
Abstract
BACKGROUND AND PURPOSE: Hypoattenuated foci in the otic capsule are routinely identified on multidetector CT (MDCT), particularly in pediatric patients. We aimed to describe and characterize the hypoattenuated focus in the anterior otic capsule.
MATERIALS AND METHODS: We first reviewed histologic sections of the temporal bone from 8-month-old fetuses to determine the nature of the hypoattenuated focus in the anterior otic capsule. A cadaver collection of skull bases from fetuses and neonates (n = 19), infants (n = 24), and young children (n = 23) were then studied with MDCT to determine the developmental evolution of this hypoattenuated focus in relation to the petrous apex. We specifically looked for the hypoattenuated focus in the anterior otic capsule, the development of the petrous apex, and the presence of other hypoattenuated foci in the fissula ante fenestram and middle otic layer.
RESULTS: The hypoattenuated focus in the anterior otic capsule corresponded histologically to a cancellous bone trabecula emanating from the middle otic layer and directed toward the petro-occipital fissure. At this level it was covered with a cartilaginous cap. The hypoattenuated focus was observed in all of the fetuses and in all of the postnatal subjects younger than 4 months of age and was always associated with hypoattenuated foci of the middle otic layer and the fissula ante fenestram. This hypoattenuated focus became less obvious as the petrous apex developed.
CONCLUSION: The hypoattenuated focus in the anterior otic capsule should be recognized as a normal variant in pediatrics. It could represent a relic from the development of the petrous apex.
