
Abstract
SUMMARY: Esthesioneuroblastoma (ENB) is a malignant neoplasm of the olfactory epithelium. Metastasis of ENBs to retropharyngeal lymph nodes is an important finding on imaging examinations that alters staging and treatment. A total of 17 cases of ENB from 3 institutions were evaluated. The CT and MR imaging findings from the cases of 4 patients with ENB with retropharyngeal metastatic disease are reviewed. The vector of spread, staging, and treatment implications are discussed.
An esthesioneuroblastoma (ENB), also called an olfactory neuroblastoma, is a rare neuroendocrine malignant neoplasm of neural crest origin. The neoplasm almost invariably originates from the olfactory epithelium high within the nasal cavity. This highly vascular and resilient tumor has a known metastatic propensity to cervical lymph nodes and distantly to the thorax and skeleton.1 The incidence of cervical lymph node metastasis from a primary ENB has been reported to range from 10% to 44% in the literature.2 Only 2 other cases of retropharyngeal lymph node (RPLN) metastasis have been reported in the literature to date.3
This study is a retrospective case series of 4 patients seen at 3 separate academic institutions found to have pathologically confirmed retropharyngeal metastatic disease from an ENB. Inpatient and outpatient imaging records were reviewed from patients diagnosed with ENB. A total of 15 patients with ENB were found within our institutional archive during a 10-year period. Two cases of retropharyngeal metastasis were identified within our data base; 2 additional cases were submitted from outside institutions to bring the total number of patients evaluated to 17. All of the patients were either primarily treated at our institution, or the imaging studies were referred from an outside institution.
The cases of 4 patients with ENB with retropharyngeal metastases were then retrospectively reviewed. The cases included 2 women and 2 men, ages 47 years (patient 1), 44 years (patient 2), 68 years (patient 3), and 67 years (patient 4). In 3 patients, the positive nodes presented after craniofacial resection and radiation treatment, and in 1 patient, the node was found on initial presentation. In 3 patients, the right RPLN was involved, and in the fourth, a left lateral RPLN was identified.
Case Reports
A 47-year-old woman presented at our institution to a combined neurosurgery and head and neck surgery service with the chief complaints of recurrent headaches, chronic nasal congestion, and proptosis of the right eye. The MR examination performed on presentation to our center demonstrated a somewhat typical superior nasal vault lesion, with heterogeneous signal intensity on T2 and T1 images, which demonstrated avid enhancement. There was intracranial and orbital invasion (Fig 1A, -B) and peritumoral cysts at the tumor-brain interface (arrows, Fig 1B). Significant edema accompanied the intracranial extension, and encasement of intracranial vessels was noted.

A, Axial T2 MR imaging at the level of the hard palate shows an enlarged right lateral retropharyngeal lymph node (asterisk). B, Coronal T1 postgadolinium scan with fat saturation through the nasal cavity and orbits shows the large esthesioneuroblastoma with extensive orbital and intracranial invasion. The arrow shows a peritumoral cyst.
Routine evaluation of structures outside the brain and orbits showed an enlarged 18-mm right retropharyngeal lymph node. The patient underwent resection of the mass requiring bifrontal craniotomy, transfacial resection, and exenteration of the right orbit. An additional neck dissection was required to remove the right lateral RPLN.
The surgical specimen consisted of multiple soft tissue fragments, some containing bony fragments, and others attached to the dura mater. The lymph node measured 2.0 × 1.0 × 0.7 cm. Histopathologic study of the nasal cavity mass revealed a cellular tumor composed of uniform small cells with scant fibrillar cytoplasm and indistinct cell borders. Scattered mitotic figures are identified. The cells were arranged in a lobular pattern (Fig 2) with Homer-Wright Rosettes, consistent with the diagnosis of an ENB.

A relatively low magnification (100X) view of a retropharyngeal lymph node containing nests of tumor cells on the left half of the field.
The case of our second patient was that of a 44-year-old man who underwent previous craniofacial resection, radiation treatment, and chemotherapy 8 years before follow-up for a Kadish B ENB. He presented with palpable parotid and submandibular masses in addition to a right lateral RPLN surgically proved metastatic ENB (Fig 3A, -B.)

