
We read with great interest the article by Fei et al1 in which symmetric paraventricular regions in MR imaging were shown to be useful in the diagnosis of nonalcoholic Wernicke encephalopathy (WE). Among clinical studies, MR imaging is currently considered the most valuable method for confirming a diagnosis of WE, though the typical findings of MR imaging are observed in only 58% of WE patients.2 To advance the clinical facility of MR imaging, we report a case of nonalcoholic WE in which symmetric paraventricular regions could be found before the clinical onset of WE.
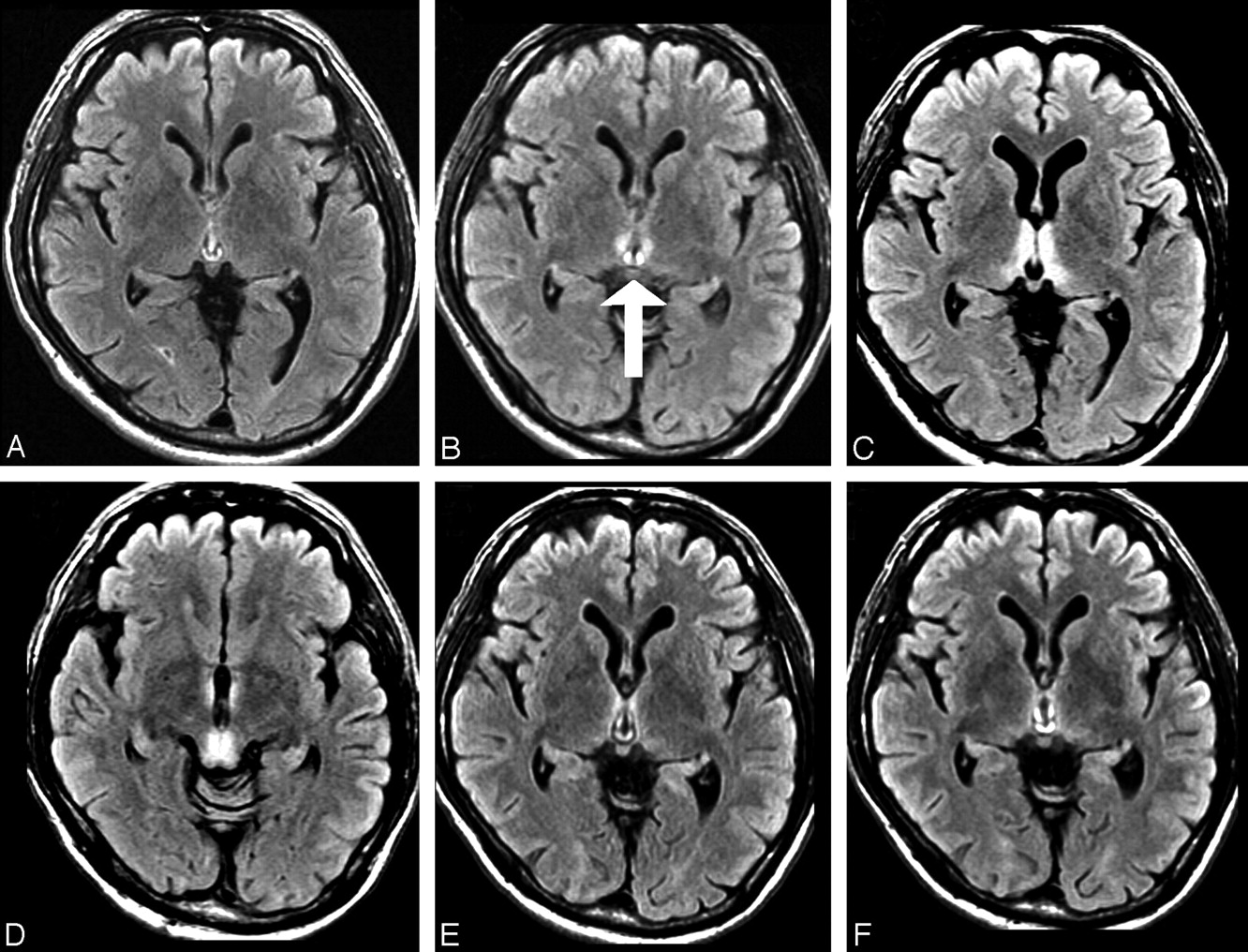
A 61-year-old Japanese man was admitted to our hospital because of impaired attention, gait disturbance, and double vision lasting for 2 days. He had undergone a partial gastrectomy because of gastric cancer 30 months before admission. He had no history of alcoholic abuse or unbalanced nutrition. He noticed transient amnesia and first came to our clinic 24 months before admission. However, there were no abnormal findings in his mental function or neurologic examinations. Brain MR imaging was normal (Fig 1A), and serum thiamine level was 61.1 μg/dL (normal, 2.0–7.2 μg/dL). After that, his symptoms abated; however, the second fluid-attenuated inversion recovery (FLAIR) MR imaging detected small symmetric paraventricular regions 6 months before the admission (Fig 1B).