The otic capsule has unique embryologic development displaying growth features found nowhere else in the skeleton. It develops around the membranous labyrinth from a cartilaginous anlage and progressively ossifies, ultimately forming 3 different layers: the thin inner endosteal layer, the middle layer, and the outer periosteal layer. The middle layer contains both enchondral and intrachondrial bone forming elements, the so-called osseous globules.1,2
Pericochlear hypoattenuated foci in the middle layer of the otic capsule are routinely observed with thin-section CT in asymptomatic patients where they can mimic pathologic conditions.3,4 It has been speculated that these foci correspond to cartilage remnants, fibrocartilage, nonmineralized bone, or bone marrow, but this still remains debated. Moreover, in pediatric patients, these hypoattenuated foci have been mostly depicted in the area of the fissula ante fenestram,5,6 whereas less attention has been paid to other locations, such as the anterior otic capsule.
We observed the occasional presence of a hypoattenuated focus in the anterior otic capsule in young patients (Figs 1 and 2). Although these findings were thought to correspond to a normal variant, this particular location has never been described thus far. This study aimed to further characterize this hypoattenuated focus and to determine its evolution over time.

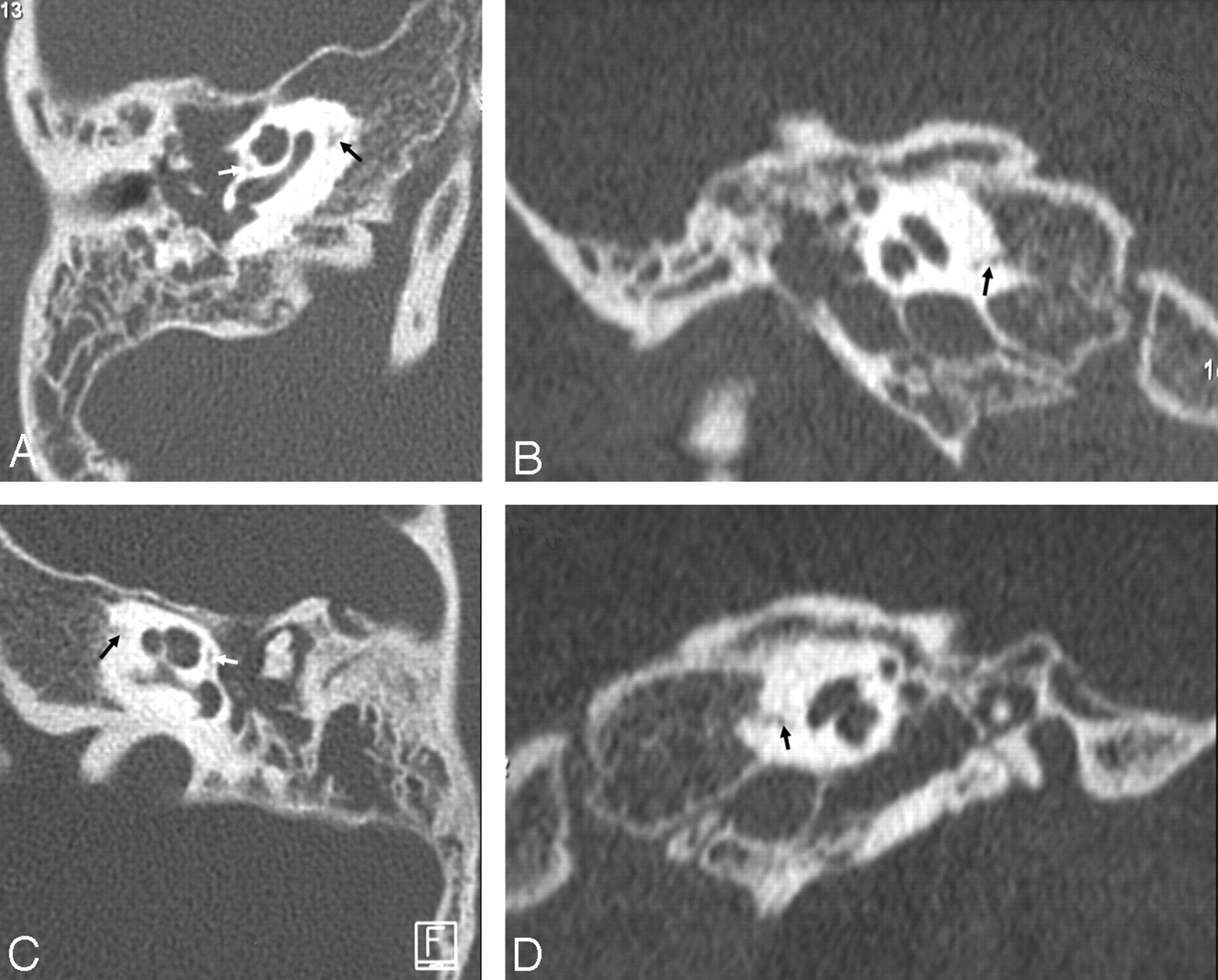
Six-year-old girl with complicated bilateral acute otitis media. Transverse (A) and coronal (B) MDCT sections of the right temporal bone. Transverse (C) and coronal (D) MDCT sections of the left temporal bone. A well-defined hypoattenuated area (black arrow) is seen in the anterior aspect of the otic capsule on both sides. The hypoattenuated focus of the fissula ante fenestram (white arrow) is also apparent.

