
Abstract
BACKGROUND AND PURPOSE: The CT appearance of the anterior skull base has been investigated but with limited attention directed to the olfactory recess. As defined by opacity abutting the undersurface of the cribriform plate, the prevalence of olfactory recess opacity (ORO) on sinus CT was examined to clarify whether this should raise suspicion for an unsuspected pathologic process.
MATERIALS AND METHODS: Outpatient sinus CTs were evaluated for ORO in 500 consecutive patients (mean age, 46.9 years; 52.6% women). On a per-side basis (n = 1000), the presence of surgical changes, inflammatory sinus disease, and concha bullosa was determined by 2 neuroradiologists. Logistic regression was used to examine the association of ORO with these variables.
RESULTS: ORO was identified in 59 (11.8%) patients, bilateral in 27 (5.4%), and unilateral in 32 (6.4%). There were 343 of 1000 ethmoid sides that were diseased, and 66 (27.2%) showed ipsilateral ORO. In contrast, only 20 (3.0%) of 657 clear ethmoid sides showed ORO (P < .0001). ORO was significantly (P = .013) more common with previous surgery (18/75; 24.0%) than without (68/925; 7.4%). Ipsilateral concha bullosa was not associated with ORO. Of 32 patients with unilateral ORO, 5 (15.6%) had no ethmoid opacification or previous surgery, and 1 of these patients had an encephalocele causing the ORO. Finally, unilateral ORO was present in only 1 of 122 patients with completely clear sinuses (the encephalocele that was just mentioned).
CONCLUSION: ORO is distinctly uncommon without sinonasal inflammation or previous surgery. Isolated unilateral ORO raises suspicion for an underlying neoplasm or cephalocele and warrants further evaluation.
The olfactory recess is located between the nasal septum and the insertion of the vertical portion of the middle turbinate on the anterior skull base. There is a limited body of CT literature dedicated to the anatomy of the olfactory recess, with more extensive studies addressing the variations of adjacent structures such as the cribriform plate and fovea ethmoidalis. These studies have focused primarily on the effect of olfactory recess anatomy on the sense of smell1,2 and how anatomic variations might pertain to preoperative planning.3–9 No studies to date have addressed variation in the olfactory recess regarding identification of the circumstances in which it is likely to become opacified.
In recent years, we have encountered 2 cases of very subtle esthesioneuroblastoma in which paranasal sinus CT only demonstrated a small amount of focal opacity in the olfactory recess. This prompted our study to determine the prevalence of olfactory recess opacity (ORO) on outpatient CT scans of the paranasal sinuses to determine when this should heighten concern for a pathologic condition such as a small neoplasm or cephalocele.
Materials and Methods
The Committee on Human Subjects Research at our institution approved this study. The radiology information system was used to identify 500 consecutive outpatients age 18 years or older who had undergone routine sinus CT between January 1, 2000, and February 1, 2001, on the same CT scanner (Lightspeed; GE Healthcare; Milwaukee, Wis). To be included for review, the CT had to be acquired as contiguous direct coronal 3-mm images from the tip of the nose through the sella with the patient in the prone position. Sinus CT scans obtained in the axial plane with coronal reconstructions were specifically excluded to allow for consistency. No scans had to be excluded on the basis of technical inadequacy.
Each CT was reviewed on a commercially available PACS system (AGFA, Greenville, SC) in both bone (W/L = 3000/600) and soft tissue (W/L = 400/40) window settings by the same 2 neuroradiologists (J.M.H., C.M.G.) in consensus. ORO was said to be present when opacity was identified in the olfactory recess that was in direct contact with the cribriform plate. In addition, the paranasal sinuses were evaluated on a per-side basis (n = 1000) for the presence of the following features: concha bullosa (pneumatization extending into the bulbous portion of the middle turbinate), infectious or inflammatory changes (polyps, mucosal or mucoperiosteal thickening, air fluid levels, mucus retention cysts), cribriform plate integrity, and postsurgical anatomy (ethmoidectomy or middle turbinectomy, or both). A normally pneumatized sinus lacking such features was considered to be clear.
