialytic treatment presented with such signal-intensity abnormalities on MR imaging (Fig 2), though 2 of them presented with elevated serum manganese levels. In the nondialytic group, only patient 7 presented with hypercalcemia, and her MR images showed small bilateral foci of marked hypointensity in the medial aspect of the globus pallidus on T2* sequences.

Patient 1. A, Axial T1-weighted image shows bilateral and symmetric hyperintensities within the globus pallidus (arrows). B, Axial FLAIR imaging finding is normal. C, CT image shows faint bilateral foci of calcification in the medial aspect of the globus pallidus (arrows), with precise correspondence on the T2* (D) sequence (arrows).

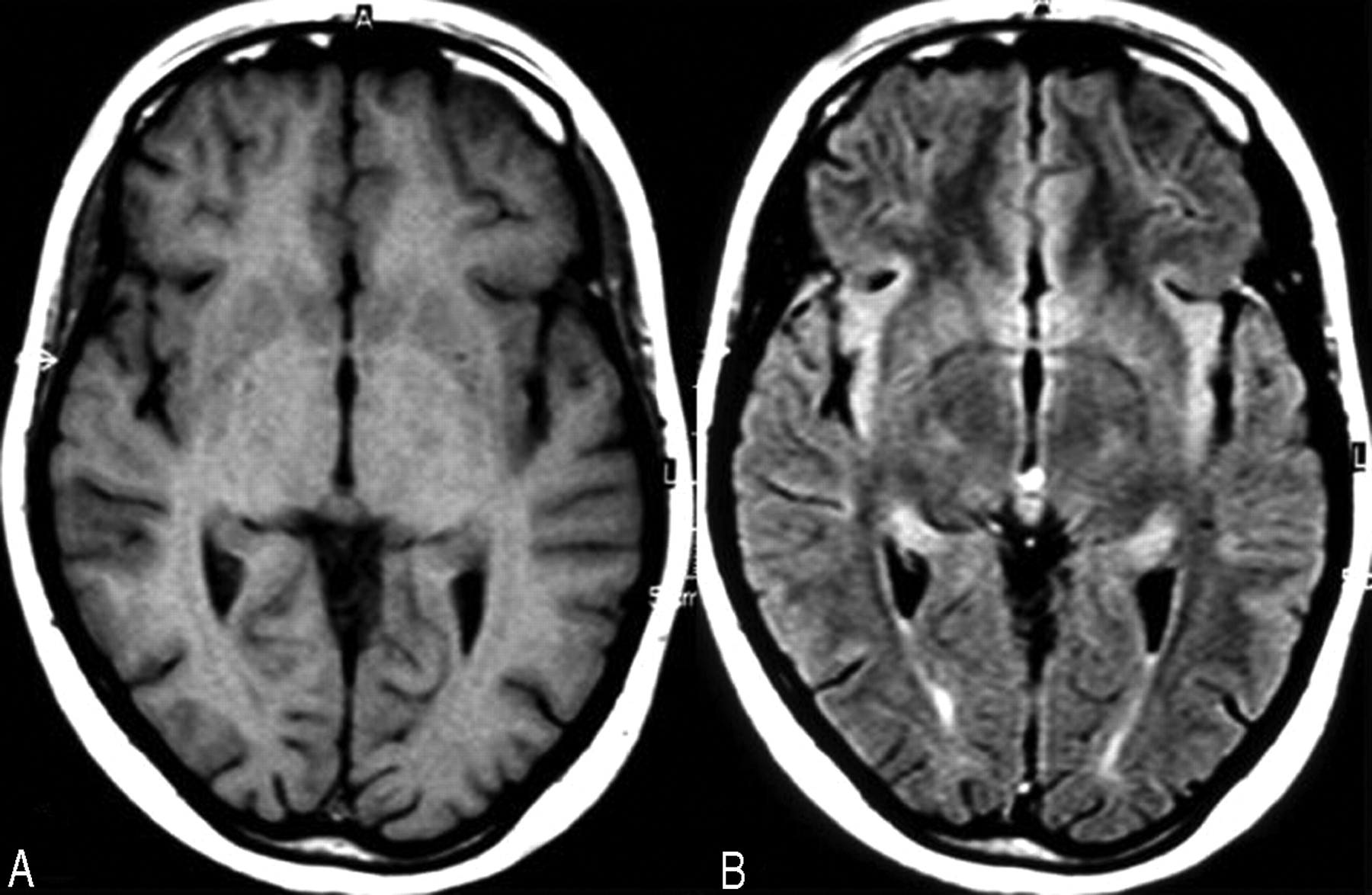
Patient 8. Axial T1-weighted (A) and FLAIR (B) images do not show any signal-intensity abnormality.