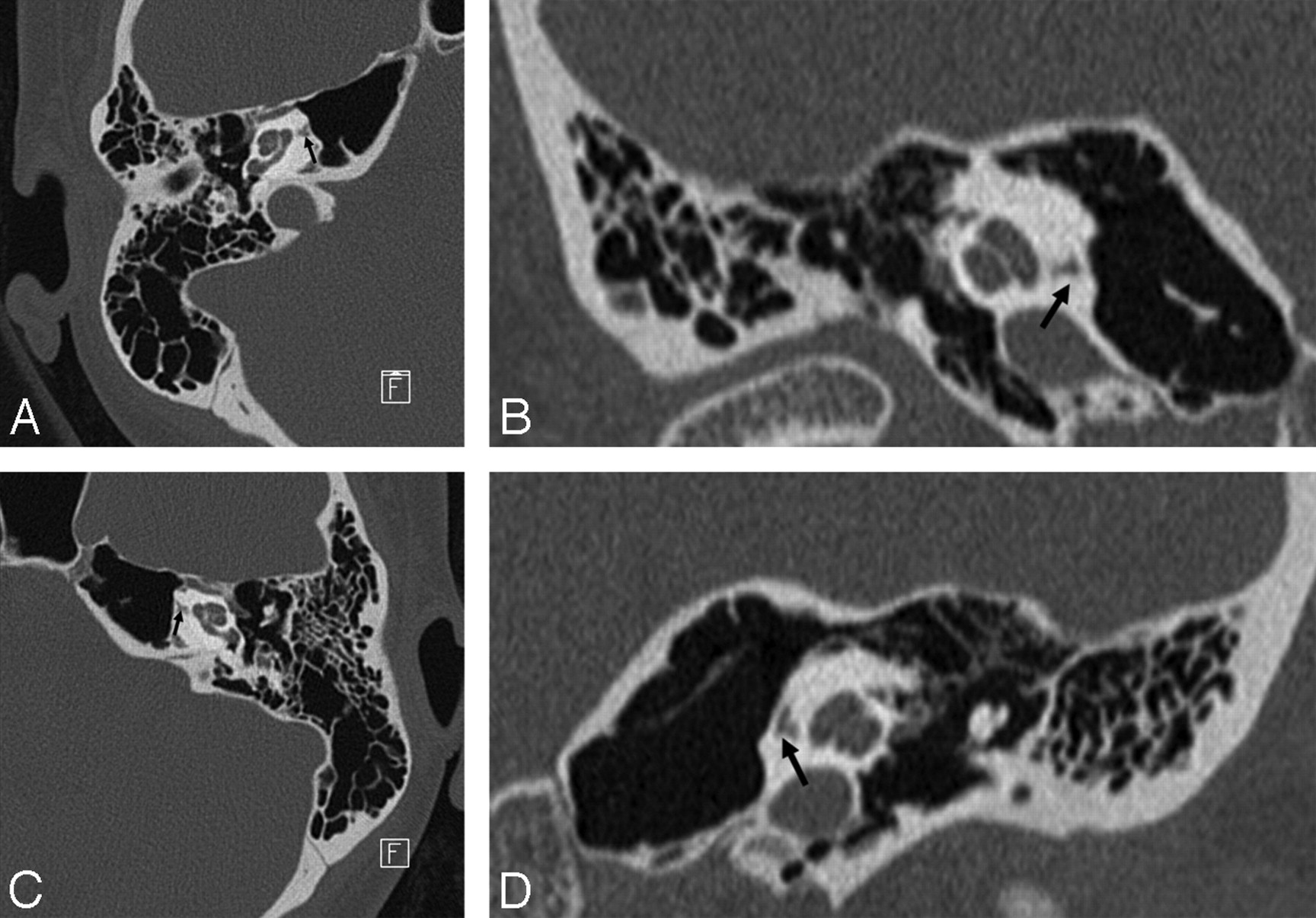
Thirty-four-year-old woman with dizziness. Transverse (A) and coronal (B) MDCT sections of the right temporal bone. Transverse (C) and coronal (D) MDCT sections of the left temporal bone. Bilateral hypoattenuated foci (black arrow) in the anterior otic capsules are particularly well underlined by complete pneumatization of the petrous apex. Otosclerosis was ruled out by other investigations, and these findings were considered as normal variants.
Materials and Methods
Our study encompassed 2 phases. In the first phase, we reviewed histologic sections of skull base from fetuses to determine the nature of the hypoattenuated focus. In the second phase, we imaged a collection of skull bases of different ages with MDCT to determine the evolution of this particular area over time.
Histologic Sections
We examined histologic sections of the head and neck from 3 8-month-old fetuses. This material resulted from a previous study, the details of which have been published.7 Transverse, coronal, and sagittal sections of the temporal bone were carefully reviewed with particular focus on the anterior otic capsule area to establish a correlation with multidetector CT (MDCT) images.