We assessed predictors of the primary outcome (the presence or absence of ORO) using SPSS 15.0 statistical software (SPSS, Chicago, Ill). We specifically created a binary logistic regression model using a forward model selection method that incorporated the explanatory variables of ipsilateral ethmoid disease, previous surgery, and concha bullosa. Interaction terms were evaluated as part of model selection to allow for interdependence of these explanatory variables. Inclusion in the model required the P value for the Wald χ2 statistic to be less than .05.
Results
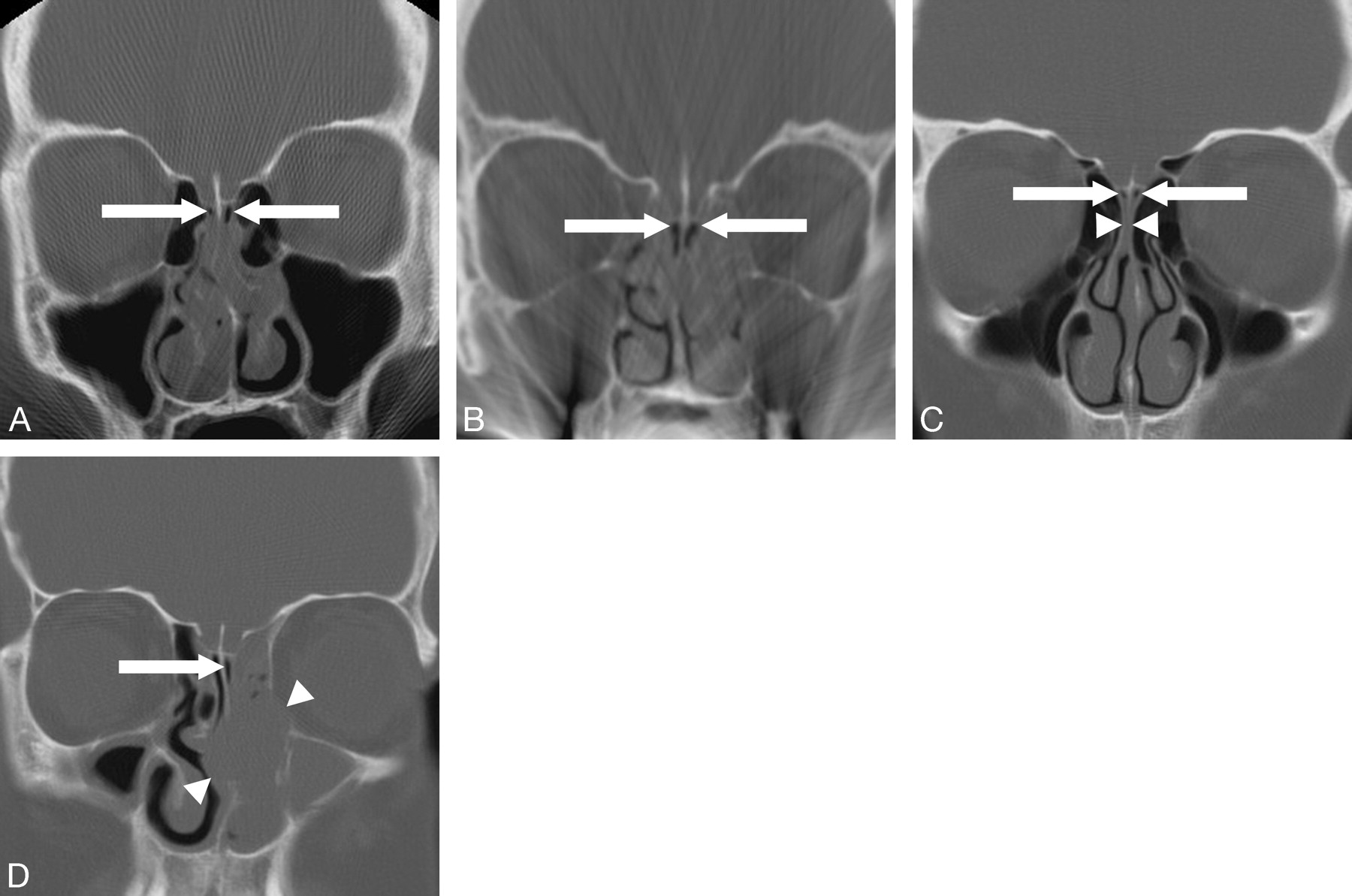
The study population consisted of 237 (47.4%) men and 263 (52.6%) women with a mean age of 46.9 years (range, 18–89 years). ORO was identified bilaterally in 27 (5.4%) patients and unilaterally in 32 (6.4%) patients, with an equal distribution between left and right. In many cases, the olfactory recess was noted to be clear even in the context of diffuse sinonasal mucosal thickening (Fig 1A), pansinus opacification (Fig 1B), narrowing related to prominent adjacent ethmoidal air cells (Fig 1C), or focal pathologic process such as an adjacent large polyp (Fig 1D).

