
Abstract
SUMMARY: We report the CT and MR imaging findings in a patient with malignant peripheral nerve sheath tumor in the right nasolabial area, which exhibited typical imaging features of cystic adenoid carcinoma.
We present a rare case of a patient without neurofibromatosis type 1 (NF-1) and with a malignant peripheral nerve sheath tumor (MPNST) arising in the terminal branches of the maxillary nerve in the right nasolabial area with retrograde perineural invasion of the entire nerve all the way to the pterygopalatine fossa. The location, behavior, and imaging features of our patient prompted the radiologic diagnosis of cystic adenoid carcinoma; however, pathologic analysis of the lesion confirmed the diagnosis of MPNST. To our knowledge, there is no previous imaging report of a lesion of this nature with this location and behavior.
Case Report
We present the case of a 62-year-old man with a previous history of facial trauma who complained of nose pain and nocturnal breathing problems. Findings of the clinical examination were completely normal. Several months later, the patient came back to our center because pain and breathing problems had increased and he could not continue his normal activities. In the new clinical examination, a soft-tissue mass was observed swelling on the right nasolabial fold and on the vestibule of the mouth, with no associated mucosal lesion; therefore, a submucosal lesion was suggested. CT and MR imaging revealed the presence of a homogeneous enhancing solid mass in the right nasolabial area (Fig 1A, -B), apparently located in the labial submucosa (Fig 1A), which invaded the right maxillary nerve all the way to the pterygopalatine fossa (Fig 1A, -B). The maxillary nerve was enlarged (Fig 2), with a homogeneous tubular-shaped increase of its diameter (Figs 3A and 1A, -B), resulting in a remodelling of the infraorbital canal (Fig 3B). A cystic adenoid carcinoma was suggested on the basis of the imaging and clinical findings. The patient underwent surgery, and the pathologic examination, surprisingly, was consistent with MPNST. Neither family history nor stigmata of NF-1 was found in the patient.

A, Curved saggital reconstruction image of a contrast-enhanced CT scan shows a submucose mass in the nasolabial area (straight arrow) with enlargement of the Vb nerve (curved arrow) all the way to the pterygopalatine fossa. Short arrows indicate buccal mucosa, and the asterisk indicates the pterygopalatine fossa. B, Contrast-enhanced oblique saggital fat-suppressed T1-weighted MR image shows an enhancing mass (straight arrow) in the nasolabial area with perineural spread through maxillary nerve (curved arrow).

Coronal reconstruction contrast-enhanced CT scan demonstrates enlargement of the right maxillary nerve (arrow).