Anatomic Specimens
Anatomic specimens were taken from an anatomic collection of skulls obtained from donors between 1891 and 1902 and used in accordance with our local ethical regulations. Specimens with any deformity were excluded, and ages were available in each case. Our population consisted of 66 subjects including 19 fetuses and neonates (age range, 4–9 months from conception; mean age, 7.7 months), 24 infants (age range, 1–11 months from birth; mean age, 5 months), and 23 young children (age range, 12–72 months from birth; mean age, 24 months).
MDCT Imaging
Skull bases were imaged with a 16 detector row MDCT Somaris (Siemens, Erlangen, Germany) using our routine high-resolution protocol. Acquisition parameters were 140 kV, 400 mAs, and 0.6-mm beam collimation. Reconstruction parameters were 0.6-mm section thickness with a 0.3-mm increment, 15-cm FOV, and a high-resolution kernel. Reformations in a plane parallel to the lateral semicircular canal and in sagittal and coronal planes were obtained.
Image Analysis
Images were simultaneously reviewed by 2 experienced radiologists. In each case, the anterior otic capsule was analyzed to determine the presence of hypodensities in the middle layer or adjacent petrous apex. In addition, the development of the petrous apex and the presence of a hypoattenuated area at the fissula ante fenestram were assessed. All of the findings were recorded by consensus.
Results
Histologic Correlations
Histologic sections exquisitely demonstrated the unique architecture of the otic capsule and its organization into 3 layers (Fig 3). A particular finding in its medial aspect consisted of a focal interruption of the outer layer and a protrusion of the middle layer. This protrusion consisted of trabecular bone morphologically identical to the remaining of the middle otic layer except that it imperceptibly merged with a cartilaginous cap in its more medial aspect adjacent to the petro-occipital fissure. This cartilaginous cap was distinct from the fibrous structure of the petro-occipital fissure. This particular anatomic pattern was found to precisely match our sporadic imaging findings in terms of location and structure.