A, Axial contrast-enhanced CT through the level of the mandible demonstrates bilateral enhancing masses within the submandibular glands. B, Axial contrast-enhanced image of the skull base at the level of the hard palate shows an enhancing right lateral retropharyngeal lymph node (asterisk) and 2 enhancing left superficial parotid masses.
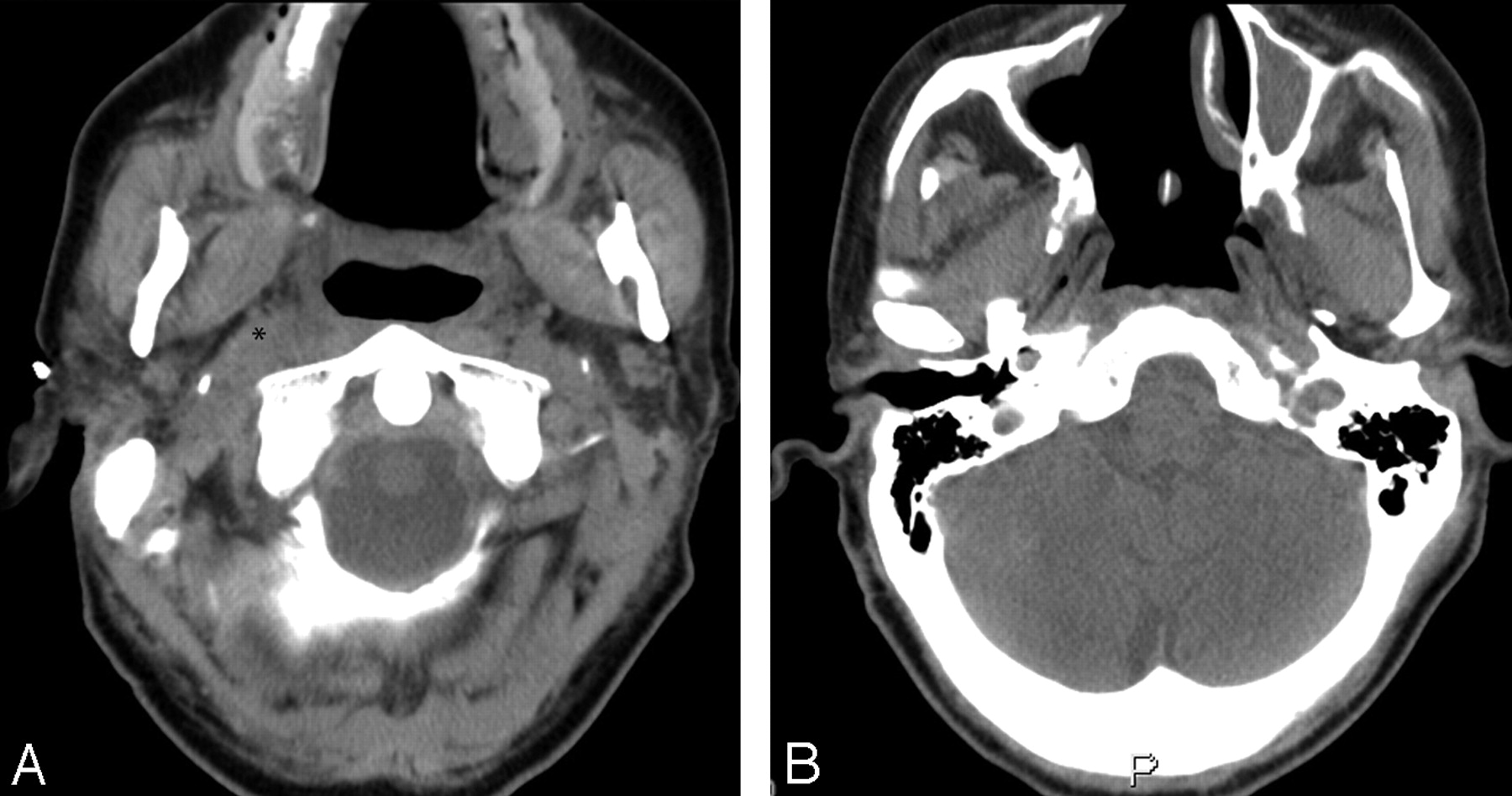
The third patient was a 68-year-old man with a previously diagnosed Kadish B ENB. He presented for CT follow-up 3 months after craniofacial resection. The noncontrast CT also demonstrated an enlarged right lateral RPLN (Fig 4A, -B.) Metastatic involvement was proved by fine-needle aspiration of the node.