A, Coronal sinus CT examination performed on a 27-year-old woman with symptoms of chronic sinusitis demonstrates prominent sinonasal mucosal thickening but preserved aeration of the olfactory recesses (arrows). B, A 65-year-old woman with chronic sinusitis underwent coronal sinus CT examination, which demonstrates continued pneumatization of the olfactory recesses adjacent to the cribriform plates (arrows) despite extensive pansinus opacification. C, A 32-year-old woman with headaches was evaluated with coronal sinus CT scan, which demonstrates olfactory recess narrowing (arrowheads) because of prominent adjacent ethmoid air cells, but no opacity is present adjacent to the cribriform plates (arrows). D, Coronal sinus CT scan performed on a 41-year-old man with a known left nasal polyp exhibits a rounded soft tissue structure centered in the middle meatus (arrowheads) with surrounding osseous remodeling. Despite extensive resultant maxillary and ethmoidal opacification, the apex of the olfactory recess is patent (arrow).
Of the 1000 interrogated sides, 343 showed evidence of inflammatory disease involving the ethmoidal sinuses, and 66 (27.2%) of these sides had associated ipsilateral ORO. In contrast, only 20 of 657 sides with normally aerated ethmoid sinuses (3.0%) were positive for ORO (P < .0001). The association between ORO and previous surgery was also found to be statistically significant (P = .013). Specifically, of the 75 olfactory recesses with evidence of previous ipsilateral sinonasal surgery, 18 (24.0%) exhibited ORO, compared with 68 (7.4%) of 925 of those without surgical changes showing ORO. A total of 96 conchae bullosa were identified. Of these, only 5 (5.2%) had ipsilateral ORO. This was not a significant association because 81 (9.0%) of 904 sides without concha bullosa showed ORO. Finally, the inclusion of interaction terms to account for explanatory variable interdependence did not meet significance levels, and these terms were not incorporated into the final logistic regression model as a result.