Photomicrograph of a parasagittal section of the head from an 8-month-old fetus. A, General view. Compared with other structures of the skull base, the otic capsule (frame) appears surprisingly large as it has already attained its adult size. Bony landmarks are F, frontal; Mx, maxillary; Md, mandible; S, sphenoid; C, clavicle; P, petrous; O, occipital; A, atlas. B, Close-up view of the otic capsule. The different layers (o indicates outer; m, middle; i, inner) of the otic capsule are well demonstrated around the basal turn of the cochlea (cbt). A focal dehiscence of the outer layer with protrusion of the middle layer is clearly seen (arrows). The protrusion of the middle layer is directed toward the petro-occipital fissure (pof) and imperceptibly merges with a cartilaginous cap (c) that is distinct from the fibrous tissue occupying the petro-occipital fissure.
Imaging Findings
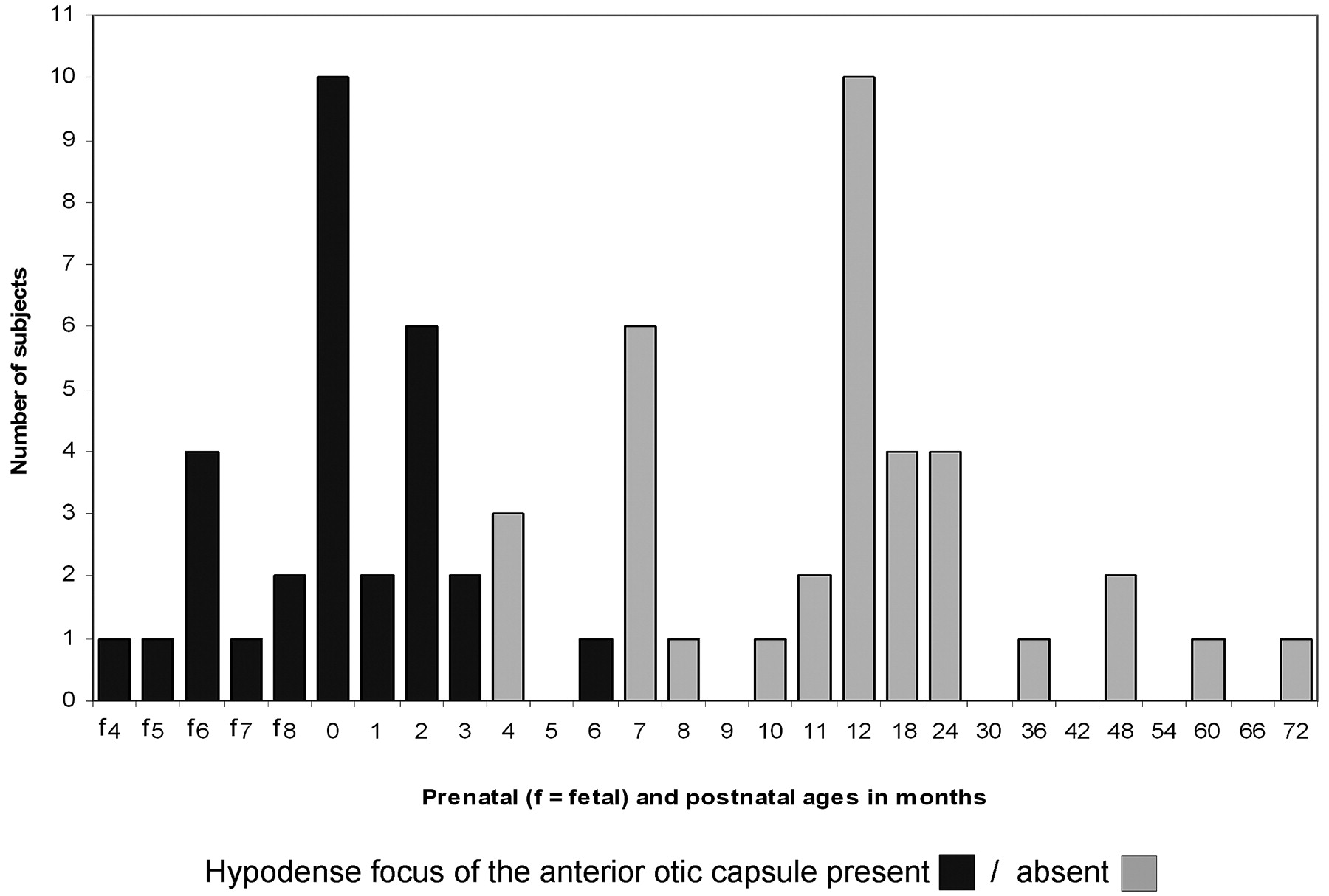
MDCT images of skull bases from anatomic specimens also demonstrated a hypoattenuated area located in the anterior otic capsule. This pattern was observed in fetuses and neonates, as well as in all of the infants before the age of 4 months. It was not found in older specimens except in 1 6-month-old infant. When present, the hypoattenuated focus was seen connecting the middle otic layer to the petro-occipital fissure (Fig 4). In the earliest stages with nondeveloped petrous apex, the hypoattenuated focus was relatively short and broadly communicated with the petro-occipital fissure (Fig 5). In subsequent stages, the hypoattenuated area appeared elongated and thinned after the growth of the petrous apex (Fig 6). The hypoattenuated focus in the anterior otic capsule was constantly associated with other hypoattenuated foci in the middle otic layer and fissula ante fenestram. Imaging findings in terms of presence or absence of the hypoattenuated focus in the anterior otic capsule are summarized in Fig 7.

