
Abstract
SUMMARY: We report a case of a swallowed partial denture in a 51-year-old man who presented with progressive dysphagia, odynophagia, and fevers. Imaging studies were initially interpreted as supraglottitis with laryngeal inflammation, which was confirmed by direct visualization with flexible endoscopy. Despite appropriate therapy, the patient's symptoms persisted and rigid laryngoscopy was performed, which revealed a partial denture in the hypopharynx and upper esophagus. The subtle imaging appearance of a swallowed denture is discussed.
Aspiration or ingestion of a foreign body has frequently been reported in the pediatric population; however, it is not uncommon in the adult population. In children, coins account for most esophageal foreign bodies, whereas in adults, bones and boluses of meat have commonly been reported as the cause. However, in the elderly population, dental prostheses account for most esophageal foreign bodies.1–3 The base used in the construction of dental prostheses is methylmethacrylate, which is radiolucent. This radiolucency complicates early diagnosis of an impacted or ingested dental prosthesis. We present the radiologic findings of unsuspected impaction of a partial denture in a 51-year-old man with perforation of the posterior cervical esophageal wall.
Case Report
A 51-year-old white man with a history of alcohol abuse and hepatitis C presented to the emergency department with complaints of dysphagia and odynophagia. He reported that his symptoms started suddenly 2 days before and had progressively worsened to the point that he was unable to swallow solid foods and had difficulty with liquids. Despite his symptoms, he continued to drink up to half a pint of vodka daily. He reported subjective fevers and chills and denied a history of hematemesis or hemoptysis. His past medical history was otherwise unremarkable.
On physical examination, the patient was noted to be afebrile and vital signs were stable. Physical examination of the head and neck demonstrated no evidence for pharyngeal erythema, edema, or exudates. The patient did have mild tenderness to palpation in the lower cervical and laryngeal regions bilaterally, left greater than right. Several 5-mm cervical lymph nodes were palpable on the left side. Initial laboratory studies demonstrated slightly elevated WBC of 13.9 with left shift (neutrophils, 10.9). He also had a blood alcohol level of 45 mg/dL (0.045%).
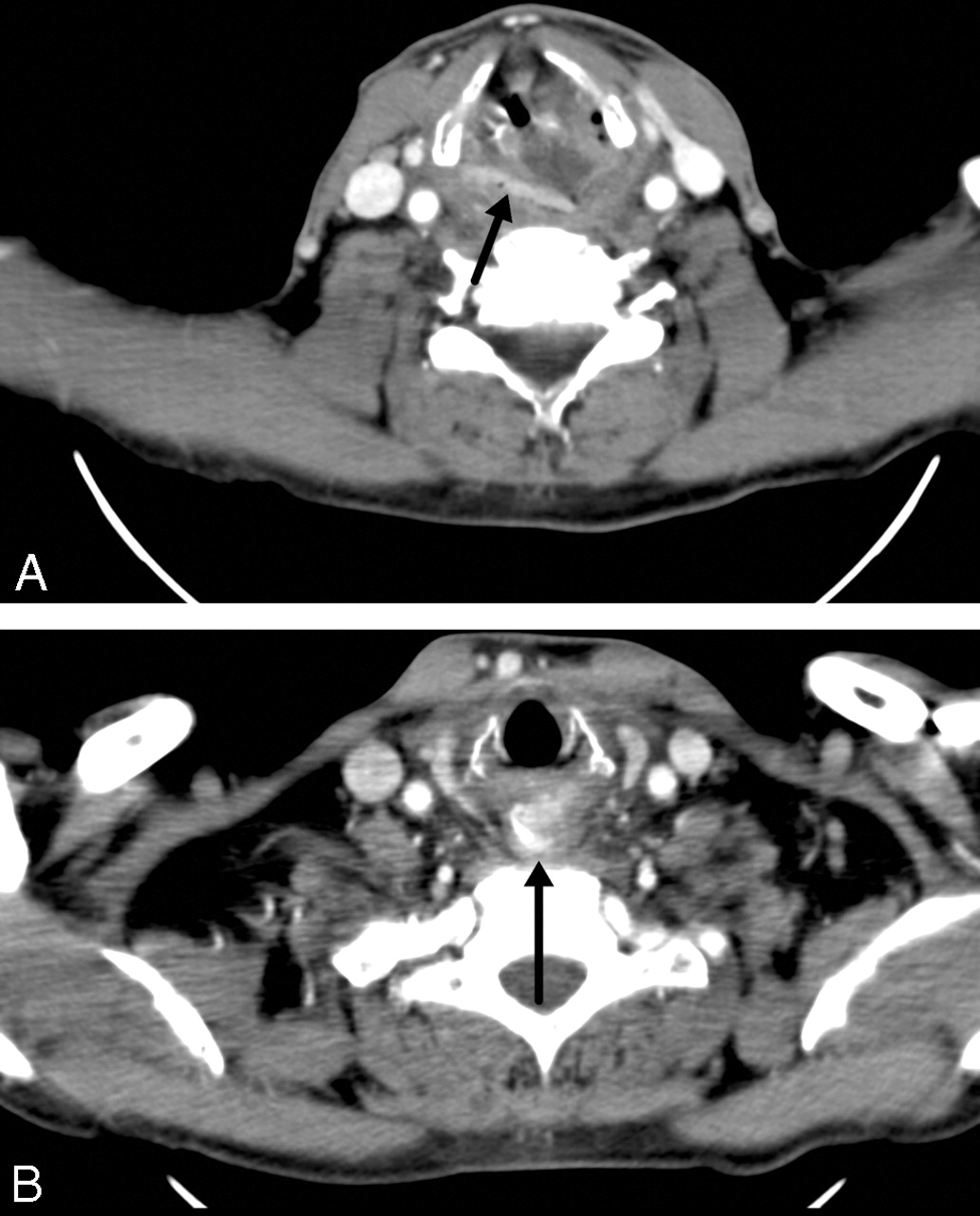