The results of the remaining blood studies (not shown) were unremarkable. None of our patients received oral supplements rich in manganese, and all of them had hydric restriction, hypokalemic and hyposodic diets, and oral supplements of vitamin B and folic acid. Our patients without dialytic treatment also had a hypoproteic diet.
On the basis of the neurologic examination, we recognized 2 different clinical syndromes, parkinsonian symptoms and myoclonus, in 4 of 5 patients undergoing hemodialysis as follows:
Mixed Syndrome with Vestibular-Auditory Symptoms. Patient 1 related left hearing loss, disequilibrium, and tinnitus for more than 5 months, confirmed by neurologic examination. Her brain stem did not show any signal-intensity abnormalities on MR imaging.
Vestibular Syndrome. Patient 2 related disequilibrium for more than 1 year and occasional left-gait deviation, confirmed by neurologic examination. His brain stem did not show any signal-intensity abnormalities on MR imaging.
Parkinsonian Symptom. Tremor was the clinical presentation in patients 1 and 5. In patient 1, tremor was greater in the upper extremities and at the end of movements for more than 5 months. In patient 5, there was only a slight and inconstant rest tremor in the upper extremities.
Myoclonus. Patient 4 presented a prominent myoclonus only in the right upper limb, causing motor dysfunction for more than 1 year.
The findings of neurologic examinations of the remaining patients were unremarkable.
Discussion
A biologic marker of manganese accumulation within the CNS is bilaterally increased T1 MR imaging signal intensity within the basal ganglia, especially in the globus pallidus.8–21 In patients undergoing hemodialysis, serum manganese concentration is reported to be low, compared with that in the healthy population,32 and the reason is thought to be removal of manganese from blood during hemodialysis. It, thus, theoretically is reasonable that manganese intoxication would be unlikely in patients undergoing hemodialysis if the dialysate is not severely contaminated by manganese. In our institution, the dialysate contains no detectable manganese. Therefore, manganese intoxication was not caused by contamination of the dialysate, unlike the case reported by Taylor and Price.33 Manganese (Mn) circulates in the blood as Mn3+ bound tightly to transferrin or Mn2+ (the free ion or bound to such plasma proteins as albumin).34 The main route of manganese excretion is thought to be through the biliary tract,35 and urinary excretion is thought to be negligible.36 Therefore, anuria caused by renal failure may not influence manganese metabolism.
