
Abstract
SUMMARY: A 33-year-old woman developed severe post–lumbar puncture headaches in the course of work-up for multiple sclerosis. Immediately after receiving treatment with intravenous caffeine, she became blind and experienced a generalized tonic-clonic seizure. Brain MR imaging then showed vasogenic parieto-occipital edema. She recovered clinically and radiologically within 72 hours. After 1 year of follow-up, there was no recurrence of symptoms or radiologic changes.
The clinical presentation of posterior reversible encephalopathy syndrome (PRES) is characterized by encephalopathy, seizures, headache, and visual abnormalities. From a radiologic standpoint, it is characterized by reversible vasogenic subcortical edema without infarction.1 It usually occurs in patients with underlying predisposing medical conditions (hypertension, malignant tumor, renal disease, postpartum state, and organ transplantation, among many others2,3) in whom a triggering factor (hypertensive emergency, eclampsia, chemotherapy [calcineurin inhibitors], or use of midodrine or ephedrine) can be identified.3 We here report a patient with post-dural puncture headaches (PDPH) in whom PRES was triggered by intravenous (IV) caffeine.
Case Report
A 33-year-old woman with no previous medical history presented with left-sided numbness and weakness over her left arm, leg, and face. Brain MR imaging revealed scattered white matter lesions on fluid-attenuated inversion recovery (FLAIR) sequences with no significant enhancement on T1 sequences after contrast injection, and she was admitted with a presumptive diagnosis of multiple sclerosis. Blood pressure was 110/70 mm Hg, pulse was 84 beats per minute, and she was alert and oriented. Initial neurologic examination showed only mild left hemiparesis with hypoesthesia and ipsilateral Babinski sign. Lumbar puncture was performed, and 12 cc of clear CSF were obtained, with an opening pressure of 140 mm/H2O. She was treated with intravenous (IV) methylprednisolone, 250 mg every 6 hours, and 2 days later her neurologic deficits were minimal. On the third day, she experienced severe postural headaches (not associated with neck rigidity, photophobia, nausea, or emesis), and a PDPH was diagnosed. Initially, the PDPH responded partially to a horizontal position in bed, IV hydration, nonsteroidal anti-inflammatory agents, and opioids. However, the next day her headache became constant and refractory. Treatment with IV caffeine was recommended at that time (500 mg of caffeine sodium benzoate, diluted in 1000-mL NS, administered for 4 hours), and blood patch was considered as the following therapeutic alternative. Two hours after finishing caffeine administration, the patient became confused and complained of increased headaches and blindness. On examination, there was no light perception, pupils were reactive to light, and there was no papilledema. Her blood pressure was 134/83 mm Hg and pulse was 92 beats per minute. Brain MR imaging was done immediately: FLAIR sequences showed edema in the occipital lobes (Fig 1A), and new enhancement of the parieto-occipital lobes as well as previously nonenhancing lesions was seen on T1 images with contrast. Her vision improved spontaneously after the MR imaging examination, but 1 hour later she experienced a generalized tonic-clonic seizure, which resolved after IV administration of lorazepam and phosphenytoin.

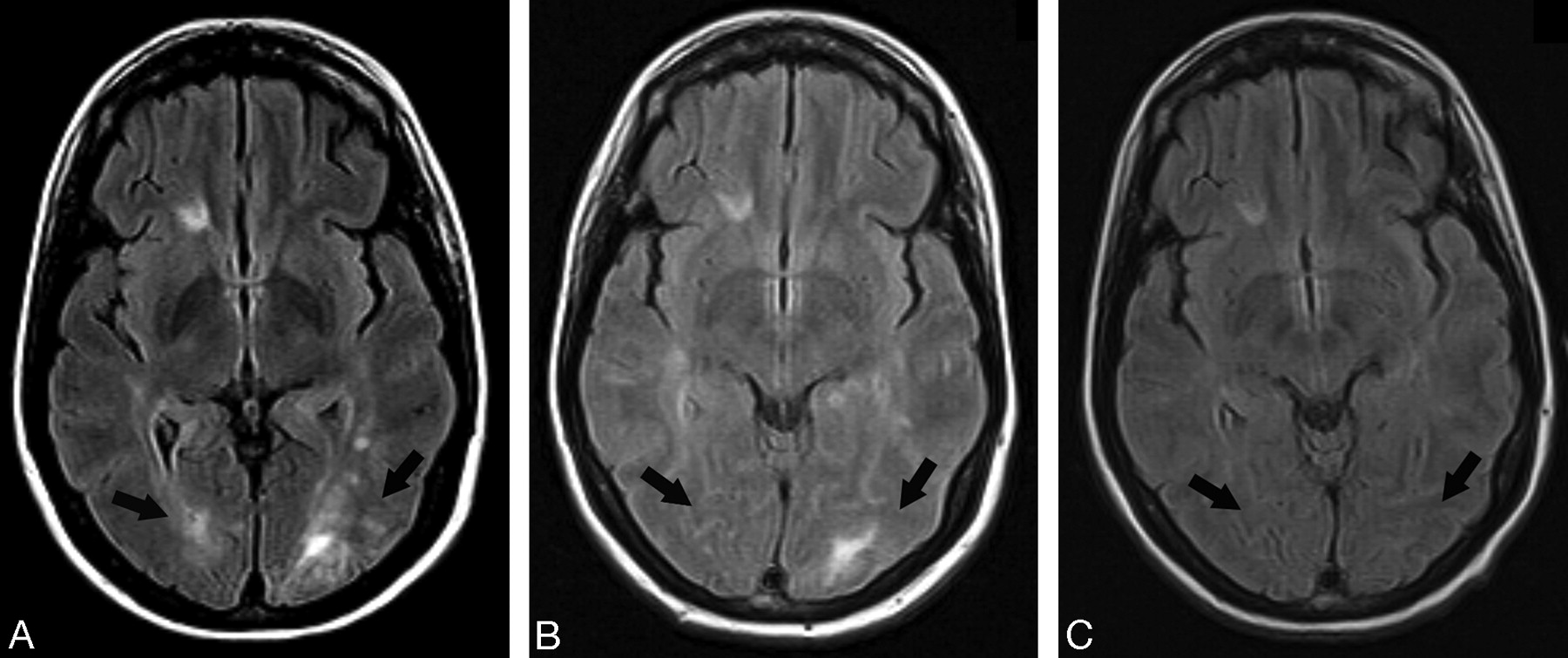