Given the above findings, there was clinical concern for an infectious cause and formation of a retropharyngeal abscess. Anteroposterior and lateral radiographs of the neck were obtained and demonstrated mild prevertebral soft tissue swelling in the lower cervical region. Contrast-enhanced CT scans in Figs 1A and B demonstrated distortion of the epiglottis and aryepiglottic folds. No radiopaque foreign bodies were prospectively identified, and there was no definite formation of an abscess. Given the concern for a neoplastic process, an ENT consultation was obtained. A laryngoscopy was performed, which demonstrated inflammatory change involving the epiglottis. The patient was admitted for supraglottitis and was started on intravenous ampicillin/sulbactam and dexamethasone.

A,B. Contrast-enhanced CT scan of the neck demonstrates extensive soft tissue edema. At the level of the vocal cords, there is a linear attenuation (arrow on A), which was not initially noted but, in retrospect, is felt to likely represent the base plate of the partial denture. In addition, a radiopaque attenuation (arrow on B) is seen in the esophagus at the level of the thoracic inlet, likely representing a tooth.
Despite adequate treatment, his symptoms persisted 5 days later and a flexible endoscopy was performed. On second examination, there was a concern for a masslike lesion and the patient underwent intraoperative rigid endoscopy, which revealed a tooth attached to a partial denture in the larynx (Fig 2). This obstruction was removed without difficulty.

Retrieved removable partial denture.
On retrospective review of CT scan, the linear attenuation seen in Fig 1A is felt to represent the base plate of the partial denture and the rounded radiodensity at the thoracic inlet, the single tooth. These findings could not be appreciated on the radiographs, likely because of superimposition with the thoracic spine.
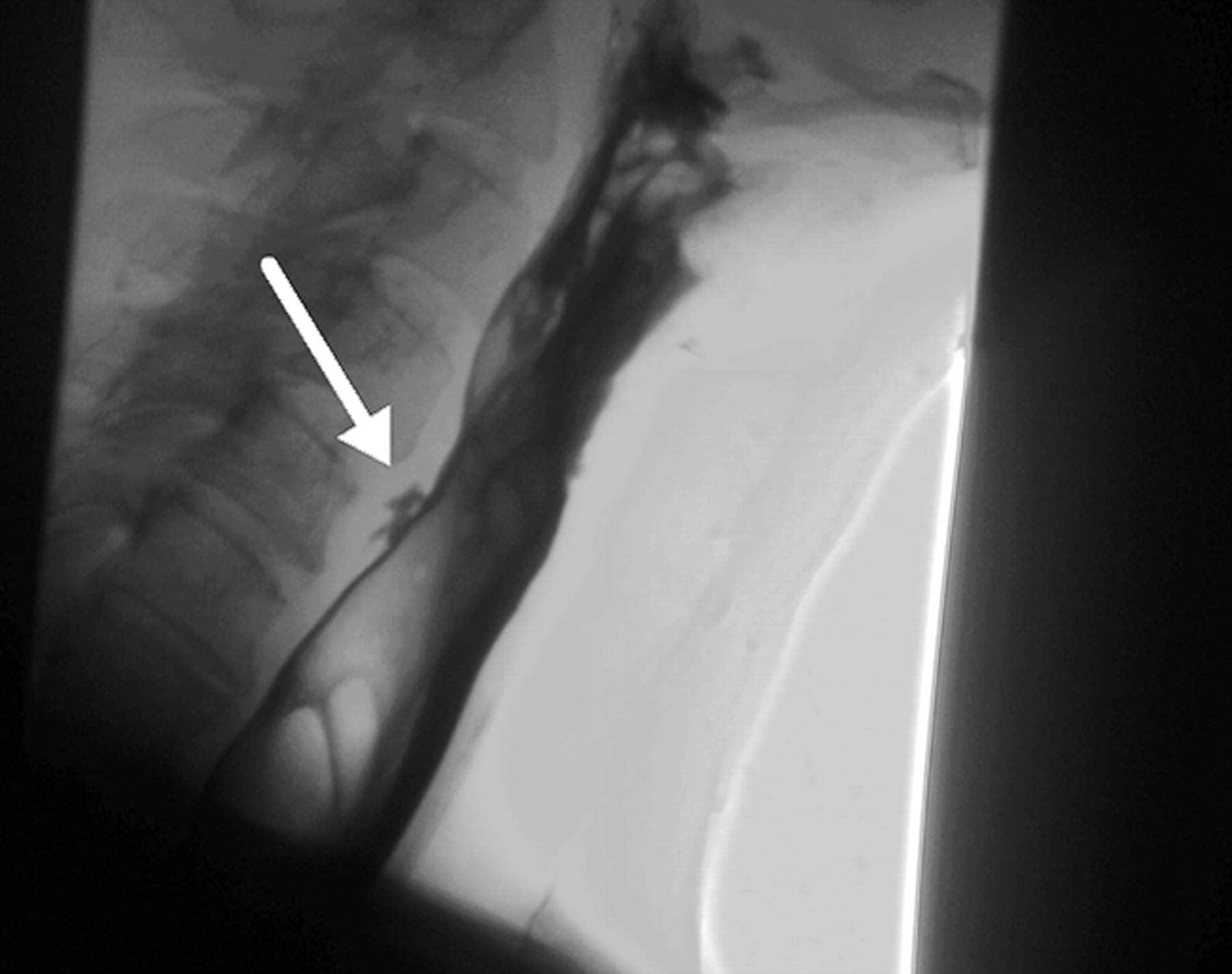
After the partial denture was retrieved, a water-soluble esophagram was performed, which showed contrast extravasation posteriorly (Fig 3). The remainder of the patient's hospital stay was uneventful, and repeat esophagram showed the leak to be contained and significantly decreased in size. On discharge, his symptoms had resolved and he was tolerating oral intake well.

Water-soluble esophagram (Omnipaque 240; GE Healthcare, Piscataway, NJ) demonstrates a small intramural tear (arrow) of the cervical esophagus at the C5 level with contrast extravasation.
Discussion
According to the National Health and Nutrition Examination Survey (NHANES III), 1 of every 5 persons between the ages of 18 and 74 years has full or partial dentures.4 The inadvertent swallowing of a dental prosthesis is not uncommon in the adult population. In a study by Abdullah et al2 of 200 patients with a known history of an impacted tracheal or esophageal foreign body, dental prostheses accounted for 11.5% of the cases.