Neurologic examination on admission revealed a confused state showing sensitivity to sound, oculomotor deficits, horizontal gaze-evoked nystagmus, and truncal ataxia. Routine blood examination and arterial blood analysis were normal. Serum thiamine level was markedly low, at 1.5 μg/dL. MR imaging clearly showed bilateral high-signal intensities over the mammillary bodies and paraventricular lesions in both T2-weighted and FLAIR modalities (Fig 1C, -D). Based on the diagnosis of WE, treatment with intravenous thiamine hydrochloride (500 mg/d) was promptly started. Neurologic manifestations were significantly improved in the following 2 days except for the impairment of recent memory. Thiamine administration for 7 days normalized serum thiamine to 10.9 μg/dL, and repeated brain MR imaging also revealed the diminishing of hyperintense lesions on FLAIR images (Fig 1E). Finally, 15 days after the start of treatment, he achieved normal scores in both the Mini-Mental State Examination and revised Wechsler Adult Intelligence Scale, and his final MR imaging could not detect any abnormal lesions (Fig 1F).
Nonalcoholic WE exhibiting complicated clinical manifestations and an atypical disease progression is prone to be underestimated.1,2 Gastric surgery is known to be one of the predisposing factors of WE, which usually develops weeks or months after the operation.2 The present patient developed WE 30 months after partial gastrectomy without episodes of vomiting or parenteral nutrition. In this regard, Karapanayiotides et al3 reported that a 53-year-old man showing restricted dietary intake and repeated vomiting developed WE 28 years after gastric surgery. In addition, bariatric surgery, commonly performed in the United States, is also a cause of WE, occurring between 4 and 12 weeks postoperatively, especially in young women with vomiting.4 Taken together, it is probable that nonalcoholic WE patients after gastric surgery have usually had antecedent episodes such as dietary restrictions, psychological food refusal, vomiting, and unbalanced total parenteral nutrition.1–4
Approximately 19% of WE patients have none of the typical triad of symptoms, including mental status changes, ocular abnormalities, and ataxic gait disturbance at presentation of WE.2 According to the review of Sechi and Serra,2 early detection of subclinical thiamine deficiency is generally difficult, because symptoms may be vague and nonspecific, such as headache, fatigue, irritability, and abdominal discomfort. In the present patient, however, it was impossible to determine that the transient amnesia at the first examination could really be ascribed to subclinical thiamine deficiency. When the “neuroradiologic” findings in MR imaging were first detected, we could not diagnose WE clinically for the following reasons. First, our patient had no antecedent events of alcohol overdrinking, unbalanced food intake, or vomiting. Second, he had recovered from amnesia, and there were no abnormal neurologic findings. Third, the level of serum thiamine was not low. In fact, he had been well with no treatments for 6 months until he was admitted to our hospital.
In conclusion, we present the chronologic changes of MR imaging before and after the onset of WE. It appears that MR imaging can predict the development of nonalcoholic WE. Thiamine supplementation should be initiated as soon as characteristic findings in MR imaging are seen, even if a clinical diagnosis of WE cannot be established.

Serial changes of MR imaging in a patient with nonalcoholic WE. Axial FLAIR images were obtained 24 months (A) and 6 months (B) before the onset of WE, on admission (C and D), and 7 days (E) and 15 days (F) after the start of treatment. Arrow indicates small symmetric paraventricular regions before the clinical onset of WE.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.