Recently, Ohtake et al37 described manganese-induced parkinsonism in a man with diabetic nephropathy undergoing maintenance hemodialysis, in whom the cause of manganese accumulation was the intake of an oral supplement (Chlorella organism extract) rich in this trace metal. The authors showed MR imaging findings characterized by symmetric basal ganglia hypointensity on T1-weighted and hyperintensity on T2-weighted images and attributed these signal-intensity abnormalities to manganese accumulation in the CNS. However, these controversial MR imaging findings are quite different from the classic pattern of manganese accumulation causing increased T1 MR imaging signal intensity within the basal ganglia, especially in the globus pallidus.8–21 We agree that manganese accumulation within the basal ganglia induced parkinsonian symptoms secondary to an overload of this trace element from dietary intake, as postulated by the authors. However, the relationship between the previously mentioned signal-intensity abnormalities on MR imaging and elevated serum manganese levels was not established in this particular case. On the other hand, there are other metabolic dysfunctions induced by hemodialysis that cause MR imaging findings quite similar to those described by Ohtake et al,37 such as the syndrome of acute bilateral basal ganglia lesions in patients with diabetic uremia38 and osmotic demyelination syndrome in end stage renal disease after recent hemodialysis.39,40
To the best of our knowledge, this is the first time that manganese accumulation in the CNS has been demonstrated by MR imaging in patients undergoing maintenance hemodialysis. As suggested by Ohtake et al,37 some possibilities exist with respect to abnormal manganese accumulation in this setting: disturbance of excretion through the biliary tract, increase in protein-bound (undiffusible) manganese that is not removed by hemodialysis, excessive manganese intake that exceeds the excretory capacity, and the effect of uremia on manganese metabolism. Biliary excretion was thought to be normal in our patients because none of them had liver dysfunction or biliary tract obstruction according to laboratory tests and abdominal ultrasonography, respectively. An elevated protein-binding rate of manganese also was thought to be unlikely. Although the exact level of protein binding could not be measured in these patients, it is reported to be decreased significantly in patients with uremia.41 Excessive manganese intake seems to be a plausible explanation even in the absence of oral supplements rich in this trace metal in our group of patients. Although 2 of our 4 patients without dialytic treatment had slightly elevated serum manganese levels, probably secondary to dietary intake, they did not have manganese accumulation in the basal ganglia demonstrated by MR imaging. However, all of our patients undergoing hemodialysis had elevated serum manganese levels and pallidal T1 hyperintensities demonstrated by MR imaging, even in patient 2, in whom the serum manganese elevation was discrete.
The absence of striking blood manganese elevations in the setting of clinical manganese toxicity is not unexpected.8,30 Although the behavior of manganese in the blood stream of humans has not been well characterized, available evidence suggests that measured serum manganese primarily reflects that which is protein bound. When circulating proteins are saturated, free manganese rapidly binds to other tissues or is rapidly excreted from the body.42,43 Thus, free manganese does not accumulate in the circulation.44 Consequently, serum manganese levels do not correlate with the intensity of exposure.15 Theoretically, patients with hypoalbuminemia tend to present with low serum manganese levels. Despite the questions raised previously, our 2 individuals with hypoalbuminemia (patients 8 and 9) had high serum manganese levels. The reason for this finding remains unknown.
We believe that manganese dietary intake (excessive or not) is necessary for accumulation of manganese in the basal ganglia, notably within the globus pallidus. However, hemodialysis might play an important role in this setting. Our findings are in line with those reported by Schabowski et al,45 who described the manganese content in patients undergoing long-term hemodialysis as significantly increased postmortem. The brain manganese level is reported to exceed that in plasma by more than 100-fold,46 so selective binding or active transport may promote manganese uptake by the brain in patients undergoing long-term hemodialysis. Manganese transport channels include transferrin receptor-dependent binding or transport through the Ca2+ channel, Na+/Ca2+ exchanger, and Na+/Mg2+ antiporter.35 Particularly, the basal ganglia are the site of abundant transferrin receptors.35 Some unknown mechanisms related to hemodialysis may lead to manganese accumulation in the brain of these patients, probably due to dysfunction of the previously mentioned manganese transport channels. Although our understanding of the cellular compartmentalization of manganese under in vivo pathologic conditions is uncertain, in vitro findings indicate that glial cells possess a high-affinity transport mechanism for manganese47 and have the capacity to accumulate manganese by up to 200 times the extracellular concentration.48 Additional studies have revealed that 60%–70% of the accumulated manganese is sequestered in mitochondria, whereas the rest is localized to the cytosol.49 Thus, current evidence suggests an involvement of mitochondria in astrocytes in the neuropathology of manganese neurotoxicity.