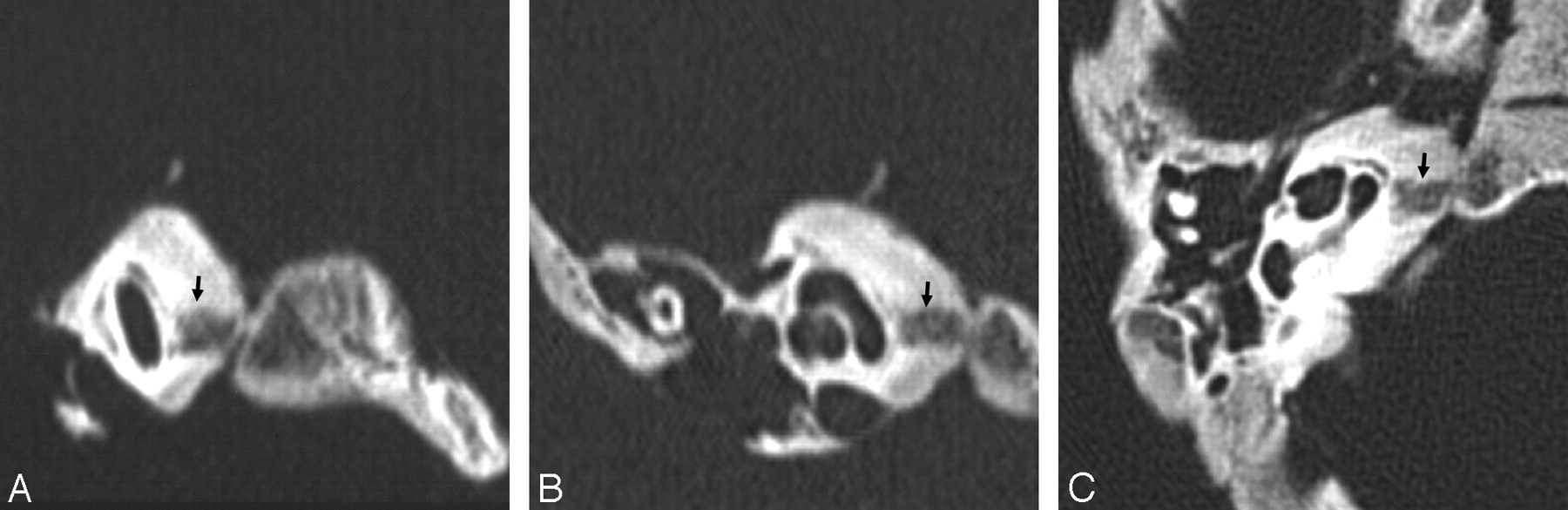
Sagittal oblique (A), coronal (B), and transverse (C) MDCT sections from a neonate specimen. The middle otic layer is seen as a smooth hypoattenuation around the cochlea, circumscribed by the attenuated inner and outer layers. A well-defined hypoattenuated focus (arrow) is seen in the anterior otic capsule, communicating laterally with the middle layer and medially with the petro-occipital fissure.

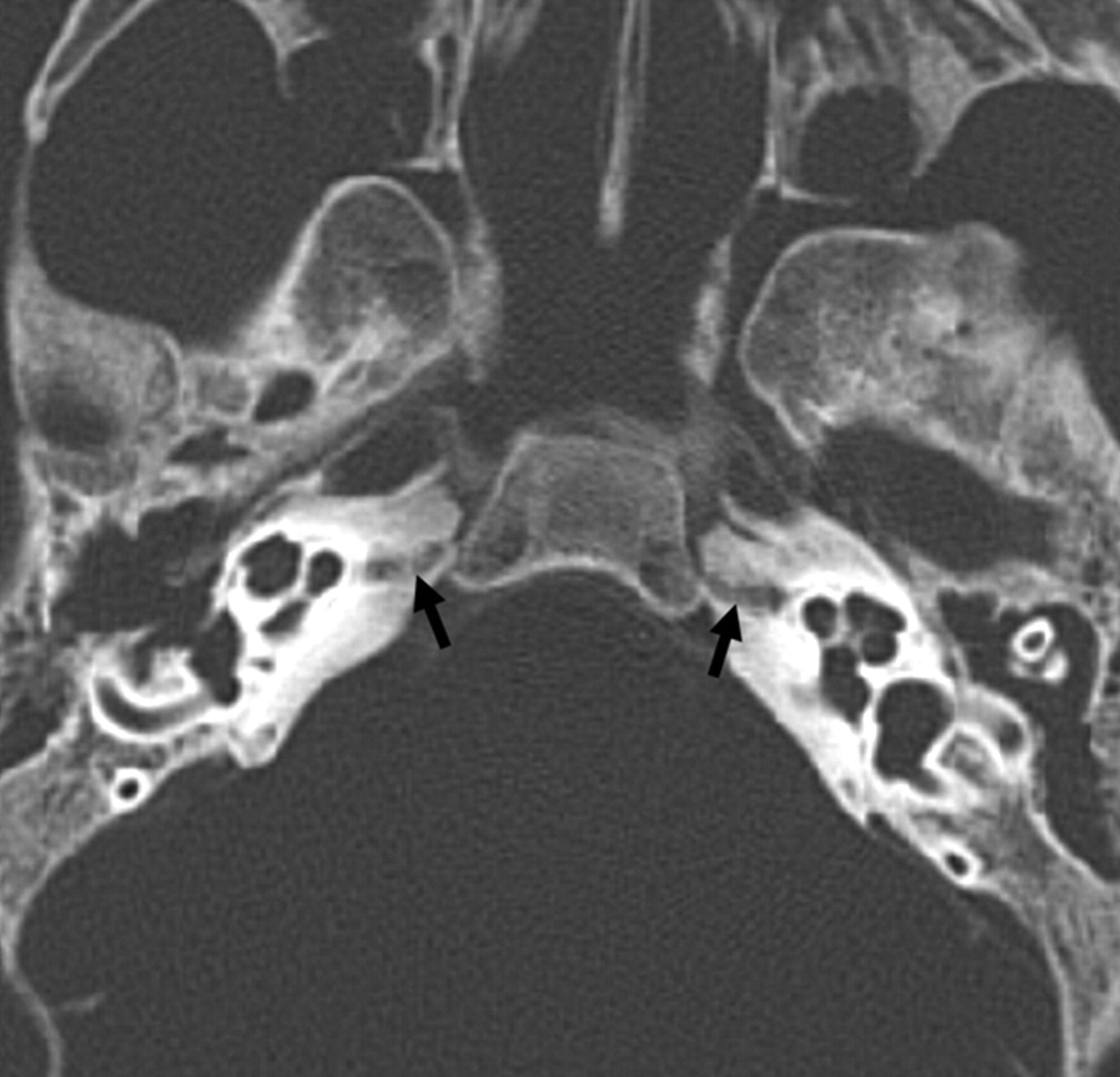
Transverse MDCT section from a 4-month-old fetal specimen. The middle otic layer is seen as a smooth hypoattenuation surrounding the cochlea, circumscribed by the attenuated inner and outer layers. The dehiscence of the outer layer of the otic capsule (arrows) allows broad communication between the middle layer and the petro-occipital fissure. The petrous apex is not yet developed.

Transverse MDCT image from a 2-month-old infant specimen. The middle otic layer persists, though tinier than in previous stages. The hypoattenuated focus (arrow) is well demonstrated, spanning the petrous apex, which is now developed and reaching the petro-occipital fissure through a focal cortical interruption.

Summary of findings in anatomic specimens.