Brain MR imaging, comparison of axial FLAIR images. A, Brain MR imaging immediately after IV administration of caffeine, showing bilateral hyperintense signal intensity in the white matter of the occipital lobe, indicative of vasogenic edema (arrows). B, Follow-up brain MR imaging 72 hours later. There is resolution of the hyperintense signal intensity over the right occipital lobe and significantly reduced hyperintense signal intensity over the left occipital lobe, indicative of resolving vasogenic edema in both occipital lobes (arrows). C, Brain MR imaging 1 year later showing no hyperintense signal intensity in the posterior lobes (arrows).
The following morning, her headaches had resolved and her vision was normal. EEG was normal.
All treatments, except antiepileptic drugs, were stopped. She remained in bed at rest for 24 hours, and she was able to get up and ambulate without any headaches.
Follow-up brain MR imaging examination 72 hours later showed no enhancing lesions and near-resolution of the edema in the posterior lobes (Fig 1B). She was discharged after 10 days of hospitalization with no recurrence of headaches or seizures.
One year later, follow-up MR imaging examination did not show any signs of edema or abnormal enhancing in the posterior lobes (Fig 1C). She has remained asymptomatic since then and has been receiving treatment with interferon-beta for multiple sclerosis.
Discussion
The common denominator in PRES seems to be the presence of conditions that tend to provoke endothelial dysfunction leading to increased blood-brain barrier permeability or change in cerebrovascular autonomic control, or both. In this setting, a trigger factor, such as an increase in systemic blood pressure, generates segmental vasogenic edema.2,4 Despite the good overall prognosis, this condition is not completely benign because of the potential for bleeding into the lesion of reversible posterior leukoencephalopathy syndrome, as in cases of hypertensive encephalopathy. Also, there are atypical cases that may take longer than usual to reverse or may not be completely reversible.3,4
PDPH is believed to be caused by a CSF leak leading to intrathecal hypotension and reflex dilation and distention of the intracranial blood vessels, which are sensitive structures. This vasodilation has been shown to be asymmetric comparing posterior versus anterior circulation and also right versus left side.3,5
IV caffeine, probably by induction of vasoconstriction of the cerebral vasculature, has been documented to be an efficacious treatment of PDPH in many studies, without significant adverse effects.6,7 It is commonly used as first-line treatment because it is a less invasive technique than the epidural blood patch.
Multiple sclerosis may have been a predisposing condition to increased permeability in our patient, which, in combination with possible increased perfusion secondary to PDPH, could have been a favorable setting for IV caffeine to trigger a further asymmetric increase of local perfusion. The use of steroids may have also cooperated through fluid retention.
Why this phenomenon does not occur in many patients treated with IV caffeine for PDPH is probably because of the absence of an underlying predisposing condition, or perhaps PRES is underdiagnosed, as in the so-called postpartum seizures after treatment with IV caffeine reported in the medical literature before the more recent description of PRES.8–11 With this case report, we suggest adding multiple sclerosis and PDPH to the list of possible predisposing factors and IV caffeine to the list of trigger factors for PRES.
References
- Received July 22, 2008.
- Accepted after revision August 11, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}