Patients can present with vague symptoms of neck pain, dysphagia, odynophagia, and excessive salivation. The clinical history may be vague, and patients may not report a definite history of swallowing their dentures secondary to trauma, intoxication, or loss of consciousness. The diagnosis is further complicated by the fact that polymethylmethacrylate (PMMA), the resin base used for construction of partial dentures, is radiolucent. Even the porcelain and plastic artificial teeth are difficult to visualize on plain radiographs. Although attempts have been made to create a radiopaque resin base, they have not been able to match the physical and esthetic qualities of PMMA.5–8 Complete dentures as well as some temporary partial dentures do not have a metallic-based reinforcement, unlike implant-supported full dentures and permanent removable partial dentures, which have a metallic base for reinforcement and retention. Some temporary partial dentures (ie, stayplates or flippers) may have clasps, which are metal based for improved retention. If the patient has cosmetic concerns and does not want the clasps to be visible and retention is adequate, then a metallic component may not be present, as was the case in our patient.9
The delay in diagnosis can result in significant morbidity. If undetected, retained foreign bodies can lead to significant edema that causes obstruction or perforation, or both. Multiple case reports have documented the development of tracheoesophageal, aortoesophageal, and even esophago-broncho-aortic fistulas.10–13 In addition, there have been reports of aortic erosion as well as complications distally in the gastrointestinal tract, such as enterocolonic fistulas and colonic perforation.13–14 In a cross-sectional study of 103 patients with foreign-body ingestion, Khan et al15 reported that complications were more common in adults (37.1%) compared with children (8.8%) and that the most severe complications occurred with ingested dentures.
In the absence of radiologic findings, management should be based on history and clinical symptoms. In a patient with dysphagia and odynophagia or new-onset neck pain, a referral to an ENT physician should be considered.16 Direct visualization with flexible or rigid endoscopy should be performed. Knowledge of the subtle imaging findings of these partial dentures and interpretation of these studies with sufficient clinical history may lead to earlier diagnosis and treatment.
Footnotes
Paper presented previously at: Annual Meeting of the American Society of Head and Neck Radiology, September 28, 2006; Phoenix, Ariz.
References
- Received February 4, 2007.
- Accepted after revision April 3, 2007.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}