Discussion
Using anatomic specimens, we characterized the hypoattenuated focus in the anterior otic capsule and determined its evolution through the earliest months of life. The otic capsule surrounding the membranous labyrinth develops from a cartilaginous anlage. However, in contrast to the typical pattern observed in long bones, this cartilaginous anlage grows extraordinarily rapidly to attain adult dimensions at the fifth month of fetal life. It is only after completion of the growth process that ossification begins from 14 centers. Each center consists of 3 layers: the inner endosteal, the middle, and the outer periosteal. The cartilage of the middle layer is progressively invaded by vascular buds and replaced by bone resulting in enchondral ossification. Cartilage also partially persists in the middle layer as islands where intrachondrial bone is formed. The ossification process begins around the cochlea and the vestibule and ends in the vicinity of the semicircular canals. Fusion is observed from the 19th week, and the bony capsule is completed by the 23rd week. Ossification of the middle layer is not complete until birth, though cartilage islands may persist much longer.1,2
Hypoattenuated foci in the otic capsule are routinely depicted with high-resolution CT of the temporal bone in children and have been attributed to either incompletely mineralized bone or cartilage. Controversy exists in radiologic literature concerning this terminology, because only a few studies have established direct correlation between histology and imaging of the otic capsule. In their previous work, Sick and Veillon7 demonstrated normal presence of fibrocartilage in the area of the fissula ante fenestram, whereas the middle otic layer mainly consisted of cancellous bone. In our study, we observed that the hypoattenuated focus in the anterior otic capsule mostly corresponded with cancellous bone protruding from the middle otic layer and included a cartilaginous cap in its medial aspect adjacent to the petro-occipital fissure. This cartilaginous cap was clearly distinct from the fibrocartilaginous material present in the petro-occipital fissure. In reference to the classic description, the hypoattenuated focus of the anterior otic capsule approximately corresponded with the first ossification center.2 The hypoattenuated focus was also found to span the petrous apex and to elongate progressively during its growth. We were unable to find precise information about the specific process and ossification centers involved in the growth of the petrous apex. However, the particular location of this hypoattenuated focus, its sequential modifications, and the presence of a cartilaginous cap in its medial aspect suggest that it could be involved in the growth process of the petrous apex. The hypoattenuated focus incidentally observed in children and young adults was restricted to the immediate vicinity of the middle otic layer and could, therefore, represent a remnant from the development of the petrous apex.
The fissula ante fenestram is probably the most common hypoattenuated focus of the otic capsule. It was observed in 23 (32%) of 73 patients aged 0–9 years by Pekkola et al6 and in 41% of 200 subjects aged 0–19 years by Chadwell et al.5 It was also observed in all of our cases. On the other hand, the hypoattenuated focus in the anterior otic capsule was mostly seen at an earlier stage of development. The hypoattenuated focus in the anterior otic capsule represents a normal pattern of growth and should not be mistaken for a pathologic condition. For forensic and anthropologic purposes, the recognition of this pattern of growth, as a constant finding before the age of 4 months, may constitute an ancillary method to determine the age of subjects by using the temporal bone. For example, it may be used in conjunction with other methods, such as the measurement of the fossa subarcuata diameter.8
Hypoattenuated foci of the otic capsule are supposed to contain cartilaginous remnants sometimes involved in the pathogenesis of otosclerosis. It has been suggested that type II collagen present in these cartilaginous remnants is the target for an autoimmune reaction leading to bone resorption.9,10 Otosclerotic foci have been extensively depicted with CT in these areas where cartilaginous remnants are commonly found, namely the fissula ante fenestram and the middle otic layer.4,11 Therefore, it would be interesting to consider the hypoattenuated focus in the anterior otic capsule as a potential site of otosclerosis and to determine its role in the development of anterior pericochlear otosclerosis.
In summary, the hypoattenuated focus in the anterior otic capsule should be regarded as a normal variant that may reflect the growth process of the petrous apex. However, it is commonly observed only in infants before the age of 4 months. In older subjects, concern for a pathologic condition (otosclerosis) must be kept in mind.
Acknowledgments
We thank the Strasbourg Anatomical Institute (Director Prof. J.-L. Kahn) for providing the anatomic material.
References
- Received December 26, 2006.
- Accepted after revision May 24, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Internal Auditory Canal Diverticula among Pediatric Patients: Prevalence and Assessment for Hearing Loss and Anatomic Associations
- Incomplete Endochondral Ossification of the Otic Capsule, A Variation in Children: Evaluation of Its Prevalence and Extent in Children with and without Sensorineural Hearing Loss