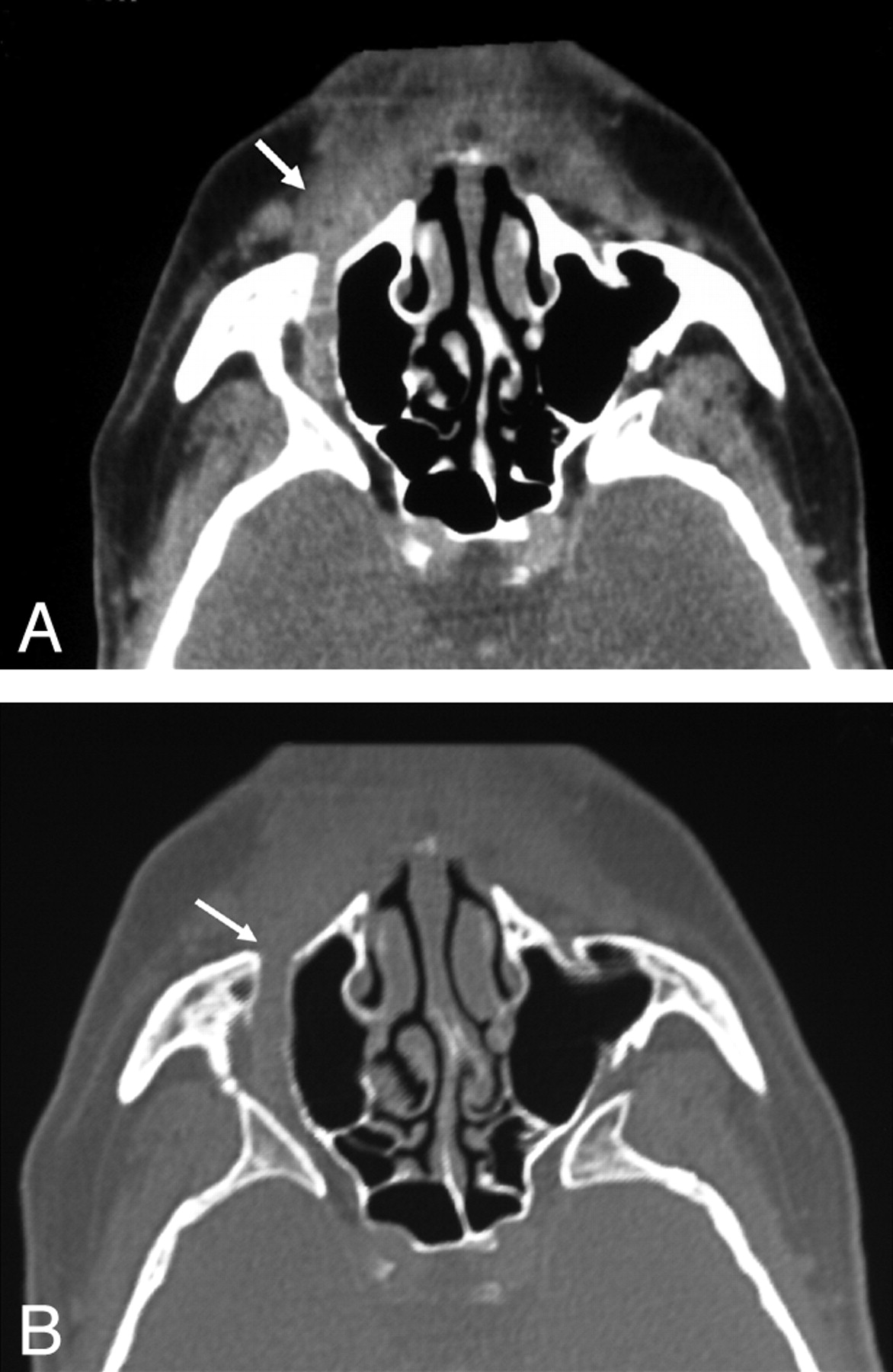
A, Curved axial reconstruction of a contrast-enhanced CT scan shows the original mass in the right nasolabial (arrow) area followed by a tubular-shaped enlargement of the maxillary nerve. B, Same image as in A with bone windowing. Note the infraorbital canal enlargement (arrow).
Discussion
MPNSTs are rare lesions derived from the mesenchymal cells of the neural crest. The term “MPNST” is now preferred instead of terms like “neurofibrosarcoma,” “neurogenic sarcoma,” or “malignant schwannoma” because the originating cell is not clearly understood.1 MPNSTs represent approximately 6% of all malignant soft-tissue tumors.2,3 These lesions have a tendency to affect the trunk and extremities, and only 10% of all MPNSTs are located in the head and neck region.2 The most common nerve affected is the sciatic nerve, followed by the brachial plexus.2 Between 38%–50%3,4 of these malignant tumors are associated with NF-1, and this entity is also related to multiplicity.3,4 The risk for developing an MPNST is 4600 times greater in patients with NF-1 than in the general population.4
The typical histologic features of these tumors are a monomorphic population of spindle cells arranged in fascicles, which usually demonstrate focal S-100 protein positivity, though 30% may be negative.3 They may show reactivity for Leu-7 or myelin basic protein, but they are negative for cytokeratins. Occasionally, they are positive for the melanocytic marker HMB-45.3
These lesions grow inside the nerve sheath, adopting a spindle or globular appearance,4 and though most of them present recognizable nerve roots entering and exiting the lesions, it is common to find intraneural invasion through the nerve bundles.2 The optimal treatment is combined surgical excision with radiation therapy.3 Radiation therapy is indicated because of the high recurrence rate of the tumor.3 Overall survival and disease-free survival are influenced by the patient's age (there is a better prognosis in patients >30 years old), tumor location, tumor size (patients with tumors <10 cm in diameter fared better than those with large tumors), and the quality of margins.5
Perineural spread involves the dissemination of a tumor through the planes of the neural sheath or along lymphatics of the epineurium and perineurium toward noncontiguous regions.6 It also carries a higher recurrence rate and a subsequent worse prognosis.6,7
The facial nerve and the second (V2) and third (V3) divisions of the trigeminal nerve are the most commonly affected nerves, with perineural invasion in the head and neck region, and perineural invasion usually occurs in a centripetal fashion, though centrifugal involvement has also been described.7 In head and neck tumors, perineural infiltration is a typical manifestation of adenoid cystic carcinoma,8 though it is most commonly found in squamous cell carcinoma because of its higher prevalence.9 Non-Hodgkin lymphomas and other sarcomas may also show this perineural invasion behavior.9 Both MR and CT imaging are capable of detecting perineural invasion, though medical literature has classically considered MR imaging as the technique of choice.7,9 The imaging findings of perineural spread depend on the head and neck area affected but usually include foraminal enlargement or destruction, obliteration of fat planes, nerve enlargement, nerve enhancement, replacement of the trigeminal subarachnoid cistern with soft tissue, convexity of the lateral dural margin of the cavernous sinus, etc.6
In our patient, the tumor arose from the terminal sensitive branches of the right infraorbital nerve in the nasolabial area and centripetally invaded this nerve all the way to the pterygoid fossa. The nerve infiltration resulted in a nerve enlargement and a homogeneous tubular-shaped increase of the nerve diameter, but not in the typical spindle shape of MPNST. Multidetector CT allowed curved reconstructions that were very illustrative of the particularly perineural invasion exhibited by the tumor. However, MR imaging is necessary in this type of lesion because CT is a limited tool for demonstrating intracranial extension to the cavernous sinus, Meckel cave, and the cisternal and pontine portions of the cranial nerve V.
The differential diagnoses in the presence of a swelling mass in the nasolabial fold involve nasolabial cyst, odontogenic inflammatory process, odontogenic tumor, squamous cell carcinoma, soft-tissue sarcoma, bone lesion, lymphoproliferative disorder, and salivary gland tumor.10 On the basis of the location, solid nature, and enhancing pattern of the lesion after intravenous contrast administration and the perineural invasion exhibited, the differential diagnosis was narrowed to solid malignant tumors. Given the absence of an associated mucosal lesion, cystic adenoid carcinoma was suggested as the first diagnostic possibility.
Conclusion
To our knowledge, there has been no previous case reported in the literature of an MPNST in this location showing this particular behavior and imaging features because it is usually seen in cystic adenoid and squamous cell carcinoma, but not in MPNSTs.
References
- Received September 7, 2007.
- Accepted after revision September 23, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.