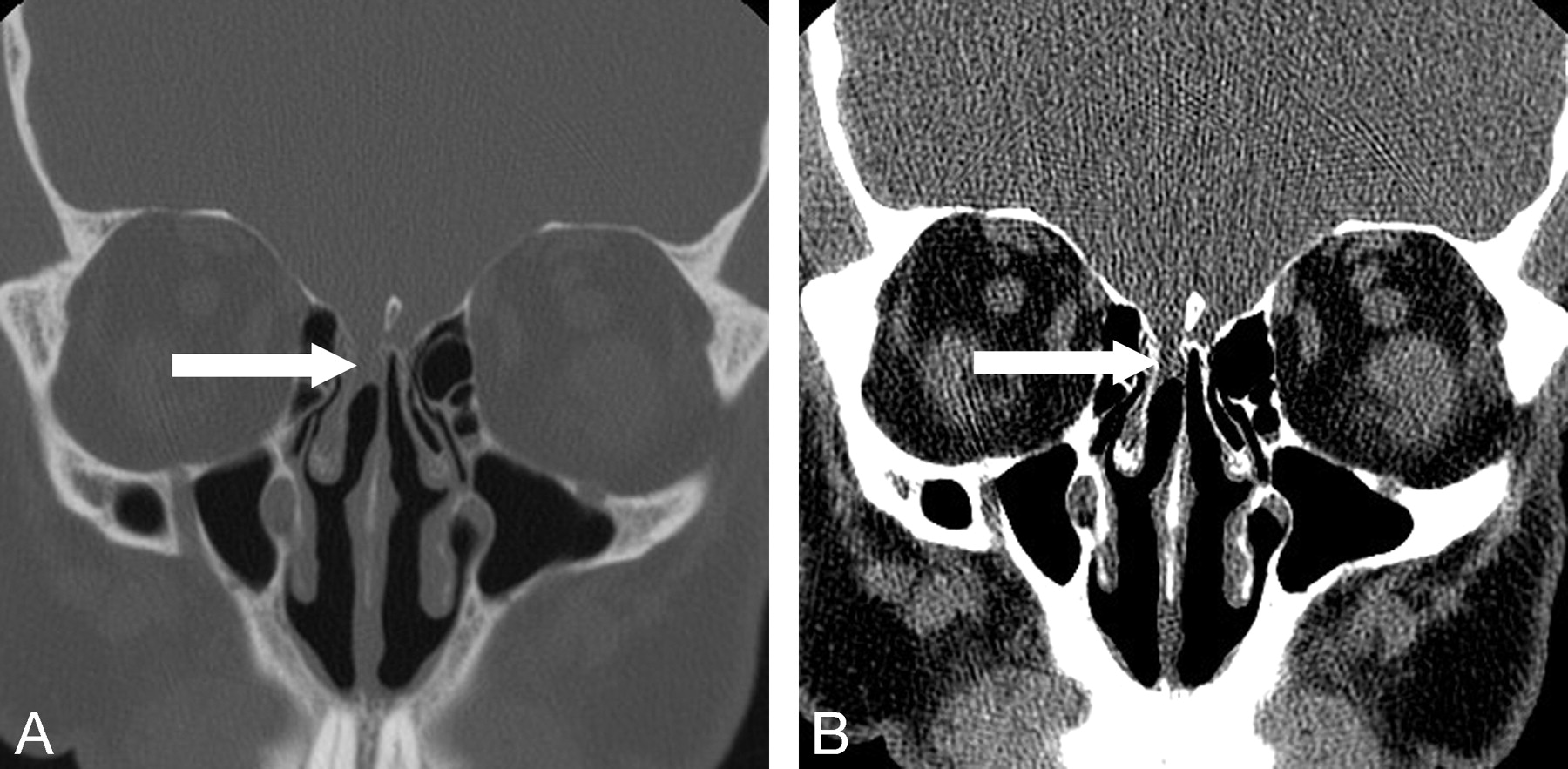
Thirty-two patients demonstrated unilateral ORO, which might be considered most suspicious for an unsuspected pathologic condition such as neoplasm or cephalocele. Of these, only 5 (15.6%) of them had no evidence of either previous surgery or ethmoidal sinus disease. One of these 5 patients had an encephalocele accounting for the ORO, which was subsequently confirmed on surgical treatment (Figs 2A, -B). A second patient had unilateral ORO with a focal defect in the cribriform plate, which was suggestive of a cephalocele (not shown), but the patient was lost to follow-up. Of the remaining 3 patients with indeterminate findings (ie, no visible defect in the cribriform plate), 1 received no additional follow-up and the remaining 2 had persistent unilateral ORO on follow-up CT scans at 19 and 75 months, respectively, without progressive enlargement of the abnormality. Assuming that the ORO in these latter 4 patients in whom there was no confirmation was inconsequential, this still translates into 20% of patients with unilateral ORO in the absence of ethmoid disease or previous surgery having a significant underlying pathologic process.

A and B, Bone and soft tissue windows from coronal sinus CT examination performed in a 60-year-old man with chronic nasal discharge reveals a soft tissue opacity filling the superior aspect of the right olfactory recess (arrow) adjacent to an apparent defect in the right cribriform plate. Subsequent otolaryngologic evaluation including endoscopy and surgical intervention confirmed the presence of an encephalocele, potentially related to a remote history of septoplasty.
Of the 122 patients in this study with completely clear paranasal sinuses on CT, none had bilateral ORO and only 1 (0.8%) showed unilateral ORO. The latter was the case of the aforementioned patient with an encephalocele confirmed at surgery.