Quite similar to authors of a previous study,15 we observed heterogeneous symptoms in those 4 symptomatic patients undergoing hemodialysis. As previously described by Josephs et al,15 2 clinical syndromes, parkinsonian symptoms and myoclonus, have also emerged in our preliminary results; parkinsonism has been reported in manganese toxicity by several authors.6,10,11,15–17,28–31 Myoclonus (depicted in patient 4) has only been documented in 3 patients with manganism so far.9,15 Although auditory and vestibular symptoms have been reported in manganese toxicity,30,50,51 they were not related to a particular syndrome, except by Josephs et al.15 Quite similar to this previous study, 1 of our patients (patient 1) undergoing hemodialysis had prominent vestibular-auditory symptoms associated with evident deficits on neurologic examination. Another presented evident vestibular symptoms confirmed by neurologic examination. Myoclonus and vestibular-auditory symptoms, though uncommon, seem to be plausible associations with manganism. Additionally, these symptoms never presented exacerbations during or immediately after dialytic procedures. However, the precise clinical spectrum of manganese neurotoxicity requires further studies and confirmation. Nevertheless, all symptoms were depicted only after an active search by an experienced neurologist.
Rodent data suggest that iron deficiency and anemia may be risk factors for manganese neurotoxicity.19 We have a small sample to perform a reliable statistical analysis among iron deficiency, anemia, and manganism. However, we considered serum hemoglobin levels below 10 g/dL as anemia in the setting of chronic nephropathy. In our series, we had 5 anemic individuals (patients 2, 4, 6, 7, and 9). Patients 2 and 4 presented symptoms of manganism (dialytic group). On the other hand, patients 1 and 5 were not anemic and also presented symptoms of manganese neurotoxicity (dialytic group). Patients 6, 7, and 9 were asymptomatic (nondialytic group). We think that there are not enough data to corroborate this association in our patients. The main risk factor for manganism seems to be maintenance hemodialysis in this setting.
Calcium deposits can accumulate in the basal ganglia of patients with chronic renal failure secondary to parathyroid hyperfunction. Unfortunately, it is not possible to demonstrate any statistical difference in serum calcium levels between the dialytic and nondialytic groups because of the small number of patients. In previous studies, the presence of high signal intensity on T1-weighted images has been demonstrated in association with cerebral parenchymal calcification, possibly reflecting the incorporation of paramagnetic ions or altered effects of hydration.25 Although CT studies in our patients undergoing hemodialysis demonstrated no change to correlate with regions of high pallidal MR signal intensity, the presence of increased calcium or other metal ions cannot be completely excluded. Postmortem analysis, not available in our series, would have been useful in evaluating these possibilities.
A limitation of our preliminary results is the small number of patients, but more individuals are being studied and an age- and sex-matched healthy control group will soon be included in this protocol. Without the widespread availability of dialysis and kidney transplantation, many lives would have ended prematurely; however, we consider our findings consistent enough to raise attention to manganese accumulation in the CNS in patients undergoing maintenance hemodialysis, causing symptoms related to manganism and increasing their morbidity.
Conclusion
Our preliminary results showed that the bilaterally increased T1 MR imaging signal intensity depicted in the globus pallidus of our patients undergoing hemodialysis could reflect manganese accumulation in the CNS, revealing a new association. Although this signal-intensity abnormality has a weak correspondence with high serum manganese levels, almost all patients undergoing hemodialysis showed signs attributable to manganism. The reason for this accumulation is yet unclear, probably related to both dysfunction of manganese transport channels facilitated by dialytic therapy and dietary intake of this trace metal. However, we have a limited number of patients, and our findings describe only an association. It would be necessary to provide further proof, such as evidence from postmortem pathology studies.
Acknowledgments
We thank Fleury Centro de Medicina Diagnóstica for the free analysis of serum manganese levels of all patients.
References
- Received November 16, 2006.
- Accepted after revision December 30, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.