A, Axial noncontrast CT image at the level just caudal to the hard palate demonstrates an enlarged right lateral retropharyngeal lymph node (asterisk) causing mass effect on the adjacent parapharyngeal fat. B, Axial noncontrast CT image of the skull base at the level of the torus tubarius showing the postsurgical changes within the nasal cavity and nasopharynx from craniofacial resection.
Our fourth patient was a 67-year-old woman with a history of an ENB resected in 1993 of unknown Kadish staging. She recently presented to a neurologist for memory loss. MR imaging obtained at an outside location at that time demonstrated an enlarged left lateral retropharyngeal lymph node. Repeat imaging was performed at our institution that confirmed the presence of an 8-mm enhancing left RPLN (Fig 5A) also seen on the first section of the series. A CT-guided biopsy was then performed (Fig 5B), which allowed confirmation of recurrence of disease at this location.

A, Axial T1 image with fat saturation obtained at the skull base demonstrating an enhancing left lateral retropharyngeal lymph node. B, Axial noncontrast CT image showing the percutaneous CT-guided biopsy results of the suspect left retropharyngeal lymph node.
Discussion
Infectious processes and carcinomas of the upper aerodigestive tract are well known to involve the lateral RPLNs. The route of disease spread to the lateral nodes was initially described by Rouviere4 in 1938. The lateral retropharyngeal lymph nodes receive drainage anteriorly via lymphatics draining from the incisive canal and nasal fossa to the soft palate, which then terminates at the lateral lymph nodes. A posterior route has also been described, which arises along the inner surface of the hard palate leading to the soft palate and on to the lateral nodes. Rouviere4 discovered crossing of lymphatic vessels along the hard and soft palates in 50% of his specimens, therefore providing an anatomic basis for contralateral spread of nodal disease.
The Kadish system,5 the classic staging system used to predict overall morbidity and mortality from ENB, does not specifically mention retropharyngeal metastatic disease. Stage A tumors are those confined to the nasal cavity. Stage B tumors extend from the nasal cavity to the paranasal sinuses. Stage C tumors extend into the orbit, base of the skull, or with intracranial extension.5,6 Other classifications have been proposed that specify which paranasal sinuses are involved, if there is extension into the cribriform plate, and the size of the tumor. Chao et al proposed a Kadish D stage that adds further distinction to ENB involving the cervical lymph nodes.6 The Kadish system and other classifications simply divide nodal disease roughly into local or regional disease.5-10
Regardless of the staging system used, metastasis from ENB portends a poor prognosis. Patients who are not cured by initial treatment eventually die from the recurrent disease, mainly from intracranial extension or distant metastatic disease.11,12 The 5-year survival rate of patients with cervical metastasis has been reported to be 0%, whereas the survival of those without positive distant metastasis was greater than 60%.2 The incidence of local or distant metastatic disease from primary ENB has been reported at ranges of 10% to 40% in different study populations.2 Recurrent metastatic disease to cervical lymph nodes has been reported in up to 18% of patients after initial treatment and up to 44% of patients with Kadish C disease at presentation.8-12 Cases 2 through 4 in our series represent locally recurrent disease within the lateral RPLNs, whereas in the first patient the lateral RPLN was found on initial presentation. No studies have been done concerning the rate of ENB metastasis to RPLNs specifically.
The spread to RPLNs has important staging and treatment implications in head and neck squamous cell carcinoma, but this issue has not been specifically reported in the English-language medical literature with regards to ENB.7 The standard treatment of ENB involves surgical resection, radiation, chemotherapy, or combined modalities. Combined treatment regimens have been most successful in rates of tumor recurrence and overall survival.6,11-15 The presence of metastatic disease to the RPLN, as in the case of our first patient, could require an additional surgical procedure.
Although the English-language literature has described these lesions with other head and neck pathologic processes, no previous publications have addressed the prognostic implications of metastatic retropharyngeal nodes from an ENB primary. Head and neck radiologists need to be vigilant because of the potential added morbidity, which has yet to be fully explored. In the cases of our 4 patients, the pathologic changes in the lymph nodes were often located on the first images of the axial datasets and were initially overlooked on routine MR evaluation of the brain in the case of our first patient.
References
- Received November 18, 2007.
- Accepted after revision February 6, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}