Discussion
Our study evaluated the prevalence of ORO and characterized the circumstances in which it was typically seen. In an outpatient cohort undergoing sinus CT examination, the prevalence of ORO was 11.8% (6.4% unilateral and 5.4% bilateral). We found that rhinosinusitis significantly increased the likelihood of ORO. Because of the close proximity of the ethmoid air cells to the olfactory recess, inciting factors for ethmoidal inflammatory changes might equally be expected to result in mucosal thickening or retained secretions in the ipsilateral olfactory recess; however, we found it to be more common for the olfactory recess to remain patent despite nearby inflammation. In a similar fashion, patients who had undergone previous ethmoidectomy or turbinectomy were more likely to exhibit ORO. It is possible that the formation of postoperative scarring or granulation tissue may contribute to ORO by impeding drainage from this area. Alternatively, one can speculate that the postoperative anatomy itself may not increase the prevalence of ORO, as aeration of and drainage from the olfactory recess is typically improved. Instead, this association perhaps reflects a surrogate marker for patients who required surgery for severe rhinosinusitis, rather than a true causal relationship. Conversely, unilateral ORO seems to be exceedingly rare in patients with completely clear paranasal sinuses (0.8%), and the only case of unilateral ORO seen in these circumstances in this series was surgically confirmed to represent an encephalocele.
We hypothesized that the presence of a concha bullosa would increase the likelihood of ipsilateral ORO because of decreased volume of the nasal cavity passages. Although published reports are variable, a recent study reviewing more than 1000 paranasal sinus CT scans concluded that there is no increased incidence of sinus disease in patients with concha bullosa.10 It is noteworthy that, because of deviation of the nasal septum away from the unilateral or dominant concha bullosa, the adjacent air channel tended to be preserved. Maintenance of this nasal air channel between the medial aspect of the concha bullosa and the adjacent surface of the nasal septum may explain the lack of an association between ORO and concha bullosa in our study.
A body of literature exists on the topic of unilateral paranasal sinus opacification,11–14 focusing on the need for close clinical and imaging scrutiny to detect a pathologic process beyond routine rhinosinusitis. With extrapolation of this to the olfactory recesses, the detection of unilateral ORO should raise suspicion for a significant pathologic condition unless seen in association with surgical anatomic changes or inflammatory sinus disease. Of the patients with unilateral ORO, 15.6% (5 patients) lacked such findings. One of these patients had an encephalocele confirmed on surgical treatment, whereas another had imaging features strongly suggestive of a cephalocele. Clinical follow-up is lacking on the remaining 3 patients, but although the sample size of this group is small, this still suggests a significant positive disease rate.
Bilateral ORO is thought unlikely to represent a significant incidental pathologic process in the absence of intervening osseous destruction or dehiscence. Specifically, neoplasms or cephaloceles large enough to result in bilateral ORO would be expected to have a readily apparent bone defect in the cribriform plate or perpendicular plate of the ethmoid bone, or both. As such, it would be unlikely to dismiss this extent of abnormality as subtle, nonspecific ORO.
Conclusion
Although ORO may be seen in the presence of adjacent ethmoid sinus disease or previous ethmoidectomy or turbinectomy, it is distinctly uncommon in the absence of these findings. Consequently, isolated unilateral ORO should be viewed as suspicious for an unsuspected pathologic process such as a small neoplasm or cephalocele and should prompt the radiologist and clinician to evaluate this area further.
Footnotes
Preliminary data previously presented at: Annual Meeting of the American Society of Head and Neck Radiology, September 22, 2005; San Francisco, Calif; and final results previously presented at: Annual Meeting of the American Society of Neuroradiology, June 11, 2007; Chicago, Ill.
References
- Received August 18, 2007.
- Accepted after revision December 24, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging Review of New and Emerging Sinonasal Tumors and Tumor-Like Entities from the Fourth Edition of the World Health Organization Classification of Head and Neck Tumors
- Intranasal Esthesioneuroblastoma: CT Patterns Aid in Preventing Routine Nasal Polypectomy
- CT Findings of Sinonasal Respiratory Epithelial Adenomatoid Hamartoma: A Closer Look at the Olfactory Clefts
- CT Assessment of Woodworkers' Nasal Adenocarcinomas Confirms the Origin in the Olfactory Cleft